


1Department of Dermatovenerology, Medical Faculty University of Rijeka, Clinical Hospital Center Rijeka, Krešimirova 42, HR-51000 Rijeka and 2Department of Anesthesia, Resuscitation and Intensive Care, Medical Faculty University of Rijeka, Clinical Hospital Center Rijeka, Rijeka, Croatia. *E-mail: larisa.prpic@medri.uniri.hr
Accepted Jul 1, 2021; Epub ahead of print Jul 5, 2021
Acta Derm Venereol 2021; 101: adv00499.
doi: 10.2340/00015555-3863
Lichen planus is a chronic inflammatory mucocutaneous disorder commonly affecting the skin, nails, hair, and mucous membranes (1). Although its main cause is still unclear, lichen planus is defined as a T cell-mediated inflammatory disease (2). CD8+ T lymphocytes activate their cytotoxic armamentarium and induce basal keratinocyte apoptosis (2). The susceptibility of basal keratinocytes to CD8+ T lymphocytes is enhanced through MHC class I expression on keratinocytes triggered by interferon (IFN)-gamma (3). The cytotoxic process is mainly mediated by the release of lytic molecules, such as perforin, granzyme B, and granulysin (GNLY) (4–8). The upregulation of perforin and granzyme B has been previously demonstrated in the peripheral blood and lesional skin of patients with lichen planus (4–8). GNLY is a member of the saposin-like lipid-binding protein (SAPLIP) family and has a cytotoxic effect on tumour cells and a variety of microorganisms (9, 10). It is located in the cytotoxic granules of T cells, which are released upon antigen stimulation, and in the cytotoxic granules of natural killer (NK) cells. GNLY presence has only recently been observed in lichen planus lesions, but the expression level of this molecule in peripheral blood and subsequent determination of cells that express this molecule in blood and lesions remains unknown (8). In this study we examined the dynamics of GNLY expression in different cytotoxic subtypes of peripheral blood lymphocytes and in the skin lesions of patients with lichen planus.
A total of 30 patients (age 31–70 years, mean age 56 years) with clinically defined and histopathologically confirmed lichen planus were included in study. The control group comprised 20 healthy volunteers, matched by age and sex with an examined group. The study was approved by the local ethics committee and all patients provided informed consent. Mononuclear cells were isolated from peripheral venous blood samples, then fixed, permeabilized and simultaneously labelled with conjugated monoclonal antibodies against surface antigens and GNLY molecule (anti-CD3, anti-CD4, anti-CD8, anti-CD56, anti GNLY; BD Biosciences, Erembodegen, Belgium) according to the protocol (11). Two skin biopsies were obtained from each patient; 1 from the inner border of the lichen planus lesions and the other from uninvolved skin at least 3 cm away from the affected skin. According to the protocol (11), the slides were blocked and then incubated with mouse anti-GNLY monoclonal antibody (Leica Biosystems, Novocastra, UK). Specific binding was detected using the EnVision/DAB+ System (DAKO, Glostrup, Denmark). Diaminobenzidine (DAB) was dispensed on the slides and the slides were then stained with monoclonal antibodies (anti-CD8, anti-CD56; DAKO, Glostrup, Denmark), followed by biotinylated secondary goat anti-mouse antibodies and streptavidin conjugated with alkaline phosphatase. Positive cells were counted under 400× magnification in 5 fields. The results are shown as a percentage of double positively stained cells among all CD8+ T lymphocytes and NK cells, respectively. Statistical analysis was performed using the Statistica 13.2 data analysis software system (StatSoft, Inc., Tulsa, OK, USA). Differences in the values of quantitative variables between the 2 groups were assessed using the Mann–Whitney U test, whereas differences between 3 groups were evaluated using the Kruskal–Wallis test. Statistical significance was set at p < 0.05. Data are presented as median values and as 25th/75th percentile.
