


1Department of Dermatology and 5Department of Orthopedic Surgery, Seoul Metropolitan Government-Seoul National University (SMG-SNU) Boramae Medical Center, 2Department of Dermatology, Seoul National University Hospital, 3Clinical Research Center, SMG-SNU Boramae Medical Center, Seoul, and 4Department of Dermatology, Yeungnam University, Daegu, South Korea
#These authors contributed equally to this manuscript.
Knee disorders that compromise patients’ lower leg movements and self-care may put these patients at greater risk of onychomycosis. However, little is known about the prevalence of onychomycosis in patients with knee diseases. This study evaluated the prevalence and characteristics of onychomycosis in patients with knee osteoarthritis. A total of 520 consecutive patients with symptomatic knee osteoarthritis who visited the Department of Orthopedics for a potential knee surgery were evaluated for onychomycosis by PCR-based reverse blot hybridization assay. Of the 520 patients, 308 (59.2%) were diagnosed with onychomycosis. Age (p = 0.004), male sex (p = 0.015), and being barefooted (p = 0.031) were statistically significant risk factors for onychomycosis. Knee disease severity, based on Kellgren-Lawrence grade, was associated with severity of onychomycosis. The impairment of physical function and self-care caused by knee disorders may increase the prevalence of onychomycosis in these patients.
Key words: onychomycosis; knee osteoarthritis; nail disease.
Accepted Aug 17, 2021; Epub ahead of print Aug 18, 2021
Acta Derm Venereol 2021; 101: adv00526.
doi: 10.2340/00015555-3895
Corr: Seung Baik Kang, Department of Orthopedic Surgery, SMG-SNU Boramae Medical Center, 20 Boramae Road 5-gil. Dongjak-gu, Seoul 07061, Korea. E-mail: ossbkang@gmail.com
Onychomycosis is a common nail disease that can inflict a huge medical burden, especially in elderly individuals. However, onychomycosis is often considered trivial and underestimated. In this study, onychomycosis was diagnosed in more than half of the patients with symptomatic knee osteoarthritis. As life expectancy increases globally and chronic diseases, including knee osteoarthritis, become more prevalent, the close association of onychomycosis, both in prevalence and severity, with osteoarthritis, warrants a careful multidisciplinary approach, since early diagnosis and treatment leads to lower patient morbidity and medical costs.
Onychomycosis is the most common nail fungal infection, accounting for up to 50% of all nail disorders (1, 2). While the reported prevalence of onychomycosis in the general population varies, a literature study, by Sigurgeirsson & Baran (3), reported the mean prevalence of onychomycosis as 4.3%, based on 11 population studies conducted in Europe and the USA. Also, several recent large-scale studies suggest that this number is still underestimated, and that the true prevalence of onychomycosis may be much greater; approximately 20% (4–6). Although highly prevalent, onychomycosis is often considered trivial by patients, and even by physicians. However, fungal nail infection can not only spread to family members or others, but can also lead to more serious complications (7). Furthermore, onychomycosis can cause significant physical and psychosocial distress and have a serious impact on quality of life (8). Overall, onychomycosis is an easily neglected disease that imposes a huge medical and economic burden on the healthcare system (9).
Increasing age is an indisputable risk factor for onychomycosis, as highlighted in numerous studies (10–13), whereas male sex and systemic comorbidity, such as diabetes, have also been suggested as risk factors by multiple studies (11, 12, 14). In elderly patients, comorbidities that limit physical function and self-care ability can be harmful in terms of both prevalence and treatment of onychomycosis (15–17). Knee osteoarthritis (OA), along with stroke, depression, and heart disease, is a disorder that causes the most significant physical disability (18), and is a prominent cause of self-care limitations (19). Patients with symptomatic knee OA have poorer flexibility and decreased knee range of motion (20), and limited joint mobility can affect the prevalence of podiatric disease, such as diabetic foot ulcer (21). We hypothesize that these mobility limitations could also affect the prevalence of onychomycosis. Nevertheless, there is a lack of studies evaluating knee OA and onychomycosis together.
The aim of the current study was to evaluate the prevalence and characteristics of onychomycosis in patients with knee OA.
Participants
Subjects were recruited at Seoul Metropolitan Government-Seoul National University (SMG-SNU) Boramae Medical Center, a secondary teaching hospital, from August 2018 to August 2019. A total of 520 consecutive patients with symptomatic knee OA who visited the Department of Orthopedic Surgery for a potential knee surgery were included in the study.
This study was reviewed and approved by the Institutional Review Board of SMG-SNU Boramae Medical Center (IRB number 20-2018-29).
