


1Dermatology Department, University Hospital Miguel Servet, 2Aragon Psychodermatology Research Group (GAI+PD), Zaragoza, 3Spanish Research Group of Dermatology and Psychiatry (GEDEPSI) of the Spanish Academy of Dermatology and Venereology (AEDV), Madrid, 4University of San Jorge, Zaragoza, Pharmacoeconomics & Outcomes Research Iberia, 5Department of Psychology, University of Zaragoza, 6Psychiatry Department, University Hospital “Lozano Blesa”, Zaragoza, 7Dermatology Department, Santa Creu i Sant Pau Hospital, Universitat Autonoma de Barcelona, Barcelona, 8Dermatology Department, University Hospital Infanta Sofía, San Sebastián de los Reyes, Madrid, 9Dermatology Department, Royo Villanova Hospital, Zaragoza, 10Dermatology Department, Barbastro Hospital, Barbastro and 11Dermatology Department, University Hospital Dr Negrín, Las Palmas de Gran Canaria, Spain
To date, there are no disease-specific instruments in Spanish to assess quality of life of patients with hidradenitis suppurativa. A multicentre study was previously carried out in Spain between 2016 and 2017 to develop the Hidradenitis Suppurativa Quality of Life-24 (HSQoL-24), a disease-specific questionnaire to assess quality of life in patients with hidradenitis suppurativa. The objectives of this study are to revalidate the HSQoL-24 in Spanish with a larger sample of patients, and to present the English version. In this multicentre study in Spain, patients with hidradenitis suppurativa completed the HSQoL-24, the Dermatology Life Quality Index and the Skindex-29. The Hurley staging system was used to assess the severity of the disease. Validation of the questionnaire was carried out in 130 patients, of whom 75 (57.7%) were women. This study demonstrates adequate values of reliability and validity of the HSQoL-24, confirming the previous test re-test validation and making this questionnaire one of wide clinical validity in terms of results perceived by patients.
Key words: hidradenitis suppurativa; quality of life; patient-reported outcome measure; psychometrics; validation.
Accepted Aug 18, 2021; Epub ahead of print Aug 24, 2021
Acta Derm Venereol 2021; 101: adv00529.
doi: 10.2340/00015555-3905
Corr: Lucia Tomas-Aragones, Department of Psychology and Sociology, University of Zaragoza, Calle Pedro Cerbuna, 12, ES-50009 Zaragoza, Spain. E-mail: luciatomas@cop.es
Hidradenitis suppurativa is a chronic inflammatory skin disease with negative physical and psychosocial effects. The importance of measuring quality of life in patients with hidradenitis suppurativa has been described in numerous studies, as this skin disease has a negative impact on people’s lives. Thus, it is important to develop and use disease-specific questionnaires to better understand the impact of this disease on patients. The Hidradenitis Suppurativa Quality of Life-24 is a disease-specific instrument for measuring quality of life in adult patients with hidradenitis suppurativa. The instrument was developed and validated in Spain.
Hidradenitis suppurativa (HS) is a chronic inflammatory skin disease with negative physical and psychosocial effects (1). The prevalence of HS is unclear, ranging from 0.00033% to 4.10%; HS occurs more frequently in young adults and in women, as well as in African-Americans and bi-racial individuals (2).
HS has a large impact on quality of life (3): advancement of the disease is the factor that has the most impact on patients’ well-being (4). Patients with HS are at a greater risk of suicide than the general population (5). The use of patient-reported outcomes and measurement of health-related quality of life (HRQoL) are probably more important in HS than in many other skin conditions, due to the considerable psychological burden of HS on patients (6).
Recent advances in non-invasive procedures for early diagnosis (6) and novel approaches to treatment of HS may contribute to improvement in patients’ quality of life (8). As HS has very specific properties, there is a need for an instrument to measure the specific impact on HRQoL in patients with HS. However, no such instrument has been published in Spanish. The development, validation and use of HS-specific instruments has been encouraged (9). HRQoL in HS is measured using various instruments, for example Skindex-29 and the Dermatology Life Quality Index (DLQI) (6). In the last 5 years other instruments have been developed: a 23-item HS-specific QoL questionnaire: HiSQoL (10), a 44-item HS-QoL instrument (11), and a 17-item HiSQoL score (12), which has been developed and validated for use in clinical trials. The development of another HS-QoL instrument is also described, but is pending validation (13). These measures have been attempts to standardize measurement of QoL in HS by using disease-specific measures, but there are now several to choose from: they are commented on below and compared with the Hidradenitis Suppurativa Quality of Life-24 (HSQoL-24).
The HSQoL-24 (14) is a disease-specific instrument for measuring quality of life in adult patients with HS. It is a Spanish self-administered questionnaire that evaluates 6 domains: psychosocial, economic, occupational, relationships, personal, and clinical. The development and initial validation of the instrument, involving 30 patients, was published previously (14). It was shown to have good psychometric properties: internal consistency, reproducibility, construct and content validity, feasibility and sensitivity to change. However, the sample of 30 patients in the original study was small, and the confidence in these results is therefore rather low. There is a strong need to repeat this work with a larger sample.
The aims of the current study are to revalidate the psychometric properties of the Spanish HSQoL-24 with a with a larger sample of patients, and to perform a cross-cultural adaptation of the instrument into the English language.
In this multicentre study, consecutive patients with a diagnosis of HS were informed about the study. Patients who were willing to participate were asked to provide written informed consent. Inclusion criteria required patients to be over 18 years of age with a diagnosis of HS confirmed by a dermatologist, and to be capable of completing the questionnaires in Spanish. Patients completed the HSQoL-24, the DLQI (15) and the Skindex-29 (16). The Hurley staging system was used to assess the severity of the disease.
The study (PI16/020) was approved by the Clinical Research Ethics Committee of Aragon (CEICA) on 10 February 2016 and by the corresponding committees in the other participating hospitals. Patients were recruited at the following hospitals: University Hospital Miguel Servet (Zaragoza), Royo Villanova Hospital (Zaragoza), Barbastro Hospital (Huesca), Infanta Sofia Hospital (Madrid), Santa Creu i Sant Pau Hospital (Barcelona), and Doctor Negri?n Hospital (Las Palmas de Gran Canaria).
To perform transcultural adaptation of HSQoL-24 to English, the published norms in the literature were followed (17, 18). The method involved translation and back-translation in the following stages: translation of the original Spanish questionnaire into English by a bilingual translator (native language, English) and back-translation of the English version into Spanish by another bilingual translator (native language, peninsular Spanish) for review by the authors of the original Spanish questionnaire.
During the cross-cultural adaptation process, it was found necessary to reorder the HSQoL-24 items consecutively according to 6 domains: psychosocial, economic, occupational, relationships, personal, and clinical. Clearer instructions for its use, completion and interpretation were also written in order to facilitate the use of HSQoL-24 in Spanish and English.
The HSQoL-24 questionnaire has 24 items, each with 5 possible answers (see Appendix S1). It is user-friendly and takes approximately 10 min to complete. The document providing information and instructions for use is shown in Appendix S2.
Validation of the questionnaire was carried out in a sample of 130 patients; 55 (42.3%) men and 75 (57.7%) women. The mean age ± standard deviation (SD) was 37.3 ± 11.8 years, with 42 patients (32.3%) under 30 years, 55 (42.3%) between 31 and 45 years and 33 (25.4%) over 45 years. A total of 33 patients (25.4%) were at Hurley system Stage I severity, 62 patients (47.7%) stage II, and 35 (26.9%) stage III. Thirty-eight patients (29.2%) had had the condition for ≤ 5 years, 17 (13.1%) between 5 and 10 years, and 75 (57.7%) for at least 10 years: overall, patients had had the condition for a mean of 14.1 ± 11.0 years.
Reliability
The internal consistency (Cronbach’s α) was 0.866. The Cronbach’s α value was also measured assuming the elimination of various questions to analyse their relevance, obtaining a minimum value of 0.854 when questions 8 (children) or 13 (cost) were eliminated, and a maximum value of 0.878 when question 18 (planned activities) was eliminated. The Cronbach α value is considered adequate and indicates a good internal consistency that is maintained even when some of the items are eliminated.
Validity analysis
Correlation and regression analysis. Construct validity was assessed using a correlation and regression analysis with DLQI and Skindex-29. Correlation with DLQI 0.690 (p < 0.001) and Skindex-29 0.869 (p < 0.001). High values of the correlation coefficients and an adequate equivalence to the validated questionnaires indicate an adequate validity.
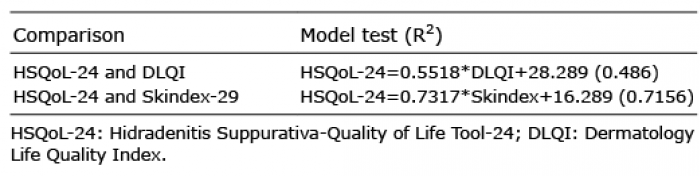
The results of the regression between the questionnaires, considering the HSQoL-24 score as the dependent variable, are shown in Table I and Fig. 1.
Table I. Regression models
Fig. 1. Graphical representation of the regression models.
