OBJECTIVE: To compare life satisfaction within couples one year after a partner’s stroke and with norm values and social factors.
Subjects and methods: A total of 56 couples were consecutively included. The respondents estimated life satisfaction using the Life Satisfaction Checklist 9-item version. Patients’ impairments, self-care ability and handicap were assessed. Social characteristics were registered. Non-parametrical statistical methods were used for analyses.
RESULTS: Patients were physically mildly disabled by their stroke. The most common symptom was mental fatigability. Patients were, in general, less satisfied than spouses. The couples were less satisfied than norms. Satisfaction with life as a whole, leisure and sex life were most affected for both patients and spouses. Relationship with partner was the only domain in which patients were more satisfied than their spouses and almost equally satisfied compared with norms. The proportion of couples in which both partners agreed they were satisfied, for the following domains was: leisure time 20%, sex life 25%, vocation/occupation 29%, life as a whole 30%, finances 47%, social contacts 48%, relationship with partner 60%, family life 66% and ability in self-care 66%.
CONCLUSION: Life satisfaction was negatively affected in both partners, although in different life domains. Support should address the different needs of patients and spouses as well as their mutual needs.
Key words: cerebrovascular accident/psychology, spouses/psychology, personal satisfaction.
J Rehabil Med 2007; 39: 219–224
Correspondence address: Gunnel E Carlsson, Reg. OT, Institute of Neuroscience and Physiology, Section of Neuroscience and Rehabilitation, SU/Sahlgrenska, SE-413 45 Göteborg, Sweden. E-mail: Gunnel.Carlsson@neuro.gu.se
Submitted May 5, 2006; accepted December 4, 2006
*This article has been fully handled by one of the Associate Editors, who has made the decision for acceptance, as it originates from the institute where the Editor-in-Chief is active.
INTRODUCTION
The complexity of the consequences of stroke and the multitude of factors that affect rehabilitation emphasize the need to measure overall well-being (1) in order to gain a more comprehensive picture of the condition. Life satisfaction is commonly used as an outcome measure of rehabilitation and the adaptation process after disease (2). Satisfaction with life as a whole and with important domains of life has been defined as the connection between the individual’s aspirations, achievement and satisfaction (3). Satisfaction with different domains of life, such as ability in self-care, family and relationship with partner, sex life, leisure and social contacts, daily occupation and finances, has been assumed to be inter-related with satisfaction with life as a whole (4).
Stroke often results in long-term physical, cognitive and emotional dysfunction that may affect all domains of life for patients and their families (5). Motor and cognitive impairment (6), post-stroke fatigue (7) and depression (8) play important roles with respect to patients’ ability to perform activities, their participation and their life satisfaction. Even an apparently mild stroke with no or minimal physical disability can lead to dependence, limited participation and a decrease in life satisfaction (7). Social support has been found to be a strong predictor of post-stroke functional ability in patients (5). Other dimensions of family function, such as communication patterns, coping style, empathy, conflict resolution, care-giving patterns, and problem-solving ability have been found to affect both physical and psychosocial outcome after stroke. Spouses of patients after stroke have been found to have elevated risk of depression, care-giver burn-out, social isolation, loss of freedom, decrease in social life and leisure activities (5), and a decreased life satisfaction (9). Furthermore, the 2 factors most related to psychiatric morbidity in stroke care-givers were the severity of disability, and the presence of emotional and behavioural problems in the stroke survivor (5). Although couples in which one partner has suffered a stroke often experience a dramatic change in their mutual life situation, studies of stroke impact thus far have chiefly been carried out in patients and spouses separately. However, 2 studies were found comparing the partners in a couple with respect to health-related quality of life (HRQoL). One study showed that spouses generally had better HRQoL than their partners with stroke, except concerning emotional and mental health domains (10). The other study showed that spouses’ employment status, amount of support and the functional independence of the patient at hospital discharge were predictors of HRQoL for both partners in the couple (11). Only one study was found that compared partners’ joint life satisfaction after brain injury (12), which showed that function in everyday life, and participation in leisure activities and social life, were related to satisfaction with life in general in both partners. Thus, little is known about how partners in a couple experience satisfaction with life as a whole and in different domains of life after a partner’s stroke. To improve support for patients after stroke and their spouses, there is a need for a better understanding of both partners’ satisfaction with life and of whether life satisfaction is affected in different ways in patients and their spouses. There is also a need for better knowledge about the impact of cognitive and emotional impairments and post-stroke fatigue on couples’ long-term life satisfaction. The study presented here is a part of an extensive study of couples in which one partner has suffered a stroke, for which the results so far have been presented separately for patients and spouses (7, 9). The main aim of the current study was to make within-couple comparisons of life satisfaction and agreement in life satisfaction among patients after stroke and their spouses one year after stroke. A further aim was to compare the patients’ and spouses’ life satisfaction with norm values and in relation to social factors.