Study design and data collection
At the baseline visit to the orthopaedic clinic, the following baseline demographics and clinical data were collected in a standardized questionnaire: sex, age, height, weight, duration of knee disease, and environmental factors potentially associated with onychomycosis (tendency to wear tightly fitting shoes, history of toenail trauma, tendency to be barefooted, frequent use of a public sauna or swimming pool, and regular participation in exercise). Systemic comorbidities, such as diabetes, hypertension, dyslipidaemia, and hypothyroidism, as well as orthopaedic comorbidities (hallux valgus, spinal stenosis, herniated intervertebral disc (HIVD), spondylosis, spondylolisthesis, and degenerative scoliosis/kyphosis), and knee clinical scores (Western Ontario & McMaster Osteoarthritis Index (WOMAC) score (22), Hospital for Special Surgery (HSS) scale (23), Knee Society Score (KSS) (24), and Tegner Activity Scale (TAS)) (25), were also recorded. The severity of knee OA was evaluated based on the Kellgren-Lawrence grade (K-L grade) using standing anterior-posterior knee radiography (26).
Thereafter, each patient was evaluated by a dermatologist within 1–2 weeks, and the following demographic and clinical characteristics were collected: clinical signs potentially associated with onychomycosis (subungual hyperkeratosis, onycholysis, onychogryphosis, ingrowing nail, superficial leukonychia, proximal leukonychia, and total nail dystrophy), nail and feet comorbidities (corn, callus, wart, tinea pedis, and finger nail onychomycosis), and history of previous onychomycosis treatment. Tinea pedis and finger nail onychomycosis were diagnosed clinically by visual assessment. A toenail sample was collected from each patient from the nail that appeared to be most severely affected by onychomycosis based on clinical signs (when there was no sign of onychomycosis, the distal part of either big toenail was sampled). The nail samples were evaluated for onychomycosis using REBA Fungus-ID (M&D, Wonju, Korea), a PCR-based reverse blot hybridization assay (REBA) kit. A potassium hydroxide (KOH) test was also performed for all toenail samples and the findings were compared with the REBA results. For patients diagnosed with onychomycosis by REBA, the severity of the disease was calculated based on the Scoring Clinical Index for Onychomycosis (SCIO) (27). In SCIO, the severity is scored in numbers (1–30), with a higher index indicating more severe onychomycosis; systemic therapy is recommended if a patient has a SCIO score greater than 6. The SCIO score for each onychomycosis-positive patient was calculated using the SCIO electronic calculator (http://www.onychoindex.com).
Statistical analysis
Data were expressed as means ± standard deviations for continuous variables, and percentages for categorical variables. Student’s t-test or non-parametric Mann–Whitney U test was used for continuous variables, and Fisher’s exact test or Pearson χ2 test was used for categorical variables. Multivariate logistic regression analysis was conducted to identify risk factors for onychomycosis. For sensitivity and specificity calculation, REBA was used as the gold standard. Sensitivity was defined as the proportion of REBA-positive cases that also screened positive for the KOH test, and specificity was defined as the proportion of REBA-negative cases that also screened negative for the KOH test. p < 0.05 was considered statistically significant. Statistical tests were performed using IBM SPSS Statistics ver. 19.0 (IBM Co., Armonk, NY, USA).
