


1Department of Dermatology, Venerology and Allergology, HELIOS St Elisabeth Hospital Oberhausen, University Witten/Herdecke, Josefstrasse 3, DE-46045 Oberhausen, and 2Institute of Pathology, Mülheim an der Ruhr, Germany. E-mail: alexander.kreuter@helios-gesundheit.de
Accepted Jul 1, 2021; E-pub ahead of print Jul 5, 2021
Acta Derm Venereol 2021; 101: adv00500.
doi: 10.2340/00015555-3865
Cutaneous lupus erythematosus (CLE) comprises a heterogenous group of autoimmune skin diseases with a variety of clinical manifestations. Four different subtypes of CLE are currently distinguished, named acute CLE, subacute CLE (SCLE), chronic CLE (including discoid LE, chilblain LE, and LE profundus), and intermittent LE (LE tumidus) (1). Several trigger factors exist for CLE, including ultraviolet light, infections, drugs, and cigarette smoking. Moreover, solid tumours, especially lung and breast cancer, have been reported sporadically in association with CLE (2). In contrast, the occurrence of CLE in patients with haematological malignancies is very rare. We report here a case series of patients with previously unknown acute myeloid leukaemia (AML), myelodysplastic syndrome (MDS) or chronic lymphatic leukaemia (CLL), who presented with clinical and histopathological features of CLE. These lupus-like skin eruptions were associated with disease progression and poor outcome of the underlying haematological disease
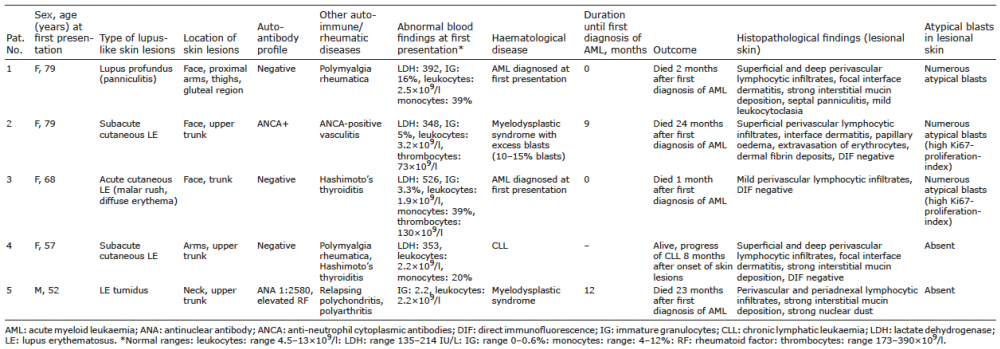
Between January 2015 and December 2020, 5 patients (4 women and 1 man, mean age at first presentation 67 years, range 52–79 years) were transferred to our department with a suspected diagnosis of CLE. All clinical, histopathological, and haematological characteristics of the patients are shown in Table I.
Table I. Clinical and haematological findings of patients with lupus-like skin lesions
Skin lesions and histopathology resembled SCLE in 2 patients and LE profundus, acute CLE, and LE tumidus in 1 case each (Fig. S1). All patients had at least 1 previous diagnosis of other autoimmune or rheumatic diseases (e.g. polymyalgia rheumatica or Hashimoto’s thyroiditis). Potential trigger factors for CLE were absent, except for cigarette smoking in patient 5 (Table I). None of the patients received medications known to cause drug-induced CLE (e.g. terbinafine, hydrochlorothiazide, or calcium-channel blockers). Moreover, standardized photoprovocation using ultraviolet (UV)A/UVB-radiation was negative in all patients. Serological analysis including antinuclear antibodies (ANA), anti-double-stranded DNA (anti-DNA) antibodies, and screening for extractable nuclear antibodies (ENA) revealed high ANAs (1:1250) in one patient (patient 5). However, none of the patients showed anti-DNA antibodies or CLE-specific ENAs.