METHODS
Study group
The couples were consecutively included at admission to an acute neurological stroke unit between September 1994 and October 1997. The inclusion criteria for patients were: (i) confirmed diagnosis of a first-ever stroke (excluding subarachnoid haemorrhage); (ii) cohabitant with a spouse; (iii) age less than 75 years; (iv) no evidence of co- existing known malignant or other rapidly progressive medical disease; (v) living in Göteborg or surrounding areas; (vi) both partners able to communicate in Swedish. The inclusion process has been described in an earlier paper (13). The patients and their spouses gave informed consent separately, and the Ethics Committee of the Faculty of Medicine, Göteborg University, Sweden approved the study.
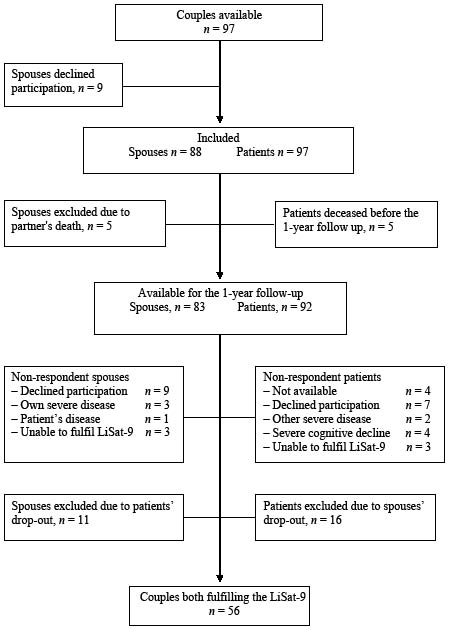
A total of 97 couples fulfilled the inclusion criteria. All patients agreed, but 9 spouses declined to participate in the study. Five patients died before the 1-year follow-up. At the 1-year follow-up the patients were seen by a neurologist (CB) and individual interviews were carried out with the patients (GC) and the spouses (GF-W) concerning their life situation and satisfaction with life. Of the 92 patients and 83 spouses invited to the individual interviews, 56 couples both completed an estimation of their life satisfaction and were included in the matched pairs’ study group. The neurologist met 90 of the 92 patients, one patient dropped out owing to severe post-stroke dementia and the other developed a fatal disease. A flow-chart of the participants and non-respondents is shown in Fig. 1.
Fig. 1. Study inclusion and non-respondents.
There were no significant differences between the non-respondents (n = 36) and the study group (n = 56) with respect to patient characteristics or the demographic characteristics of the couples. There were no significant differences in estimation of life satisfaction between the 16 patients and 11 spouses where only 1 of the partners in the couple completed the Life Satisfaction Checklist 9-item version (LiSat-9) compared with the 56 couples where both partners completed the LiSat 9.