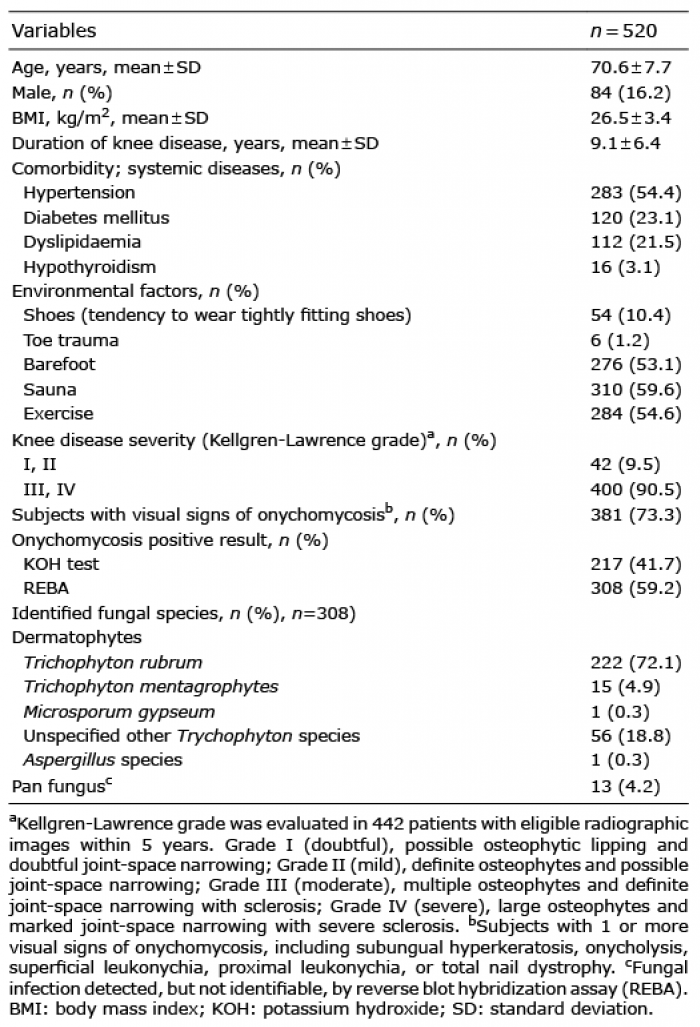
A total of 520 consecutive patients (84 (16.2%) male; 436 (83.8%) female) were included in the study. Their mean age was 70.6 ± 7.7 years (range 23–95) and mean duration of knee disease 9.1 ± 3.4 years. Mean body mass index (BMI) was 26.5 ± 3.4 kg/m2. The most common systemic comorbidity was hypertension (n = 283, 54.4%), followed by diabetes mellitus (n = 120, 23.1%), dyslipidaemia (n = 112, 21.5%) and hypothyroidism 16 (3.1%). Among the environmental factors, patients had a high tendency of using a public sauna or swimming pool (n = 310, 59.6%), participating in exercises regularly (n = 284, 54.6%), and being barefooted (tendency to wear slippers/sandals or shoes without socks; n = 276, 53.1%). K-L grade, a knee disease severity index based on a radiological imaging, was evaluated in patients who had adequate radiological images within a period of 5 years; the majority of the patients had advanced knee OA (K-L grade III or IV; moderate to severe) with 400 (90.5%) out of 442 patients having eligible radiographic images. Based on REBA, 308 (59.2%) patients were diagnosed with onychomycosis, and Trichophyton rubrum was the most frequently identified dermatophyte, with 222 (72.1%) patients. Detailed characteristics of the patients and the fungal species identified are listed in Table I.
Table I. General and clinical characteristics of the patients
A comparison of onychomycosis-positive and -negative patients with knee OA revealed age (p = 0.001), male sex (p = 0.046), hypertension (p = 0.041), being barefooted (p = 0.025), and HIVD (p = 0.041) as statistically significant predictors of onychomycosis (Table II). Subungual hyperkeratosis, concurrent tinea pedis and history of onychomycosis treatment were also statistically more frequent in onychomycosis-positive patients, while onycholysis was more frequent in onychomycosis-negative patients. A multivariate logistic regression analysis was performed to further evaluate the risk factors for onychomycosis; age (p = 0.004), male sex (p = 0.015), and being barefooted (p = 0.031) were the only statistically significant risk factors (Table II). Hypertension and regular participation in exercises were statistically significant in univariate analysis, but not in multivariate analysis.
Table II. Comparison of characteristics between onychomycosis-positive and -negative groups and logistic regression analysis on risk factors for onychomycosis
The association between knee disease severity indices and onychomycosis severity index (SCIO) (27) was evaluated among the patients diagnosed with onychomycosis. A statistically significant association was found between K-L grade and SCIO (p = 0.016) when the knee OA group was divided into doubtful to mild (K-L grade I and II) vs moderate to severe (K-L grade III and IV) groups (Table III). Notably, age and BMI were also higher in the patient group with moderate to severe knee OA. No such association was found between SCIO and other knee disease severity indices that evaluated the severity in continuous variables.
Table III. Association between knee osteoarthritis and onychomycosis severities in the onychomycosis-positive group
The sensitivity and specificity of the KOH test relative to REBA were also calculated. A moderate sensitivity (66.2%) and high specificity (93.9%) were found; positive predictive value (PPV) was 94.0% and negative predictive value (NPV) 65.7% (Table IV).
Table IV. Sensitivity and specificity of potassium hydroxide (KOH) test relative to PCR-based reverse blot hybridization assay (REBA)
Onychomycosis is a highly prevalent disorder that can pose a huge clinical burden, especially in elderly patients (11–13, 28). Physical and functional limitations are particularly prevalent in the older population (18), and the ability to self-care is also important in both the surveillance and treatment of onychomycosis (15). While metabolic comorbidities prevalent in elderly patients, such as diabetes, have been frequently studied in association with onychomycosis (15, 29), knee OA, which is significantly debilitating and vastly prevalent in the elderly population (30, 31), has rarely been studied in association with onychomycosis.