It is notable that 3 patients (patients 1–3) had atypical blasts in the lupus-like inflammatory infiltrates, and additionally showed abnormal blood findings (e.g. immature granulocytes, elevated lactate-dehydrogenase, and monocytosis) at first presentation (Fig. S1). In 2 of them (patients 1 and 3), a diagnosis of AML was made, and both died within 2 months shortly after initiation of chemotherapy. In the other patient (patient 2), MDS with excess blasts was diagnosed 9 months after onset of skin lesions, and this patient died due to transition into AML 2 years after first diagnosis of MDS. In the 2 remaining patients (patients 4 and 5), atypical blasts or signs of leukaemia cutis were absent in the lupus-like skin lesions, but both of them had abnormal blood findings (Table I). In these 2 patients, a diagnosis of CLL (patient 4) and MDS (patient 5) was finally made. Similar to the other cases, lupus-like skin lesions were also associated with poor outcome of the underlying haematological disease.
It is well known that several rheumatic disorders may occur as paraneoplastic syndromes, for example dermatomyositis, inflammatory myopathies, rheumatoid arthritis, or vasculitides (3). CLE, specially SCLE, has been reported in association with malignancies such as cancer of the breast, colon, lung, or gastrointestinal tract (4, 5). In contrast, CLE or lupus-like eruptions have rarely been reported in patients with haematological disorders (6–8). Misri et al. (6) reported a 48-year-old woman with a lupus-like butterfly rash that histopathologically revealed superficial and perivascular infiltrates with admixed blast cells. AML was diagnosed 1.5 months before, and the patient died shortly after initiation of chemotherapy with cytarabine. Cedeno-Laurent et al. (7) reported a 52-year-old woman with lupus-like skin lesions clinically resembling both ACLE and SCLE. Histopathology showed interstitial and perivascular lymphocytic infiltrates with prominent interstitial mucin, but absence of atypical blasts. A diagnosis of AML was made, and chemotherapy with idarubicin and high-dose cytarabine was initiated, followed by bone-marrow transplantation. Thomas et al. (8) reported a 34-year-old woman with skin lesions resembling lupus erythematosus tumidus (LET). Histopathology showed perivascular and periadnexal lymphocytic infiltrates with lack of mucin but presence of atypical blasts. The patient was diagnosed to have mixed T/B-cell acute lymphoblastic leukaemia and experienced a complete remission after polychemotherapy followed by bone-marrow transplantation. None of the 3 patients had CLE-specific autoantibodies (6–8). These findings are in line with the characteristics of our patients, showing that women are predominantly affected, autoimmune serology is unremarkable in most cases, and occurrence of lupus-like skin lesions is associated with progression and poor outcome of the underlying haematological disease.
Lupus-like skin lesions of our patients and previously reported cases differ substantially from leukaemia cutis (LC). LC presents as erythematous papules, plaques, nodules or tumours, but clinical findings, as seen in our patients (e.g. facial malar rash with erythematous macules, such as in ACLE, erythematous annular or polycyclic lesions, such as in SCLE, or indurated subcutaneous nodules involving the arms, face, and buttocks, such as in LE profundus) have so far not been described in LC (9). Although a perivascular and periadnexal pattern of LC has been reported, deposition of mucin and interface dermatitis with vacuolar alteration in histopathology is usually missing in LC (10). Moreover, the vast majority of LC develop in individuals who are already diagnosed with leukaemia (9, 11).
LC most frequently occurs in patients with AML and CLL (11). Similarly, 4 of our patients had AML and one patient had CLL, indicating that these 2 types of leukaemia have a particular tendency for skin involvement. The occurrence of LC is associated with a poor prognosis, and up to 90% of patients die within the first year after a diagnosis of LC, especially patients with AML (9). This is in line with our observations. All except one (patient 4 with CLL) patient died within 2 years after first diagnosis of AML.
Autoimmune features, such as elevated ANAs, inflammatory arthritis, or polymyalgia rheumatica, have been described in up to 20% of patients with MDS or CLL (12). All of our patients presented other autoimmune/rheumatic diseases in addition to CLE lesions, indicating that autoimmune features also occur in AML.
In conclusion, this case series demonstrates that CLE or lupus-like eruptions can rarely occur as a first manifestation of a haematological malignancy, especially AML, MDS, or CLL. A paraneoplastic cause should be considered in older patients with such skin lesions, especially if other frequent triggers for CLE are absent and if autoimmune serology is negative.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize