


1Doctoral Program in Medical and Surgical Sciences, Complutense University of Madrid, 2Dermatology Department, Clínico San Carlos University Hospital, 3Dermatology Department, MD Anderson Cancer Center Madrid and 4Dermatology Department, Infanta Cristina University Hospital, Madrid, Spain
In the absence of guidelines recommending routine total-body skin examination, patient concern remains the main factor in seeking consultation regarding suspicion of skin cancer. This study explores gaps in patients’ understanding of malignant skin lesions, through the factors associated with incidental skin cancer. Included patients had a confirmed histological diagnosis of basal cell carcinoma, squamous cell carcinoma or melanoma. Tumour characteristics, patient demographics and other risk factors related to the development of skin cancer were obtained from each participant. The main measure was incidental skin cancer detection, using both binary logistic regression and Chi-squared Automatic Interaction Detection (CHAID) algorithm. Of the total tumours, 26.6% were detected incidentally. The following variables: male sex, living alone, long-axis diameter, tumour location, symptoms and time of disease evolution were independent predictors of incidental skin cancer. According to the CHAID algorithm, the most significant risk factor for incidental skin cancer was the absence of symptoms at diagnosis.
Key words: early diagnosis; incidental findings; projections and predictions; skin cancer.
Accepted Jul 1, 2021; Epub ahead of print Jul 5, 2021
Acta Derm Venereol 2021; 101: adv00498.
doi: 10.2340/00015555-3862
Corr: Álvaro Iglesias-Puzas, Dermatology Department, Hospital Universitario Clínico San Carlos, c/ Profesor Martín Lagos, s/n, ES-28040, Madrid, Spain. E-mail: alvaroigpu@gmail.com
Incidental skin cancer diagnosed in routine dermatology consultations represents a significant proportion of the total diagnosed. This study contributes to current strategies to improve early diagnosis of cancer, by highlighting factors that can trigger or act as barriers to skin cancer detection and seeking consultation. Incidental skin cancer appears to be related to both patient and tumour characteristics, with symptoms, time of evolution, family history of skin cancer, sex and living alone being the major contributors to patients taking notice of any changes or newly appearing skin lesions.
Skin cancer has become a global health problem. Despite numerous prevention initiatives and strategies for raising awareness among the general public, the incidence of skin cancer continues to increase (1, 2). In recent decades, basal cell carcinoma, squamous cell carcinoma and melanoma have reached epidemic proportions. Total annual cases now outnumber the combined total for lung, colon, breast and prostate cancer (1, 3, 4).
Early detection and treatment of skin cancer is related to a decrease in morbimortality and costs associated with the treatment of the illness in its advanced stages. However, prevention strategies based on screening the population (focused particularly on melanoma) have not been demonstrated to reduce the mortality and morbidity related to skin cancer (2 ,3, 5). Given the lack of clear recommendations for screening, physical exploration and clinical history of changes continue to be key in the detection of skin neoplasms, despite the in vivo diagnostic techniques now available (5).
There is clear evidence that exploration of the surface of the skin, either by a doctor or by patients themselves, is effective in the diagnosis of skin cancer (6, 7). However, few studies have focused on assessing how patients come to detect and consult their doctors about these lesions (8). Understanding of the reasons for a skin-cancer patient’s first encounter with the health system could serve as a way of determining where to focus specific efforts to improve the results of interventions for skin cancer (9). The aim of this study is to determine what factors are related to a malignant lesion going unnoticed by the patients themselves and being detected incidentally. Risk stratification to enable targeted screening of those individuals at high risk of developing an unsuspected skin cancer may improve the value of early detection initiatives.