Measurements
The patients were investigated during the first week after stroke according to clinical routines, including a computerized tomography scan. The location of the lesion was registered. Neurological deficit was assessed with the Scandinavian Stroke Scale (SSS) (range from 0, severe neurological impairment, to 48, no neurological impairment) (14), cognitive screening was carried out with the Mini Mental State Exam (MMSE) (range from 0 to 30, with 24 as cut-off level of dementia) (15), and dependence in self-care with the Barthel Index (16) (range from 0, total dependence in self-care, to 100, independent in self-care) (17). Neurological deficit, cognitive screening, and dependence in self-care were re-assessed at the 1-year follow-up. At the 1-year follow-up the following assessments were added: Level of handicap was assessed with the Oxford Handicap Scale (OHS), which is a further development of the Modified Rankin scale and focused on restrictions in lifestyle (range from 0, no handicap/restriction in lifestyle, to 5, severe handicap/restriction in lifestyle) (18); Post-stroke fatigue operationalized as the astheno-emotional syndrome (AE syndrome) (19), which is characterized by mental fatigability, concentration and memory difficulties, sensitivity to bright light and loud sounds, irritability, stress sensitivity and emotional instability, was diagnosed by the neurologist; Depression according to the DSM IV criteria was also diagnosed by the neurologist; The patients and the spouses separately rated their life satisfaction on the LiSat-9 (20); The checklist contains: satisfaction with life as a whole; 1 health item; ability to manage self-care; 2 provision items; vocational, and financial situation; 3 closeness items; sex life, relationship with partner, and family life, and 2 spare time items; leisure, and social contacts. The scale is graded according to 6 levels ranging from 1 (very dissatisfied) to 6 (very satisfied). Age, sex, length of relationship, vocational situation before and after stroke, and responsibility for children were registered for both patients and spouses.
Data analyses
Descriptions of basic data in the study group are presented with median and 25th–75th percentiles as well as with frequencies and proportions. The LiSat-9 was dichotomized into “not satisfied” (categories 1–4) and “satisfied” (categories 5–6). A comparison was made with norm values in a comparable age group living in a steady relationship with a partner (personal communication: K. Fugl-Meyer, 2004) extracted from a Swedish population study (21). Confidence intervals (95% CI) were calculated for the differences in proportion of satisfied patients and spouses, respectively, compared with the norm group, as well as for the difference between paired proportions within the couples. Within-couple differences in life satisfaction were calculated with McNemar’s test. Differences between patients/spouses and norm values were calculated using the χ2 test. The relationship between patients and spouses who were satisfied/not satisfied and the dichotomous variables of sex, working situation, responsibility for children were analysed with the χ2 test or Fisher’s exact test. A p-value of 0.05 was chosen for the level of significance. To investigate whether the non-respondents affected the results, a series of worst case/best case scenario analyses were created. The best-case scenarios, which hypothesized that all non-responding couples agreed in their estimations, did not affect the results. The worst-case scenario that is disagreement between the partners, would in the case of all non-responding patients being satisfied have changed the differences between the partners concerning satisfaction with life as a whole. The worst-case scenario was that all non-responding patients who were dissatisfied would have changed the differences concerning satisfaction with the relationship with partner.
RESULTS
The median age of the patients was 60 years (range 38–74 years) (interquartile range (IQ) 50–67 years) and of the spouses 59 years (range 34–79 years) (IQ range 50–66 years). Thirty-nine (70%) of the 56 patients were men. The median length of the relationships was 32 years (range 2–54 years). Twenty percent of the couples had responsibility for children. The number of patients working full-time was reduced from 26 before stroke to 6 after one year, and another 6 patients working part-time. Twenty-one spouses worked full-time and 13 part-time both before and after their partners’ stroke, although some had changed their working schedule after their partner’s stroke.
The first week after stroke onset 57% of the patients were independent in personal activities of daily living with a maximum score of 100 in the Barthel Index. Despite this, 80% of the patients had a moderate handicap at the 1-year follow up according to the OHS, which means a handicap that significantly restricts lifestyle and prevents a totally independent existence. AE syndrome was the most common problem, diagnosed in 77% of the patients. The characteristics of the stroke patients at stroke onset and at the 1-year follow-up are described in Table I.
| Table I. Patients’ neurological and cognitive characteristics, ability in self-care and level of handicap in the first week after stroke onset and at the 1-year follow up (n = 56). |
| | n (%) | Median (IQ),range First week after stroke onset | Median, (IQ), range 1-year follow-up |
| Cerebral infarction | 47 (84) | | |
| Cerebral haemorrhage | 9 (16) | | |
| Stroke location Left hemi- sphere Right hemis- phere Bilateral Infratentorial lesion | 25 (44) 20 (36) 1 (2) 10 (18) | | |
| Scandinavian Stroke Scale | | 42 (42–46) 7–48 | 48 (48–48) 25–48 |
| Mini Mental tate Exam | | 28 (24–29) 0–30 | 29 (26–30) 14–30 |
| AE syndrome 1-year follow-up | 43 (77) | | |
| Depression 1-year follow-up | 21 (38) | | |
| Barthel Index | | 100 (60–100) 0–100 | 100 (100–100) 60–100 |
| Oxford Handicap Scale | | | 3 (2–3) 0–5 |
| AE: astheno-emotional; IQ: interquartile range, 25–75% percentiles. |
Life satisfaction compared with the norm group
Compared with the norm group, the trend was that the patients and spouses were more often less satisfied. These differences were significant for both partners in the couples as concerns their satisfaction with life as a whole (patients p = 0.001, spouses p = 0.05), leisure (patients p = 0.001, spouses p = 0.01) and sex life (patients p = 0.01, spouses p = 0.025) and for the patients concerning satisfaction with ability in self-care (p = 0.001), family life (p = 0.05) and daily occupation (p = 0.001). The spouses were significantly less satisfied with their relationship with their partner (p = 0.001), while the patients were almost as equally satisfied as norms. The proportions of patients, spouses and persons in the norm group that were satisfied with different life domains and 95% CI for differences in life satisfaction between the patients, spouses, and norms are shown in Table II.
| Table II. Proportion of patients and spouses satisfied according to LiSat-9, comparison with a Swedish norm population, and confidence intervals for the differences between the proportions (n = 56). |
| | Patients satisfied | Spouses satisfied | Norm group satisfied Age 50–74 years† | Differences in proportion satisfied patients and the norm population with 95% CI | Differences in proportion satisfied spouses and the norm population with 95% CI |
| | (%) | (%) | (%) | % (95% CI) | % (95% CI) |
| Life as a whole | 39 | 64 | 77 | 38 (25–51) | 13 (0–26) |
| Health | | | | | |
| Ability in self-care | 71 | 93 | 93 | 22 (10–34) | 0 (–7–7) |
| Closeness | | | | | |
| Relationship with partner | 83 | 67 | 86 | 3 (–7–13) | 19 (6–32) |
| Family | 79 | 82 | 89 | 10 (3–19) | 7 (–3–17) |
| Sex life | 34 | 41 | 58 | 24 (10–38) | 17 (3–31) |
| Spare time | | | | | |
| Leisure | 38 | 52 | 71 | 33 (20–46) | 19 (6–32) |
| Contacts | 64 | 73 | 75 | 11 (–2–24) | 2 (–10–14) |
| Provision | | | | | |
| Vocation /occupation | 45 | 61 | 67 | 22 (8–36) | 6 (–7–19) |
| Finances | 58 | 70 | 65 | 7 (–7–21) | 5 (–8–18) |
| †Fugl-Meyer, K, unpublished data (2004). LiSat-9: Life Satisfaction Checklist 9-item version; 95% CI: 95% confidence interval. |
Within-couple comparisons of life satisfaction
A within-couple comparison of satisfaction with different life domains was carried out. Concerning life as a whole the patients were significantly less satisfied than their spouses (p = 0.007), with a difference in the proportion of satisfied patients and spouses of 25% (95% CI 9–41). The spouses were also significantly more satisfied with their ability in self-care (p = 0.008), with a difference in proportion of satisfied patients and spouses of 21% (95% CI 16–26). By contrast, spouses were significantly less satisfied with their relationship with their partner than were the patients (p = 0.035), with a difference in proportion of satisfied patients and spouses of 17% (95% CI 4–30). Even though there was a trend that the patients were less satisfied with their family life, sex life, leisure, social contacts, vocation/daily occupation and finances than their spouses, there were no significant differences concerning these items within the couples.
The proportion of couples in which both partners were satisfied varied between the life domains. The highest proportion of couples in which both partners were satisfied was found for family life (66%) and relationship with partner (60%). In addition, in 66% of the couples, both partners were satisfied with their own ability in self-care. In 48% both partners were satisfied with their social contacts and in 47% with their finances. However, in only 29% of the couples were both partners satisfied with their vocation/daily occupations, 25% with their sex life and 20% with leisure time. Both partners were satisfied with their life as a whole in 30% of the couples. The levels of agreement within the couples in their estimation of life satisfaction are given in Table III.
| Table III. Agreement within the couples in estimation of life satisfaction according to the LiSat-9 (n = 56). |
| | Agreement satisfied n (%) | Agreement not satisfied n (%) | Patient satisfied/spouse not satisfied n (%) | Patient not satisfied/spouse satisfied n (%) |
| Life as a whole | 17 (30) | 15 (27) | 5 (9) | 19 (34) |
| Health |
| Ability in self-care | 37 (66) | 1 (2) | 3 (5) | 15 (27) |
| Closeness |
| Relationship with partner | 33 (61) | 6 (11) | 12 (22) | 3 (6) |
| Family life | 37 (66) | 3 (5) | 7 (13) | 9 (16) |
| Sex life | 11 (25) | 22 (50) | 4 (9) | 7 (16) |
| Spare time |
| Leisure time | 11 (20) | 17 (30) | 10 (18) | 18 (32) |
| Contacts | 27 (48) | 6 (11) | 9 (16) | 14 (25) |
| Provision | | | | |
| Vocation/occupation | 16 (29) | 13 (23) | 9 (16) | 18 (32) |
| Finances | 25 (47) | 10 (19) | 6 (11) | 12 (23) |
| LiSat-9: Life Satisfaction Checklist 9-item version. |
Life satisfaction and demographic and social variables
There were no significant differences between men and women with respect to any of the domains of life satisfaction. Among the spouses, responsibility for children was related to lower satisfaction with finances (p = 0.027). For patients, responsibility for children was related to lower satisfaction with family life (p = 0.008). Spouses who worked compared with spouses not working were significantly more satisfied with their ability in self-care (p = 0.020) and vocational/occupational situation (p = 0.015). Both patients (p = 0.018) and spouses (p = 0.016) who worked were significantly more satisfied with their social contacts than those who were not working.
DISCUSSION
Although most patients in this study had an apparently mild stroke, it had affected satisfaction for both partners in the couple, but in somewhat different areas of life. Compared with the norm group there was a pattern of less satisfaction among the couples, and within the couples the patients were less satisfied than their spouses in all domains except relationship with partner.
Marital aggrandizement, i.e. an idealized appraisal of one’s spouse and marriage, has been found in persons with failing health (22). It is also probable that the patients’ satisfaction with their relationship with their partner could be based on a feeling of gratitude towards the spouses.
Setting goals together and maintaining purpose and meaning in life (16), and equity in decision-making (23) have been found to be important to marital adjustment and satisfaction. These are abilities that demand more advanced cognitive processing, possibly affected by the different symptoms of the AE syndrome (19), which was the main problem of the patients in this study. Contradictory to the finding that spouses were significantly less satisfied with their relationship with their partner compared with the stroke survivor, this was also one of the items with the highest agreement for both partners being satisfied. This poses an indication of the importance of identifying the couples with problems and in need of support.
The closeness items were those with highest agreement with both partners satisfied. These are areas that are unconditionally shared with the partner, while leisure time and provision items are areas in life in which the partner is not necessarily included. To our knowledge no norm values are available concerning the extent to which both partners in a couple agree with each other in their perception of life satisfaction. However, there is a growing knowledge concerning the importance of focusing on the relationship and the dyadic coping within couples in which one partner has a chronic illness (24).
Satisfaction with life as a whole was negatively affected for both partners in the couple, but mostly for the patients. In 27% of the couples both were dissatisfied. This is in agreement with the study by Eriksson et al. (12), who found this to be the case in 29% of couples. There are no indications that the participants in our study were less satisfied with life as a whole prior to stroke compared with norms (9).
Both patients and spouses were significantly less satisfied with leisure activities compared with the norm group, and in only 20% of the couples they agreed in being satisfied with this area of life. Leisure activities are known to be affected by stroke (25). Engagement in leisure activities is an important predictor of satisfaction with life as a whole in patients after stroke (12), as well as in the general population (26), showing that this is an important area for rehabilitation services.
Only 25% of the couples agreed in being satisfied with their sex life and as many as 50% agreed in being not satisfied. In a study focused on moderately-severely disabled stroke patients and their spouses, more than 50% reported a marked decline in their sexual function and satisfaction with sex life (27). Our study suggests the need to give this problem attention even among couples where the partner has suffered a mild stroke.
Responsibility for children was related to the patients being less satisfied with family life. This finding was supported in the qualitative study conducted on a sub-group of 15 patients from this study group, where the respondents told that they were unable to respond to the expectations and needs of their children after the stroke (28). No other study was found, addressing the parenting ability from the perspective of the stroke survivor. Studies have shown that changes in the parents’ ability to be supportive have an impact on children’s emotional health and functioning (29). Perception of a stressful life situation was found to affect children’s adjustment more than the objective severity of illness of the parent (30). Visser-Meily et al. (31) found that only 50% of children of patients after stroke received any support during the rehabilitation period, and the support given was related largely to the severity of the disablement in the parent. The present study indicates the importance of taking into account the parenting role of the stroke survivor and the need of providing support to children even when the parent has suffered an apparently mild stroke.
Our aim was to make within-couple comparisons of life satisfaction, as an outcome measure of the adaptation process of the couples. We did not address the issues of coping strategies, social support and family function, all of which are known to be important factors for life satisfaction. This could be raised as a limitation of this study, and of course are important issues for future studies from a within-couple perspective. Another limitation of this study is the ceiling effects of the SSS, the Barthel Index and the MMSE, all instruments frequently used in stroke studies. To be able to capture difficulties in more advanced motor control, cognitive processing, and activities, more sensitive instruments must be used. By using self-reporting data and assessment of restrictions in lifestyle, however, this study shows that these patients have remaining limitations after one year, which affects life satisfaction for themselves and their spouses. To rate life satisfaction, the LiSat-9 was used in this study. The grouping of the domains (26) as well as the reference values (21) are based on a later developed 11-item version that also includes 2 further domains concerning physical and psychological health. Despite this, there is no difference between the 2 versions. Therefore, in agreement with the originators, the reference values were used in the analysis of differences in satisfaction concerning the items common in the 2 versions.
The results of our study should not be generalized to the entire stroke population. The study group was dominated by patients with mild stroke, and focused on younger cohabiting couples. However, the current trend in the Western world of decreasing severity of stroke (32) and the increase in stroke incidence among younger people (33) points to the importance of studies emphasizing these groups.
This study was explorative. The level of significance was chosen to be 0.05, to be able to identify possible patterns of relationships. Because of the rather small study group in combination with multiple statistical analyses, a balance between the risks of type I and type II errors must be considered. The statistical significances should therefore be interpreted with care and be regarded only as indications of possible relationships and patterns. A focus should also be on the trends and patterns found in the results. In matched pair studies, non-respondents pose a special problem, because if one partner drops out, the other is also lost. It could be assumed that non-respondents either experience a high level of impairment and stress or have made good recovery, which has been found in previous studies of stressful life events (34).