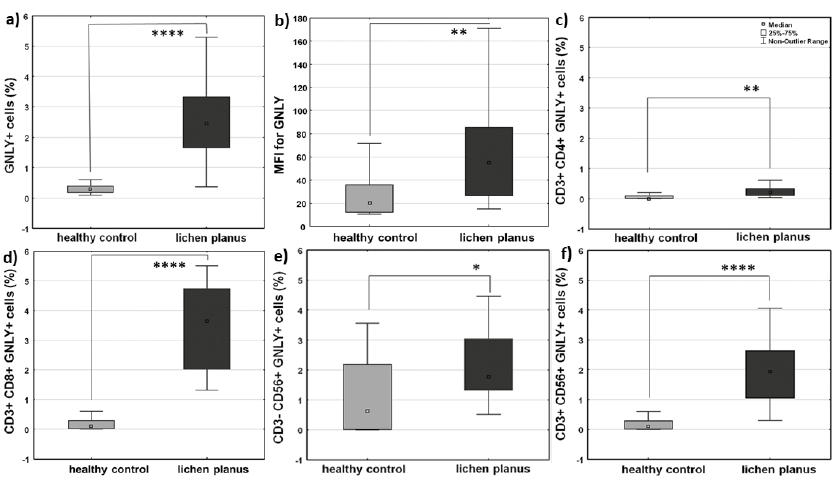
The frequency of GNLY+ cells and the mean fluorescence intensity (MFI) for GNLY (representing the mean number of molecules per cell) were higher in the peripheral blood of patients with lichen planus compared with the healthy individuals (Fig. 1a, b). Furthermore, the frequency of cytotoxic cell populations; that is, CD3+CD4+GNLY+ cells, CD3+CD8+GNLY+ cells, CD56+GNLY+ NK cells and CD3+CD56+GNLY+ NKT cells was also significantly higher in the peripheral blood of patients with lichen planus (Fig. 1c–f). Interestingly, the frequency of CD3+CD8+GNLY+ cells was 5 times higher than that of CD3+CD4+GNLY+ cells in lichen planus, suggesting the importance of CD8+GNLY+ cells in disease pathogenesis (Fig. 1c, d). In lesional skin, there was a significantly higher number of CD8+ cells expressing GNLY in both the epidermis and dermis compared with the complete absence of these cells in the epidermis and dermis of non-lesional and healthy skin (Fig. 2a–d). On the other hand, CD56+GNLY+ cells were not found in the epidermal compartment of lesional lichen planus skin, n or in the non-lesional and healthy skin (Fig. 2e). However, they were abundantly present in dermal lesional infiltrates (Fig. 2f–h), while absent in the dermis of non-lesional and healthy skin (Fig. 2f).
Fig. 1. Granulysin expression in peripheral blood lymphocytes and their cytotoxic subpopulations in patients with lichen planus (median values: 25th/75th percentile). Boxplots show (a) the percentage of granulysin (GNLY)+ lymphocytes, (b) mean fluorescence intensity (MFI) of granulysin, (c) CD3+CD4+GNLY+ cells, (d) CD3+CD8+GNLY+ cells, (e) CD3–CD56+GNLY+ NK cells, and (f) CD3+CD56+GNLY+ NKT cells in healthy volunteers (grey bar) and patients with lichen planus (black bar). Levels of significance: *p < 0.05, *p < 0.01, ***p < 0.001, ****p < 0.0001.
Fig. 2. Immunohistochemical evaluation of double-positive (GNLY+CD8+ and GNLY+CD56+) cells in lesional lichen planus skin compared with uninvolved skin and healthy skin. Frequency of CD8+GNLY+ T lymphocytes and CD56+GNLY+ NK cells in healthy skin (white bar) non-lesional skin (grey bar), and healthy skin (black bar) of patients with lichen planus in (a, e) epidermis and (b, f) dermis (median value – 25th/75th percentile) Levels of significance: *p <0.05, **p <0.01, ***p <0.001, ****p <0.0001. Tissue distribution of CD8+GNLY+ (c, d; magnification ×200 and ×400) and CD56+GNLY+ cells (g, h; magnification ×200 and ×400) in lichen planus lesional skin. Surface markers CD8 and CD56 are stained red and granulysin is stained brown. Double-positive CD8+GNLY+ cells and CD56+GNLY+ cells are stained with both colours and indicated by red arrows.