In the current study, 59.2% of the patients with knee OA were diagnosed with onychomycosis. Even with the differences in study design and diagnostic methods, this is not only much higher than 4.3% found in the general population (3), and 3.49% in the Korean population (32), but also higher than the number reported by Elewski & Charif (13), in the 61–100 years age group (28.1%) and 29.9% reported from a cross-sectional study of Finnish adults aged 70–93 years (33). Use of REBA, which has a higher sensitivity and specificity than conventional methods, may have also contributed to the higher prevalence found in the current study, but the number was also still greater than 40% based on the KOH test. In summary, although age is a significant risk factor for onychomycosis, and the mean age of the current study group was high, at 70.6 years, the prevalence of onychomycosis was still considerably high; at 54.3% (25 out of 46 patients) in patients under the age of 60 years. This may indicate that, while age is important, the functional limitation caused by knee OA itself is also influential. Severe knee OA is likely to cause the acceleration of a vicious cycle as patients age, of losing the ability to perform surveillance and hygiene care with regards to onychomycosis.
The number of male patients in the current study was relatively low (84 patients; 16.2%), as knee OA is much more prevalent in females (34). However, male sex was again confirmed as a significant risk factor for onychomycosis, as in many previous studies. It is unclear why men are more prone than women to onychomycosis. Environmental factors, including the type of footwear, occupation, and the type and frequency of sports they participate in, are possible factors in this sex difference (35). Notably, the subgroup multivariate logistic analysis based on sex, showed only age as a significant risk factor in the male group (data not shown). Meanwhile, it should also be recognized that 57.3% (250/436) of the female patients with knee OA were found to be positive for onychomycosis, which is significantly greater than the prevalence in the general population. This finding suggests that OA itself acts as a meaningful risk factor for onychomycosis regardless of sex. Also, in the female group, rather than age, the duration of the disease was a significant risk factor, along with hypertension, and being barefooted. Considering that females are more severely affected by knee OA (34), the duration of the disease being more important than age again suggests that knee OA itself has a strong influence on onychomycosis in addition to ageing. Being barefooted is a new risk factor found in our study. Some studies suggest that wearing shoes with socks may provide an ideal environment for onychomycosis, as the feet get moist and warm (28). However, the tendency to wear shoes or sandals without socks could expose the feet and toes to more trauma and lower levels of cleanliness, which is a possible explanation for the current results. Overall, other environmental factors, skin comorbidities, and orthopaedic comorbidities were irrelevant to onychomycosis in the current study.
When multiple knee severity indices were evaluated in association with onychomycosis severity based on SCIO score, K-L grade was the only association found. The patients with K-L grade III or IV had a higher SCIO score (16.3 ± 8.1 vs 12.3 ± 8.1, p = 0.016) compared with the patients with K-L grade I or II. However, precaution is needed in interpreting this result, as age and BMI were also associated with K-L grade. The reason for the limited association found between knee OA and onychomycosis severities may be that the majority of patients visiting the surgery clinic had advanced knee OA (K-L grade III or IV; moderate to severe). We speculate that a comparison between similar proportions of the mild disease group and severe disease group might reveal a more definite association between the 2 disease severities.
While the KOH test is the most frequently used modality in diagnosing onychomycosis, it yields a low sensitivity and high false-negative rate (36). PCR-based REBA is a molecular biologic method that can be used for diagnosing bacterial or fungal species (37–40). Studies showed that REBA yields fast and reliable results with higher specificity and sensitivity compared with fungal culture or KOH test (38, 40). The sensitivity and NPV of the KOH test relative to REBA were only moderate, at 66.2% and 65.7%, respectively. As the newer diagnostic technologies with higher accuracy become both cheaper and faster, the conventional use of the KOH test may need to be reconsidered.
The current study has some limitations. First, there were a limited number of mild cases and the study lacked a proper control group. Secondly, common method bias is possible with a questionnaire-based collection of clinical information. Third, REBA was not performed in all 10 toenails, which would have prevented potential false-negative cases. Despite these limitations, this is the first comprehensive study of onychomycosis in patients with knee OA, which is highly prevalent and debilitating in elderly patients. A large-scale prospective cohort study with a control group is warranted to elucidate the detailed association between knee OA and onychomycosis.