Study design and data collection
An observational, cross-sectional, descriptive study was carried out in 3 hospitals in the Madrid region from November 2020 to March 2021. The study included 2 hospitals under direct public management and 1 private hospital, in order to better represent the existing resources for skin cancer diagnosis in Spain. Hospital Clínico San Carlos and Hospital Universitario Infanta Cristina are public hospitals that only treat patients referred from primary healthcare centres, while Hospital MD Anderson Cancer Center treats patients with a private health insurance scheme, and thus does not require an external referral. Referrals from other healthcare professionals to the dermatologist within the same hospital are possible for all 3 centres. The study was approved by the Ethics and Clinical Research Committee of Hospital Clínico San Carlos, and received informed consent from all participants. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for a descriptive study were followed (10).
The included patients were over the age of 18 years, with a recent histologically-confirmed diagnosis of basal cell carcinoma, squamous cell carcinoma or melanoma. Patients with cognitive, memory or serious sensory impairment, or any other condition that could prevent them from noting the presence of a skin tumour were excluded from the analysis. If more than one skin cancer was detected at the time of consultation, only the tumour that led to the consultation, or the first to be detected incidentally, was included in the study. Three dermatologists, who provided general dermatology consultations, took part in the study. They carried out a physical examination in response to the reason for each patient’s consultation, which thus varied according to each researcher, his or her age or personal history, but without being required by protocol to carry out a complete exploration of all the subjects (11). The following data were taken from each of the patients: type of tumour, its size, location, period of evolution, presence of associated symptoms, and whether the lesion was the reason for the consultation or was detected incidentally. All lesions that were not the reason for the main consultation, as well as the tumours diagnosed by other healthcare professionals (the general practitioner, other specialists, nursing staff) during a healthcare consultation carried out for another reason, are all considered incidental, provided that they were not detected previously by the patient. Demographic data were also collected (age, sex, marital status, level of studies, employment and family situation), as well as other risk factors related to the development of skin cancer, such as the existence of family or personal history with respect to skin cancer, sunburn and immunosuppression.
Statistical analysis
Data were analysed using SPSS program version 23.0 (SPSS, Chicago, Illinois, USA) and SPSS modeler version 18.0 (SPSS, Chicago, Illinois, USA). Descriptive analysis of the data was carried out by the distribution of frequencies for qualitative variables; mean values and standard deviation were calculated for quantitative variables (age, tumour size and variables were used as continuous variables). The resulting variable was how the skin cancer was first detected (incidentally during any exploration/by the patients themselves or people close to them). For logistical regression analysis, the association between the form of detection of the study variables was initially analysed using univariate analysis. All the variables associated significantly with incidental detection of a skin cancer in the univariate analysis were included in a model of binary logistical regression adjusted for confounding factors. Model performance was assessed by the change in the area under the curve (AUC).
The Chi-squared Automatic Interaction Detection (CHAID) algorithm was also used to evaluate the interaction of the most relevant characteristics from the protocol with incidental detection of skin cancer. CHAID was selected for this study due to its inherent advantages over traditional statistical approaches, such as a classification tree technique, in which the most influential variable divides the entire sample into 2 or more subgroups, which are subsequently divided at each step until there are no more significant risk factors (12, 13). The minimum parent and child nodes were determined as 30 and 25, respectively, in order to overcome the rule of thumb (or stopping rule) for the growth of the tree (14). A receiver operating characteristic (ROC) curve was drawn from the predictive probability and AUC calculated. A p-value < 0.05 was considered the level of statistical significance for all analyses.
A total of 406 patients with skin cancer were included consecutively (33 melanomas, 271 basal cell carcinomas, and 102 squamous cell carcinomas). Of the total, 52.2% were men and the mean age of the participants was 69.3 ± 14.7 years. The proportion of tumours detected incidentally was 26.6%, 76.9% of them being detected by dermatologists and 23.1% by other healthcare professionals. No relevant differences were found regarding patients and disease according to the hospital and model of care. Data concerning the clinical and demographic characteristics of patients included are summarized in Table SI.