The analysis suggests that DLQI makes it possible to predict 48.6% of the value of variance in HSQoL-24; Skindex-29 shows a greater fit for the model, accounting for 71.5% of the variance in HSQoL-24.
Cut-off points. The cut-off points were calculated by comparing the categories of the Skindex-29 with those of the HSQoL-29, because Skindex-29 yielded the highest correlation and regression values. Table II shows the results of the descriptive study of the HSQoL-24 value in the different categories of Skindex-29.
Table II. Values of Hidradenitis Suppurativa-Quality of Life Tool-24 (HSQoL-24) in Skindex-29 categories
Receiver operating characteristic (ROC) curve analysis showed that values of between 0 and 32 in HSQoL-24 correspond to patients in whom HRQoL is not affected, with a sensitivity of 0.878 and a specificity of 0.636. The area under the curve (AUC) was 0.897 (95% confidence interval (95% CI) 0.839–0.954). The separation between the categories mild and moderate was suggested at a cut-off point of 37, with a sensitivity of 0.645 and specificity 0.714 and AUC 0.712 (95% CI 0.602–0.822). For patients whose HRQoL was severely affected, the cut-off point of the proposed curve was 43, with a sensitivity of 0.881 and a specificity of 0.800. The AUC was 0.942 (95% CI 0.900–0.984) (Fig. 2).
Fig. 2. Receiver operating characteristic (ROC) curves.
The cut-off scores to interpret the effect on patients’ quality of life are shown in Table III.
Table III. Cut-off points and effect on patient’s quality of life in Hidradenitis Suppurativa-Quality of Life Tool-24 (HSQoL-24)
In recent years, the development of new drugs for the treatment of HS has promoted efforts to develop disease-specific questionnaires to measure quality of life of patients with HS. Generic QoL instruments can underestimate the severity of the impact of the disease on patients’ lives (8).
This paper analyses the characteristics of the HSQoL-24 questionnaire as a predictor of HRQoL in patients with HS. It is a 24-item HS-specific QoL instrument with a 4-week recall period. The questionnaire has already passed a preliminary validation of test re-test reliability in 30 patients with a 30 ± 10 days interval between assessments. The revalidation of other validation aspects presented here was performed with 130 patients, but test-retest was not validated and this point could be a limitation of the study. However, the strong results achieved in the preliminary phase concerning the validity of all domains should be taken into consideration (14). This validation of the main topics of the questionnaire was considered necessary before using the questionnaire more widely (19).
The importance of measuring quality of life in patients with HS has been described in numerous studies (20–22), as this skin disease has a negative impact on people’s lives due to its chronicity, recurrence, impact on body image and sexual health, pain, and odour, among other impacts (20).
The psychometric properties analysed in this study are reliability, validity and prognostic capacity. Reliability was measured as internal consistency with the Cronbach a statistic. The HSQoL-24 results give a value of 0.866, which indicates excellent internal consistency, which is maintained even when one of the items is eliminated. Similar values were located by McLellan et al. (11), who presented α values of 0.955 in physical function and 0.900 in the domain of symptoms and 0.88 in physical function in the Hidradenitis Suppurativa Quality of Life score, which are similar to our values. In the preliminary validation of the HSQoL-24, the values of Cronbach α statistic were similar; 0.92 in test and 0.92 in retest (14).
The construct validity was verified by correlation and regression analysis with the DLQI and Skindex-29. The high values of the correlation coefficients and the appropriate fit of regression models indicated adequate validity, presenting a higher correlation (r = 0.869 vs r = 0.690) and better regression adjustment (R2 = 0.7156 vs R2 = 0.486) with the Skindex-29 vs DLQI. Similar results were found in the preliminary validation with correlation values close to 0.9 with Skindex-29 and 0.7 with the DLQI (14). These values of correlation or determination coefficients are higher than those of other questionnaires used in dermatology in Spain, such as the PSO-LIFE questionnaire in psoriasis, which presented correlation values between 0.4 and 0.8 (23), and similar to the values found in other studies (r = 0.90) (12) although the HSQoL-24 has a better fit with the Skindex. These results indicate that the HSQoL-24 can be considered to have adequate construct validity.
The values of the HSQoL-24 cut-off points presented an adequate sensitivity and specificity for the detection of the categories of patients, with no impact on their HRQoL (0.878 and 0.636, respectively), patients with severe impact (0.881 and 0.800) and mild and moderate impact (0.645 and 0.714). These values were similar to those reported by other authors in other questionnaires used in HS or in dermatology (24, 25).
In conclusion, analysis of the psychometric properties of HSQoL-24 in this further validation study demonstrated adequate values of reliability and validity, adding to the previous test-retest validation and consolidating this questionnaire as a valid tool for wide clinical use.