Studies have shown that support should focus on the needs of both patients and spouses (35). Information provision and counselling should be grounded on patients’ and spouses’ individual needs, rather than based on pre-structured programs, and be focused on active problem solving strategies and support seeking behaviour in the couples (35). The results of our study are in congruence with the above-mentioned research findings. Furthermore, extended rehabilitation services including wider areas of life than self-care ability should be offered to the patients and their spouses, even for those with an apparently mild stroke.
ACKNOWLEDGEMENTS
This study was supported by grants from the Committee for Mental and Physical Disabilities in Region Västra Götaland, Sweden, the Swedish Association for the Neurologically Disabled (NHR), the Rune and Ulla Amlov Foundation for Neurological and Rheumatological Research, and the John and Brit Wennerstrom Foundation for Neurological Research. We thank Professor K. S. Fugl-Meyer for making available data collected in the Swedish population study of life satisfaction. We thank Martin Gellerstedt, biostatistician, for his valuable help and discussion on the statistical analyses. We also thank Magnus Pettersson, MS Statistics, biostatistician at Statistics Consultants, for his help with the worst-case/best-case scenario analyses.
Some of the results were published as a poster in the Nordic Stroke Conference held in Göteborg, Sweden, in September 2005.
REFERENCES
1. Wilkinson PR, Wolfe CD, Warburton FG, Rudd AG, Howard RS, Ross-Russell RW, et al. Longer term quality of life and outcome in stroke patients: is the Barthel index alone an adequate measure of outcome? Qual Health Care 1997; 6: 125–130.
2. Fuhrer MJ. Subjective well-being: implications for medical rehabilitation outcomes and models of disablement. Am J Phys Med Rehabil 1994; 73: 358–364.
3. Musschenga AW. The relation between concepts of quality-of-life, health and happiness. J Med Philos 1997; 22: 11–28.
4. Cohen E. A facet theory approach to examining overall and life facet satisfaction relationships. Soc Indic Res 2000; 51: 223–237.
5. Palmer S, Glass T. Family function and stroke recovery: a review. Rehabil Psychol 2003; 48: 255–265.
6. Mercier L, Audet T, Hebert R, Rochette A, Dubois MF. Impact of motor, cognitive, and perceptual disorders on ability to perform activities of daily living after stroke. Stroke 2001; 32: 2602–2608.
7. Carlsson GE, Möller A, Blomstrand C. Consequences of mild stroke in persons < 75 years – a 1-year follow-up. Cerebrovasc Dis 2003; 16: 383–388.
8. Robinson RG. Poststroke depression: prevalence, diagnosis, treatment, and disease progression. Biol Psychiatry 2003; 54: 376–387.
9. Forsberg-Wärleby G, Möller A, Blomstrand C. Life satisfaction in spouses of patients with stroke during the first year after stroke. J Rehabil Med 2004; 36: 4–11.
10. Jonsson AC, Lindgren I, Hallstrom B, Norrving B, Lindgren A. Determinants of quality of life in stroke survivors and their informal caregivers. Stroke 2005; 36: 803–808.
11. Bluvol A. The Codman Award Paper: quality of life in stroke survivors and their spouses: predictors and clinical implications for rehabilitation teams. Axone 2003; 25: 10–19.
12. Eriksson G, Tham K, Fugl-Meyer A. Couples’ happiness and its relationship to functioning in everyday life after brain injury. Scand J Occup Ther 2005; 13: 40–48.
13. Forsberg-Wärleby G, Möller A, Blomstrand C. Spouses of first-ever stroke patients: their view of the future during the first phase after stroke. Clin Rehabil 2002; 16: 506–514.
14. Multicenter trial of hemodilution in ischemic stroke-background and study protocol. Scandinavian Stroke Study Group. Stroke 1985; 16: 885–890.
15. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975; 12: 189–198.
16. Cook D, Casillas A, Robbins S, Dougherty L. Goal continuity and the “big Five” as predictors of older adult marital adjustment. Personality and Individual Differences 2005; 38: 519–531.
17. Mahoney FI, Barthel DW. Functional Evaluation: The Barthel Index. Md State Med J 1965; 14: 61–65.
18. Bamford JM, Sandercock PA, Warlow CP, Slattery J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1989; 20: 828.
19. Lindqvist G, Malmgren H. Organic mental disorders as hypothetical pathogenetic processes. Acta Psychiatr Scand Suppl 1993; 373: 5–17.
20. Fugl-Meyer A, Bränholm I, Fugl-Meyer K. Happiness and domain specific life satisfaction in adult northern Swedes. Clin Rehabil 1991; 5: 25–33.
21. Fugl-Meyer K. Health, sexual ability and quality of life. In: Lewin B, editor. Sex in Sweden. Stockholm: Swedish National Institute of Public Health 2000: p. 217–234.
22. O’Rourke N, Cappeliez P. Marital satisfaction and marital aggrandizement among older adults: analyses of gender invariance. Measurement and Evaluation in Counselling and Development 2001; 34: 66–78.
23. Houlihan M, Jackson J, Rogers T. Decision making of satisfied and dissatisfied married couples. J Soc Psychology 2001; 130: 89–102.
24. Acitelli LK, Badr H. My illness or our illness? Attending to the relationship when one partner is ill. In: Revenson TA, Kayser K, Bodenmann G, editors. Couples coping with stress. Emerging perspectives on dyadic coping. Decade of behavior. Washington DC: American Psychological Association; 2005.
25. Teasdale TW, Engberg AW. Psychosocial consequences of stroke: a long-term population-based follow-up. Brain Inj 2005; 19: 1049–1058.
26. Fugl-Meyer AR, Melin R, Fugl-Meyer KS. Life satisfaction in 18- to 64-year-old Swedes: in relation to gender, age, partner and immigrant status. J Rehabil Med 2002; 34: 239–246.
27. Korpelainen JT, Nieminen P, Myllyla VV. Sexual functioning among stroke patients and their spouses. Stroke 1999; 30: 715–719.
28. Carlsson GE, Möller A, Blomstrand C. A qualitative study of the consequences of ‘hidden dysfunctions’ one year after a mild stroke in persons < 75 years. Disabil Rehabil 2004; 26: 1373–1380.
29. Armistead L, Klein K, Forehand R. Parental physical illness and child functioning. Clinical Psychol Rev 1995; 15: 409–422.
30. Korneluk YG, Lee CM. Children’s adjustment to parental physical illness. Clin Child Fam Psychol Rev 1998; 1: 179–193.
31. Visser-Meily A, Post M, Meijer AM, Maas C, Ketelaar M, Lindeman E. Children’s adjustment to a parent’s stroke: determinants of health status and psychological problems, and the role of support from the rehabilitation team. J Rehabil Med 2005; 37: 236–241.
32. Rothwell PM, Coull AJ, Giles MF, Howard SC, Silver LE, Bull LM, et al. Change in stroke incidence, mortality, case-fatality, severity, and risk factors in Oxfordshire, UK from 1981 to 2004 (Oxford Vascular Study). Lancet 2004; 363: 1925–1933.
33. Medin J, Nordlund A, Ekberg K. Increasing stroke incidence in Sweden between 1989 and 2000 among persons aged 30 to 65 years: evidence from the Swedish Hospital Discharge Register. Stroke 2004; 35:1047–1051.
34. Weisaeth L. Importance of high response rates in traumatic stress research. Acta Psychiatr Scand Suppl 1989; 355: 131–137.
35. Visser-Meily A, van Heugten C, Post M, Schepers V, Lindeman E. Intervention studies for caregivers of stroke survivors: a critical review. Patient Educ Couns 2005; 56: 257–267.