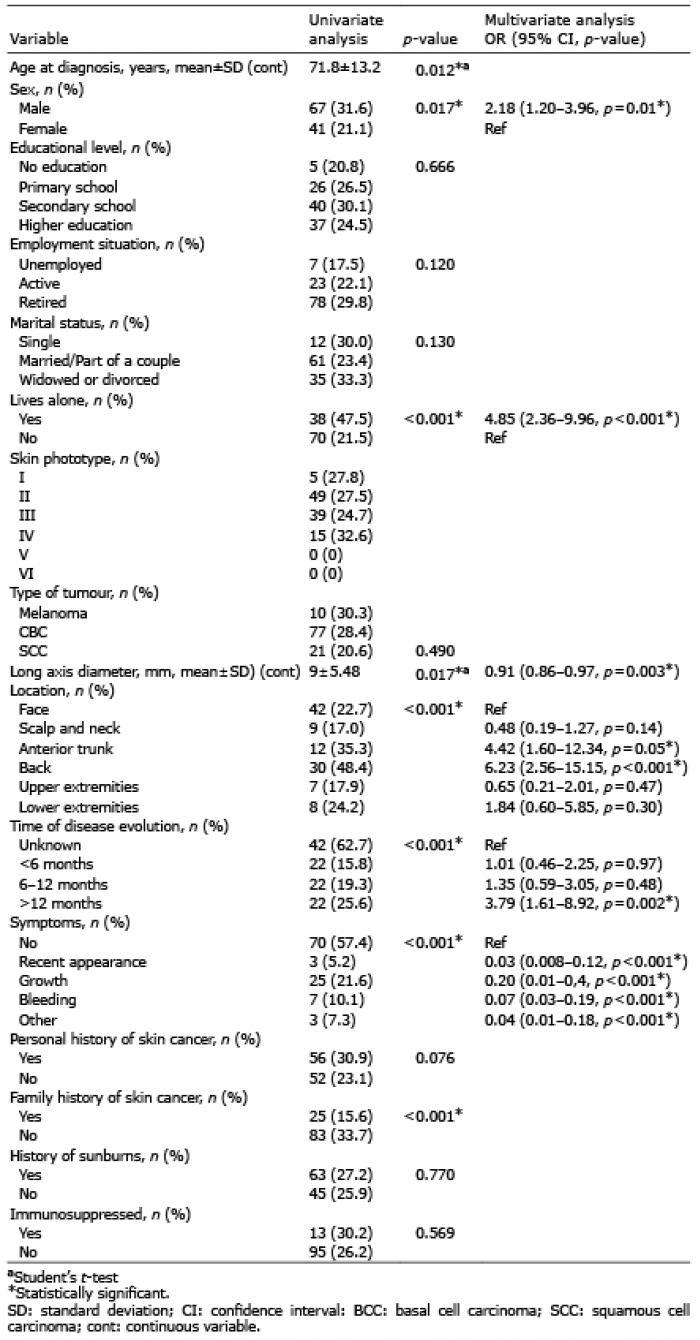
On a binary logistic regression, after adjusting for potential clustering and confounding effects, the variables: sex, living alone, long axis diameter, tumour location, time of disease evolution and symptoms were independent predictors of incidental skin cancer (Table I). The Hosmer–Lemeshow χ2 value was 9.906 (df=8), with a non-significant p-value of 0.272, which indicates that the model was well-fitted. The area under the ROC curve was 0.88 (95% CI 0.85–0.92, p < 0.001) (Fig. 1).
Table I. Univariate and multivariate analysis of prognostic factors of incidental skin cancer
Fig. 1. Receiver operating characteristic (ROC) curves of the established models. (A) and (B) represent the development data of the logistic regression model and the CHAID model, respectively. AUC: area under the curve; 95% CI: 95% confidence interval.
CHAID analysis was conducted on the 406 patients. The absence of symptoms was the most important predictor of incidental skin cancer. For asymptomatic patients, living alone and a lesion of unknown evolution increased the risk of incidental skin cancer. In the case of symptomatic tumours, family history, not living alone and female sex decreased the risk (Fig. 2). The model had 81.53% accuracy and the area under the ROC curve of the CHAID tree was 0.81 (95% CI 0.77–0.86, p < 0.001) (Fig. 1).