The most important event in the pathogenesis of lichen planus is the cytotoxic attack of immune cells on epidermal basal keratinocytes, leading to basal layer disruption (6). Mononuclear cells located close to apoptotic keratinocytes mainly consist of CD8+ T lymphocytes that express the cytolytic molecules perforin and granzyme B (5, 6, 12). Perforin is abundantly found in the epidermis of lichen planus lesional skin, and a significant correlation between the apoptotic index and perforin+ cells has been demonstrated (13). Granzyme B is predominantly expressed in the epidermis and dermal infiltrates, mainly in CD8+ T lymphocytes that undergo exocytosis (6). Immunoelectron microscopy has shown that granzyme B molecules are located in the intercellular space adjacent to apoptotic keratinocytes (6). However, the number of granzyme B+ cells is smaller in lichen planus lesions than in other skin diseases that are also characterized by vacuolar degeneration of the basal epidermal layer, supporting the hypothesis that cytolytic molecules other than granzyme B could also play a role in keratinocyte apoptosis (14).
GNLY has been detected in the skin lesions of Stevens–Johnson syndrome and toxic epidermal necrolysis, both of which are characterized by the vacuolar degeneration of basal keratinocytes (15). It is thus speculated that GNLY could serve as a key mediator of disseminated keratinocyte death (15). Ammar et al. (8) found a significant increase in the expression of GNLY mRNA in lesional lichen planus. In the current study we specified higher abundance of GNLY-expressing CD8+ T lymphocytes in both epidermis and dermis and GNLY-expressing NK cells in dermis in the lesional skin of lichen planus compared with non-lesional and healthy skin, supporting the hypothesis that GNLY could be involved in basal keratinocyte lysis. Systemic upregulation of the cytotoxic armamentarium, specifically of perforin, in the peripheral blood of patients with lichen planus, was demonstrated previously (7). In this study, for the first time, we showed elevated values of GNLY, especially in CD8+ T lymphocytes, CD56+ NK cells, and CD3+CD56+ NKT cells in the peripheral blood of patients with lichen planus than in the healthy controls, suggesting that peripheral blood is a good source of GNLY+ cytotoxic cells moving towards skin lesions.
In conclusion, the results of this study showed the prevalence of GNLY-expressing cytotoxic cells in the blood and lesions of patients with lichen planus. These results indicate that keratinocyte lysis mediated by GNLY could contribute to basal cell disruption and subsequent disease development, although the exact mechanism needs to be elucidated.
This work was financially supported by the University of Rijeka Foundation (grant number: biomed-uniri-18-43, investigator: Larisa Prpi? Massari, MD, PhD).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize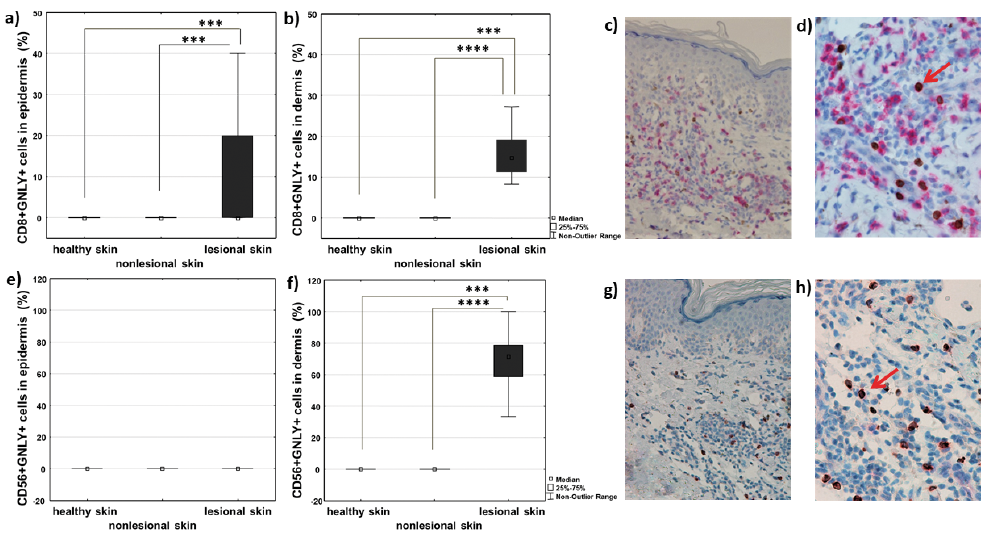 Click to show fullsize
Click to show fullsize