


1Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, 2Department of Food Hygiene and Consumer Health Protection, Faculty of Veterinary Medicine, Wroclaw University of Environmental and Life Sciences, 3Laboratory for Applied Research on Cardiovascular System, Department of Heart Diseases, Wroclaw Medical University and 4Cardiology Department, Centre for Heart Diseases, University Clinical Hospital, Wroclaw, Poland
Current understanding of the underlying pathophysiology of hidradenitis suppurativa (HS) links the disease with proinflammatory activation and autoimmune processes. This study investigated serum levels of interleukin (IL)-22, a cytokine critically involved in epithelial homeostasis, in the context of the broad clinical spectrum of patients with HS. The study also assessed the relationship between serum IL-22 and pro-inflammatory activation (as evidenced by serum level of IL-6) and serum hepcidin (central regulator of systemic iron homeostasis). Serum concentrations of IL-22 were assessed in 74 patients with HS and 15 healthy subjects. Compared with healthy controls, patients with HS demonstrated decreased levels of serum IL-22 (median; interquartile range (IQR): 12.4 pg/ml (9.8; 23.5) vs 34.8 pg/ml (24.8; 39.8), p < 0.001 vs controls). Disease severity (assessed both with Hurley staging and Hidradenitis Suppurativa Severity Index) did not differentiate IL-22 levels (p > 0.1 in both comparisons). Serum levels of IL-22 and IL-6 did not correlate with each other (R=–0.17, p = ns). In a subgroup of 24 patients with HS with pro-inflammatory activation, the mean level of IL-22 was similar to that of the remaining patients (median (IQR): 9.8 pg/ml (8.5; 15.0) vs 12.0 pg/ml (9.4; 16.3), p = ns). Patients with HS demonstrated a decreased level of hepcidin (mean: 31.3 ± 25.9 pg/ml), which correlated with the levels of IL-22 (R=0.36, p < 0.05). Patients with HS demonstrated significantly decreased levels of serum IL-22, which was neither correlated with pro-inflammatory status nor associated with disease severity, but correlated modestly with serum hepcidin.
Key words: hidradenitis suppurativa; cytokines; interleukin-22; hepcidin.
Accepted Sep 8, 2021; Epub ahead of print Sep 13, 2021
Acta Derm Venereol 2021; 101: adv00558.
doi: 10.2340/00015555-3928
Corr: Jacek C. Szepietowski, Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, ul. Chalubinskiego 1, PL-50-368 Wroc?aw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Although interleukin-22 plays an important role in various inflammatory skin disorders, there are very limited data regarding its status in hidradenitis suppurativa, which is a rare, chronic and highly debilitating disease. The aim of this study was to assess serum levels of interleukin-22 in patients with hidradenitis suppurativa and to connect it with proinflammatory activation, potential derangements in iron status, and the clinical severity of the disease. The results showed that circulating levels of interleukin-22 were significantly lower in patients with hidradenitis suppurativa in comparison with healthy controls, and that these levels correlated with decreased levels of hepcidin, which is the central regulator of iron storage. Surprisingly, there was no connection between interleukin-22 levels and either proinflammatory activation or severity of hidradenitis suppurativa.
Hidradenitis suppurativa (HS) is a chronic skin disease with a recurrent nature and debilitating course, with a prevalence of 0.05–4.1% of the population (1, 2). HS significantly impairs patients’ quality of life and remains a challenge in terms of treatment and management (3). The pathophysiology of HS is multifactorial and not fully understood. Recent data strongly indicate the generalized character of the disorder, with a pivotal role of immunological abnormalities and proinflammatory activation (4, 5). Subclinical inflammation presents within the skin of patients with HS before the appearance of clinical lesions leads to aberrant secretion of cytokines and abnormal production of antimicrobial proteins (AMP) (6). AMPs are produced continuously by the keratinocytes as part of innate immunity in response to microbial infection and inflammation. In addition to antimicrobial properties, AMPs exhibit multiple immunomodulatory functions; namely stimulation of production of cytokines (6, 7).
Interleukin (IL)-22, a member of the IL-10 family, is released by various types of lymphoid and non-lymphoid cells, and its production is regulated by an interplay of cytokines and transcription factors (8). IL-22 interacts directly with IL-22 receptors expressed in tissue cells (broadly distributed in the skin, digestive and respiratory system), preserving the integrity of homeostasis in the boundary organs and tissues against intestinal pathogens and commensal bacteria (9). In the epithelial cells IL-22 stimulates AMPs, therefore preventing bacterial infections and interacting with inflammatory processes (10). The role of upregulated IL-22 production has been reported in psoriasis (11). Little is known about downstream IL-22 signalling in HS. It appears that HS is characterized by relative deficiency of IL-22 expression in the lesional skin compared with other chronic inflammatory skin diseases, such as psoriasis or atopic dermatitis (12).
The aims of this study were to evaluate the serum level of IL-22 in a broad clinical spectrum of patients with HS, and to assess the relationship between serum IL-22 and serum hepcidin, which is central regular of systemic iron homeostasis. Our previous study found dysregulated iron homeostasis in HS (13), and IL-22 is known to regulate iron availability through induction of hepcidin (14).
Study cohort
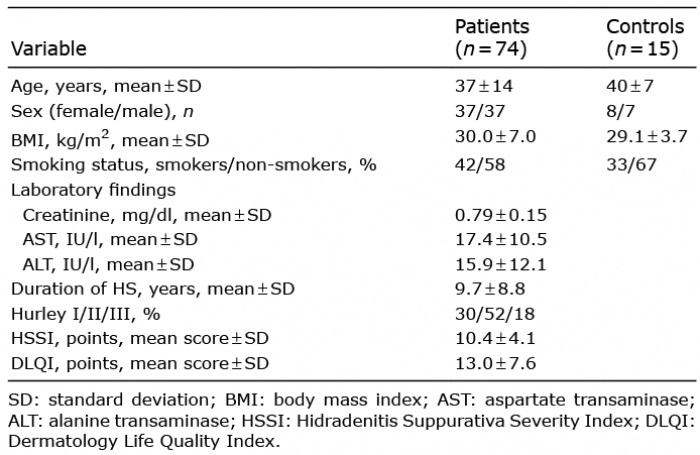
The study was conducted following approval from the local ethics committee (number KB - 336/2017 issued by Wroclaw Medical University Ethics Commitee). Seventy-four patients (37 women and 37 men, mean ± standard deviation (SD) age: 37 ± 14 years) with diagnosed HS (according to well-established clinical criteria) (15) were included in this study. The mean duration of the disease was 9.7 ± 8.8 years. Subjects with any acute or chronic illness that might have influenced pro-inflammatory activation (including infection, known malignancy, chronic kidney disease, chronic cardiovascular diseases and haematological diseases) were excluded. Since the study evaluated iron status-related biomarkers, those patients who received treatment for anaemia or iron deficiency in the previous 12 months were also excluded. None of the patients received any biologic treatment before entering the study and they all were biologic naïve. None of the patients took any immunomodulatory medications (including antibiotics) for at least 6 months prior to inclusion. The clinical evaluation of HS severity was made according to the Hidradenitis Suppurativa Severity Index (HSSI) and 3-degree scale proposed by Hurley (16, 17). With regard to HSSI, patients were classified as having mild (0–7 points), moderate (8–12 points) or severe (≥ 13 points) disease (18). To further characterize the HS patient population Dermatology Life Quality Index (DLQI) assessment was performed (18). The clinical characteristics of the patients are shown in Table I.
Table I. Baseline characteristics of the patients with hidradenitis suppurativa (HS) and controls
The control group comprised 15 subjects (8 women and 7 men, mean ± SD age: 40 ± 7 years) with no acute disease (occurring in the previous 6 months) or chronic disease and related therapy. Healthy controls were recruited from the hospital staff and patients’ relatives
Laboratory assessments
In both groups (HS patients and healthy controls) venous blood samples were taken in the morning after an overnight fast, following at least 15 min of supine rest. After centrifuging, the plasma and serum were collected and frozen at –70°C until further analysis.
Serum level of IL-22 was measured using a commercially available enzyme-linked immunoassay (ELISA) (R&D Systems, Minneapolis, MN, USA). Serum level of IL-6 (pg/ml), as a marker of proinflammatory activation, was measured using a commercially available ELISA (R&D Systems) (19). The upper limit of normal in our laboratory for IL-6 was 1.48 pg/ml. We prospectively defined HS patients with IL-6 above 1.48 pg/ml as having proinflammatory activation (20).
Serum hepcidin (ng/ml) was measured using a commercially available ELISA (BACHEM, Bubendorf, Switzerland). This ELISA method was validated against a gold standard for hepcidin assessment, namely liquid chromatography mass spectrometry developed at King’s College London, confirming a strong correlation between the measurements performed using the liquid chromatography mass spectrometry and the BACHEM assay in patients with chronic kidney diseases and healthy subjects (21). Increased levels of hepcidin may occur in the circulation due to the state of inflammation (22).
Basic laboratory biomarkers indicating liver and kidney function were measured: creatinine (mg/dl), aspartate transaminase (AST), and alanine transaminase (ALT) (IU/l).
Statistical analysis
The normality of the distributions of continuous variables was tested using the Kolmogorov–Smirnov test. Continuous variables with a normal distribution were expressed as means ± SD. The remaining continuous variables with a skewed distribution were expressed as medians with upper and lower quartiles (interquartile range; IQR). Categorical variables were expressed as numbers with percentages. The statistical significance of differences between the groups was tested using Student’s t-test, Mann–Whitney U test, or the χ2 test, where appropriate. The associations between variables were assessed using Spearman’s rank correlation coefficients. All statistical analyses were performed with Statistica 10 (Statsoft, Tulsa, OK, USA). A value of p < 0.05 was considered statistically significant.
The clinical severity of the disease was assessed with Hurley staging with the following distribution: 22 patients (30%) were classified as stage I, 39 (52%) as stage II and 13 (18%) as stage III, respectively. HS severity assessed with HSSI was 10.4 ± 4.1 points (range 4–18 points). Patients’ quality of life, evaluated with Dermatology Life Quality Index (DLQI), was impaired with mean score of 13.0 ± 7.6 points (range 0–28 points).
Serum interleukin-22 in patients with hidradenitis suppurativa
Compared with healthy controls, patients with HS demonstrated a significantly decreased level of serum IL-22 (median [IQR]: 12.4 pg/ml (9.8; 23.5) vs 34.8 pg/ml [24.8; 39.8], p < 0.001 vs controls) The IL-22 level neither differed across Hurley stages nor across HSSI (p > 0.05) (Table II).
Table II. Interleukin (IL)-22 level and hidradenitis suppurativa severity assessed with Hurley scale and Hidradenitis Suppurativa Severity Index (HSSI)
Relationship between serum interleukin-22 and proinflammatory activation in patients with hidradenitis suppurativa
Patients with HS demonstrated elevated levels of IL-6 (median [IQR]: 0.05 [0.05; 2.6] pg/ml). There was no correlation between serum level of IL-6 and disease severity expressed as HSSI (R = 0.22, p = 0.06).
There was no correlation between levels of IL-22 and IL-6 in the entire study population (R = –0.166, p = 0.16).
A group of 24 patients with HS (32%) with evidence of pro-inflammatory activation (defined as IL-6 level above the upper limit of normal in our laboratory) was identified. Serum levels of IL-22 did not differ between these 2 groups (median [IQR]: 9.8 pg/ml [8.5; 15.0] vs 12.0 [9.4; 16.3], patients with proinflammatory activation vs remaining patients, p > 0.2). Also, in the group of 24 patients with proinflammatory activation, no correlation was found between serum levels of IL-22 and IL-6 (R = 0.144, p > 0.1).
Relationship between serum interleukin-22 and hepcidin in patients with hidradenitis suppurativa
As reported previously, patients with HS demonstrated decreased levels of hepcidin (mean 31.3 ± 25.9 pg/ml), which did not correlate with the severity of the disease expressed by HSSI (R = 0.01, p = 0.98). Hepcidin serum levels in our patients with HS correlated with IL-22 (R = 0.36, p < 0.05; Fig. 1).
Fig. 1. Modest correlation (R = 0.36, p < 0.05) between serum levels of interleukin (IL)-22 and hepcidin, suggesting potential interrelationship between IL-22 signalling and iron status in hidradenitis suppurativa.
This study revealed decreased serum levels of IL-22 in a broad clinical spectrum of patients with HS, which neither correlated with pro-inflammatory activation nor with disease severity. There was a modest correlation between serum levels of IL-22 and hepcidin, suggesting a potential relationship between IL-22 signalling and iron status in HS.
A growing body of evidence indicates that deranged inflammatory mechanisms are involved in the underlying pathophysiology of HS (4). However, it remains unclear which immune pathways and cytokines are involved in pro-inflammatory signalling leading to disease progression. Among cytokines for which a pathogenic role appears to be well-established are IL-1, IL-17, IL-10, and tumour necrosis factor (TNF)-alpha, which have also become therapeutic targets in HS (24–27). In contrast to up-regulated signalling comprising these cytokines, studies investigating cellular responses in skin lesions of patients with HS revealed reduced numbers of IL-22- secreting cells with down-regulation of the IL-22 pathway (28). Interestingly, IL22 does not directly interact with the immune cells, but targets cells in the outer-body barriers (e.g. the skin, digestive and respiratory systems) and stimulates the production of antibacterial proteins and chemokines (29). IL-22 deficiency in the skin lesions in HS may be associated with an altered pattern of production of AMPs with subsequently impaired skin protection against infections (29, 30). To the best of our knowledge this study is the first to investigate serum levels of IL-22 in a broad clinical spectrum of patients with HS. The results suggest that, in HS, not only is local expression of IL-22 in the skin lesions affected (compared with psoriasis and atopic dermatitis (12)), but also the serum level of this cytokine is significantly decreased, which may indicate more a generalized down-regulation of IL-22 signalling pathways in HS. A lack of interrelation was found between serum IL-22 and disease severity, which can be interpreted as indirect evidence of an early derangement of IL-22 signalling during the natural course of the disease. The results of a double-blind, randomized, placebo-controlled trial with IL-1 antagonist anakinra in patients with HS, demonstrated that IL-1 blockade was associated with improved clinical status, with a concomitant increase in IL-22 production by peripheral blood mononuclear cells (31). These findings do not contradict the therapeutic observations. The current study included patients with less severe disease (as evidenced by both Hurley stage and DLQI), and anti-IL-1 strategy may well result in clinical improvement and the up-regulation of IL-22 signalling across the whole disease spectrum. Interestingly, 24 out of total 74 patients with HF (32%) demonstrated generalized pro-inflammatory activation, as evidenced by an elevated level of serum IL-6. In these patients the serum level of IL-22 did not differ from that in the remaining patients, which may indicate that inflammatory-mediated mechanisms are not involved in IL-22 down-regulation, at least as detected in the blood.
The modest, but significant, relationship between serum hepcidin and IL-22, is an intriguing novel finding. It has been well established that production of hepcidin, a key regulator of iron homeostasis in the body, is induced by proinflammatory cytokine IL-6. We have recently reported deranged iron status in HS, which can be characterized as iron deficiency with a concomitant low level of hepcidin (11). Smith et al. (14) described that IL-22 signalling induces hepcidin production independently of IL-6. Hepcidin limits iron uptake and availability by causing iron accumulation in the macrophages. Therefore, the local and generalized down-regulation of IL-22 found in HS, may be the mechanism underlying the low level of hepcidin, and might lead to reduced iron availability with resultant deterioration of processes involved in microbial defence. However, this hypothetical pathway needs further study.
In summary, patients with HS demonstrated significantly decreased levels of serum IL-22, which was neither related to pro-inflammatory status nor associated with disease severity, but modestly correlated with serum hepcidin. Further research into the role of IL-22 in HS is required.
The preliminary results of our research were presented at European Hidradenitis Suppurativa Foundation 2019 8th Conference.
Funding source: Project for Young Scientists (number STM.C260.20.097), Wroclaw Medical University.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize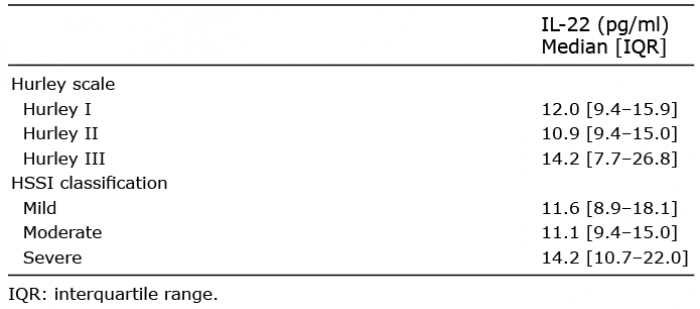 Click to show fullsize
Click to show fullsize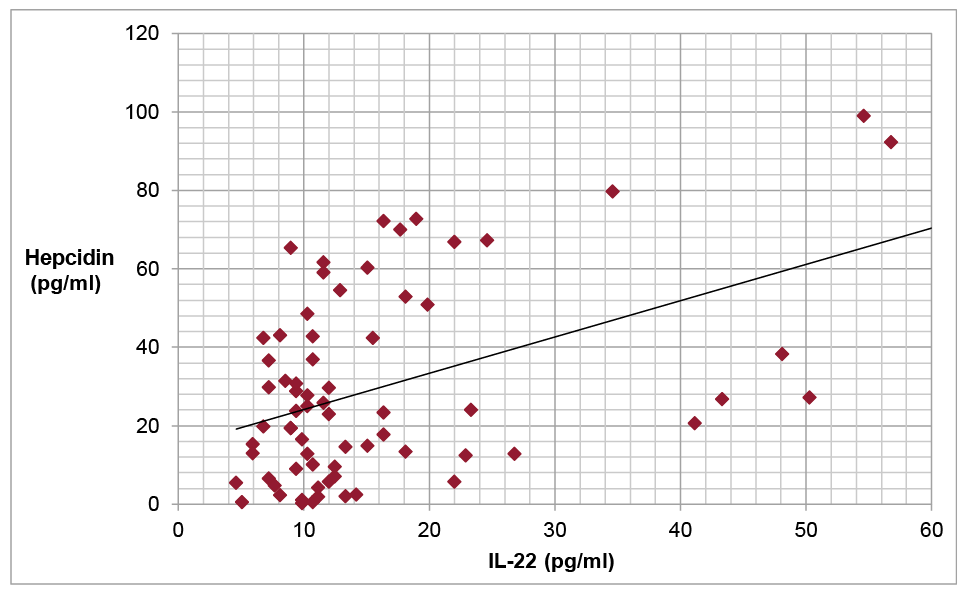 Click to show fullsize
Click to show fullsize