Fig. 2. Chi-squared Automatic Interaction Detection classification tree analysis to identify the predictors related to the development of incidental skin cancer.
Approximately 27% of skin cancers in the study sample were incidental and would otherwise have been missed without an in-person skin examination by a dermatologist (15). Despite tumours being on the skin surface and thus potentially detectable, malignant lesions frequently remain unsuspected by patients who do not seek consultation (16). Considering that identifying one’s own malignant lesion is not always an easy task, the results of the current study provide some interesting insights into skin examination behaviour, delay in detection, and factors associated with incidental skin cancer. Men and people living alone were more likely to ignore malignant lesions, which supports the active role that women, relatives and other cohabitants play in the discovery of skin cancer. Increasing men’s awareness of their skin, by encouraging them to take notice of any changes or newly appearing skin lesions, has the potential to reduce skin cancer morbidity and mortality (4, 17).
Consistent with previous studies, the most common anatomical location among all incidental malignancies was the face (38.9%), an area considered easily self-observable (18). The next most frequent body location was the back (27.8%), a region of the body not typically visible. Moreover, small-diameter lesions increased the risk of remaining unsuspected (odds ratio (OR) 0.91 (95% confidence interval (95% CI) 0.86–0.97) p = 0.003). These findings may be related to failure to identify lesions of concern, whether due to a low rate of performing a complete self-skin examination or the lack of patient awareness of skin cancer (18). Earlier detection of skin cancer may improve through education of patients and healthcare professionals on warning signs of skin cancer and ‘’easy to miss’’ locations.
Interestingly, a few of the common skin cancer risk factors were not associated with patient detection in univariate analyses or did not remain independently significant in the multivariable analysis. The first of these was age, which has been related to reduced patient concern about malignancy, both due to a diminished visual acuity or to a general indifference regarding the medical condition (19). The second was personal history of skin cancer. Although 44.6% of participants reported removal of a malignant lesion in the past, this did not translate into a significant reduction in incidental skin cancer (p = 0.076). These findings may represent a lower perceived likelihood of developing a second skin cancer among participants, while fitting with previous observations that this perception can persist even if patients have experienced treatment (7, 17).
Another interesting finding is that, even if the proportion of skin cancer in the index lesions parallels the overall distribution, conventional statistics did not find significant differences between incidental detection and the different types studied (p = 0.276). This raises the question as to what existing differences in patient’s or tumour characteristics, whatever its type, are essential to avoid a malignant lesion remaining unsuspected. While it is true that the lack of symptoms and time of disease evolution are responsible for a significant proportion of cases, it is noteworthy that CHAID analysis showed that 3 out of the 5 major contributors to incidental skin cancer detection were patient related (Fig. 2). Detection of incidental skin cancers may be enhanced through consideration of patients’ sex, environment and family history of skin cancer, which are established and readily identifiable risk factors.
This study has several limitations. Patients were included during the COVID-19 pandemic, which could have decreased incidental skin cancer detection due to a negative tendency in seeking consultation for non-malignant concerns, and in performing preventive examinations. The study was developed according to routine clinical practice; hence patients could have specifically requested total body skin examination at the time of the visit, limiting the providers’ influence on the decision to perform this examination (20). If a patient presented with 2 incidental skin cancers at the time of consultation, the study included only the first detected, which may introduce some bias in terms of examination patterns among the different dermatologists and the location of the first tumour diagnosed. Although incidental skin cancer would have probably been detected at a later stage, analysis of subsequent morbidity and mortality is beyond the scope of this study. Finally, the resulting predictive model was simple, and the pool of included patients specifically examined the differences in incidental detection rates between patients with skin cancer. Although this study included patients seeking care in public and private settings and the sample size is satisfactory, the results may not be generalizable to other countries or healthcare systems. However, further risk stratification using these common variables may improve the ability to identify otherwise low-risk asymptomatic patients for whom screening is of highest value in other countries (20, 21).