This study reveals that onychomycosis is highly prevalent in patients with symptomatic knee OA. Considering that onychomycosis, which often leads to severe complications, can easily be neglected by both patients and physicians, patient education regarding foot hygiene, more attention to toenail status by the physician, and a multidisciplinary approach, are needed for patients with orthopaedic knee diseases, whose physical function and self-care are compromised. As global life expectancy increases and degenerative diseases, including knee OA, become more prevalent, the close association of onychomycosis, both in prevalence and severity, with OA, should be borne in mind when caring for these patients, since early diagnosis and treatment leads to lower patient morbidity and medical costs.
This study was partially funded by a clinical research grant-in-aid from the Seoul Metropolitan Government-Seoul National University (SMG-SNU) Boramae Medical Center (03-2018-10).
IRB approval status. Approved (Boramae Medical Center IRB number 20-2018-29).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize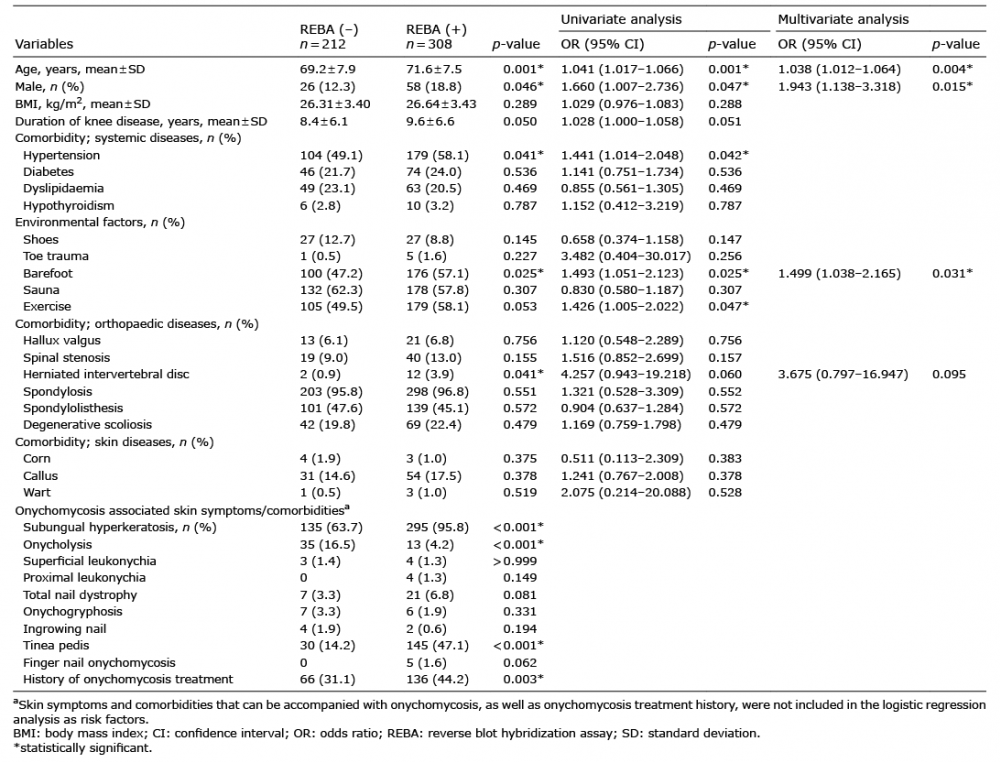 Click to show fullsize
Click to show fullsize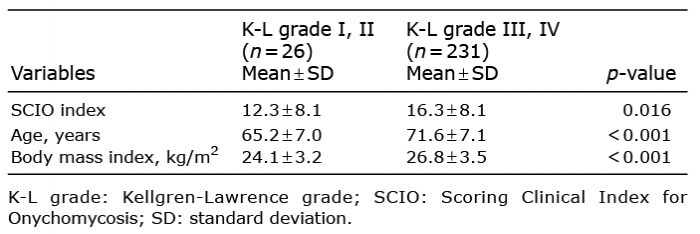 Click to show fullsize
Click to show fullsize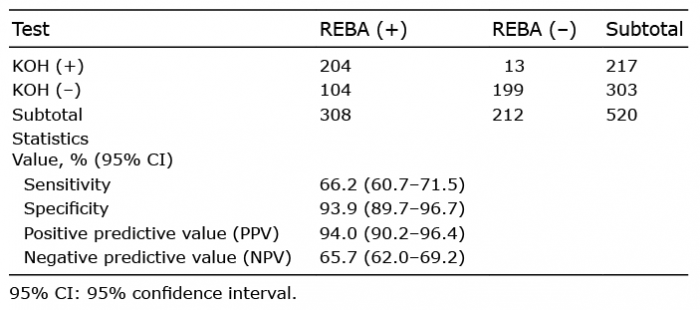 Click to show fullsize
Click to show fullsize