The authors would like to thank the patients who made this study possible.
Disclosure statement. SEM is copyright owner of HSQoL-24. EVR reports grants, personal fees, non-financial support and other from Abbvie, Almirall, Amgen, Boehringer, Celgene, Janssen-Cilag, Leo Pharma, Lilly, MSD-Schering-Plough, Novartis, Pfizer and UCB, outside the submitted work. TGC reports personal fees from Lilly and Novartis, outside the submitted work. LP reports grants and personal fees from AbbVie, Almirall, Amgen, Boehringer Ingelheim, Celgene, Janssen, Leo-Pharma, Lilly, Novartis, Pfizer, Regeneron, Roche, Sanofi, and UCB, personal fees from Baxalta, Biogen, Fresenius-Kabi, JS Biocad, Mylan, Sandoz, Samsung-Bioepis, and Bristol Myers Squibb, outside the submitted work. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize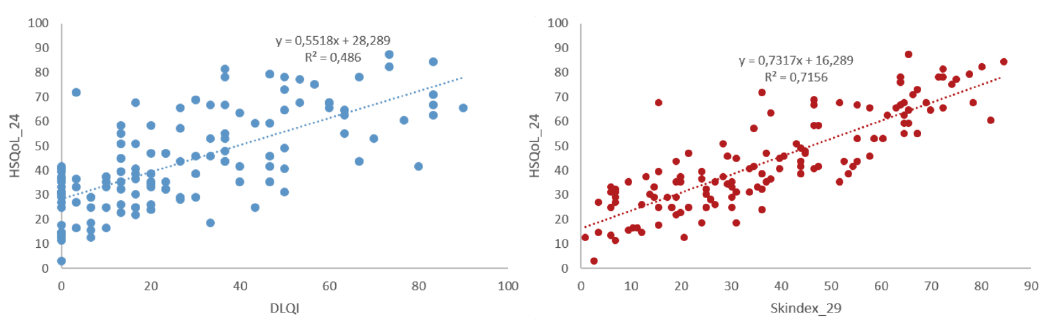 Click to show fullsize
Click to show fullsize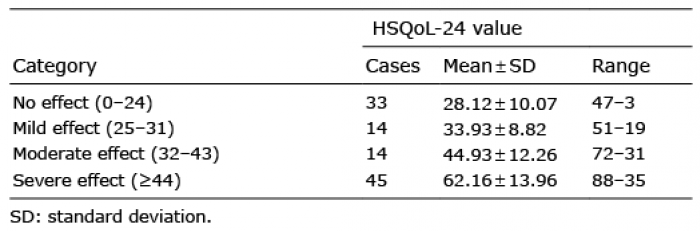 Click to show fullsize
Click to show fullsize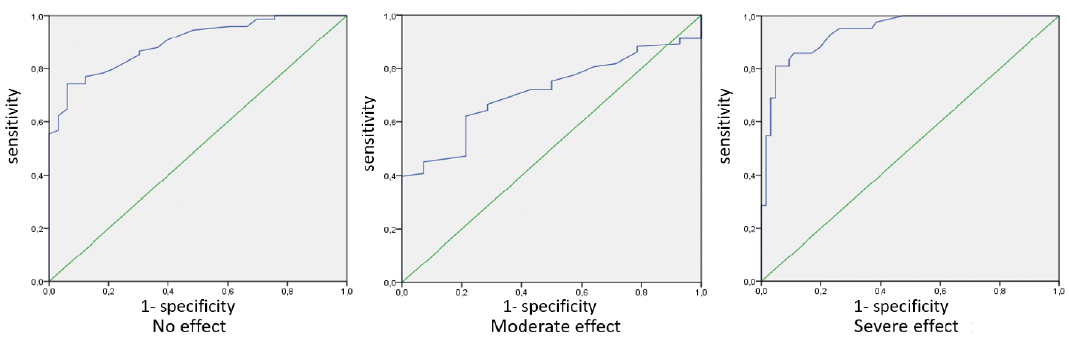 Click to show fullsize
Click to show fullsize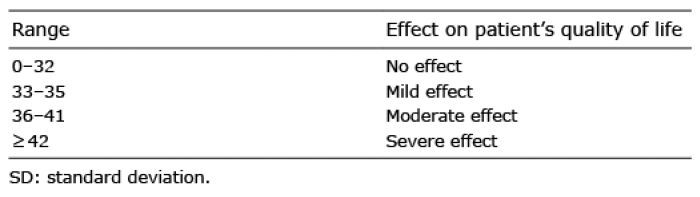 Click to show fullsize
Click to show fullsize