These data highlight patient understanding of skin cancer, as well as the differences in patient demographics and tumour characteristics regarding the detection process. Incidental skin cancer appears to be related to both patient’s and tumour characteristics, with the absence of symptoms and living alone being the main factors for not noticing any changes or newly appearing skin lesions and therefore not seeing a doctor. Dermatologists and non-dermatology practitioners should be aware of the importance of a thorough examination in addition to examining the lesion leading to the consultation. In the absence of clinical guidelines to recommend routine total-body skin examination, patient characteristics should be combined and interpreted in the context of reducing the possibility of skin cancer remaining undetected, even after an in-person examination (18).
The authors thank the members of the Methodological Research Support Unit of San Carlos Health Research Institute (IdISSC) for their help with statistical analysis.
Ethical approval was received from the Hospital Clínico San Carlos Institutional Review Board (Number 20/141).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize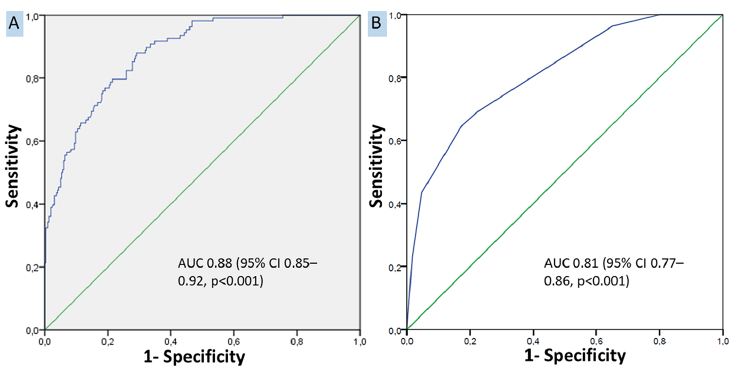 Click to show fullsize
Click to show fullsize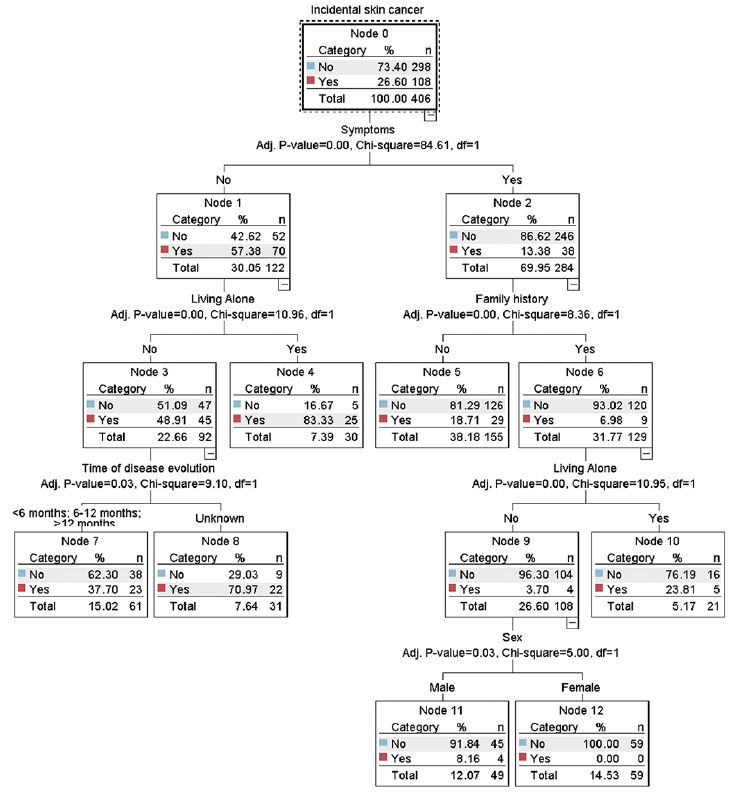 Click to show fullsize
Click to show fullsize