OBJECTIVE: To investigate the association of muscle function and subgroups of low back pain (no low back pain, pelvic girdle pain, lumbar pain and combined pelvic girdle pain and lumbar pain) in relation to pregnancy.
DESIGN: Prospective cohort study.
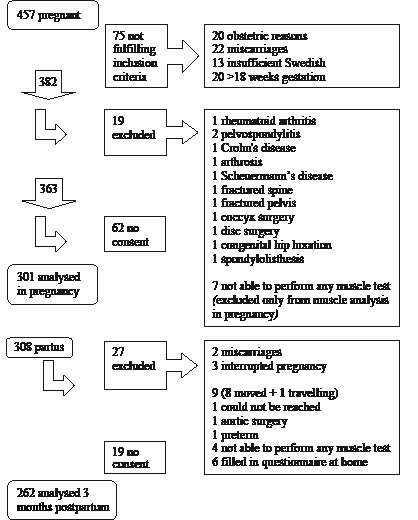
SUBJECTS: Consecutively enrolled pregnant women seen in gestational weeks 12–18 (n = 301) and 3 months postpartum (n = 262).
METHODS: Classification into subgroups by means of mechanical assessment of the lumbar spine, pelvic pain provocation tests, standard history and a pain drawing. Trunk muscle endurance, hip muscle strength (dynamometer) and gait speed were investigated.
RESULTS: In pregnancy 116 women had no low back pain, 33% (n = 99) had pelvic girdle pain, 11% (n = 32) had lumbar pain and 18% (n = 54) had combined pelvic girdle pain and lumbar pain. The prevalence of pelvic girdle pain/combined pelvic girdle pain and lumbar pain decreased postpartum, whereas the prevalence of lumbar pain remained stable. Women with pelvic girdle pain and/or combined pelvic girdle pain and lumbar pain had lower values for trunk muscle endurance, hip extension and gait speed as compared to women without low back pain in pregnancy and postpartum (p < 0.001–0.04). Women with pelvic girdle pain throughout the study had lower values of back flexor endurance compared with women without low back pain.
CONCLUSION: Muscle dysfunction was associated with pelvic girdle pain, which should be taken into consideration when developing treatment strategies and preventive measures.
Key words: low back pain, pelvic girdle pain, lumbar pain, muscle function, gait, pregnancy, postpartum.
J Rehabil Med 2008; 40: 304–311
Correspondence address: Annelie Gutke, Department of Medicine and Health Sciences, Division of Physiotherapy, Linköping University, SE-581 83 Linköping, Sweden. E-mail: annelie.gutke@ihs.liu.se
Submitted November 29, 2006; accepted December 3, 2007
Introduction
Identification of subgroups of patients with low back pain (LBP) has been recommended in order to develop specific treatment strategies (1). LBP is a common complication of pregnancy and a subgroup of LBP, pelvic girdle pain (PGP), is often related to pregnancy, whereas pregnancy seems to have little impact on the subgroup of patients with pain of lumbar origin (2). PGP is experienced between the posterior iliac crest and the gluteal fold, predominantly near the sacroiliac joints, and can radiate to the posterior thigh. Pain can also be experienced in conjunction with, or exclusively in, the symphysis (3). Functionally, women with PGP often complain of increased pain when walking (4, 5). Women with PGP have a different clinical presentation from that of women with lumbar pain (5–7). In order to identify possible differences in management, both subgroups need further investigation in relation to pregnancy.
According to guidelines, PGP classification requires exclusion of lumbar causes (3). Several tests for examination of the lumbar spine in pregnancy have been described (6–8), but the test reaction in terms of pain or stiffness is not specific enough to exclude intervertebral disc pathology, probably the most common structural source of non-specific LBP (9). Based on current knowledge and existing guidelines (3, 10), a clinical evaluation of pregnancy-related LBP should include pelvic pain provocation tests and a neurological examination, take known characteristics of PGP and lumbar pain into account and be sufficient to identify discogenic pain and red flag conditions.
Low endurance of back and hip muscle has been reported postpartum in women with longstanding PGP and lumbar pain (5). It was indicated that muscular dysfunction may be an important factor in persistent problems. It is unknown whether the reported dysfunction was developed due to longstanding problems or whether the women already had muscular dysfunction early in pregnancy.
In a theoretical model, a self-locking mechanism of the pelvic joints based on the principles of form and force closure was described (11). Force closure refers to the compressive forces needed sufficiently to stabilize the closely fitting sacroiliac joint (SIJ) surfaces making up the form closure. When the muscular capacity and the tension of the ligaments are inadequate, decreased compression across the SIJ will occur, insufficient stability will follow, and optimal load transfer between the back and legs will be compromised (12). In pregnancy the dynamic stability of the pelvis may be altered due to hormonally induced ligament laxity. Back extensors (13), abdominals (14) and hip extensors (13) are important muscles of force closure and stabilizing exercises improve muscle function, pain and functioning in women with PGP (15, 16). The hypothesis of muscular dysfunction in PGP requires investigation of muscle function in pregnancy.
The aim of this study was to investigate the association of muscle function and subgroups of LBP (no LBP, PGP, lumbar pain and combined PGP and lumbar pain) in relation to pregnancy.
Methods
Study participants
The Swedish antenatal healthcare system serves nearly 100% of the country’s pregnant women. Our cohort comprised all pregnant women consecutively registered at 2 antenatal care clinics in a community of 26,000 people. Swedish-speaking women who were expected to have a normal pregnancy (as determined by midwives) were approached for participation between gestational weeks 12 and 18. Participants received written and verbal information about the study from their midwife before giving oral consent. Women were excluded if they had a systemic locomotor system disease, verified diagnosis of spinal problems in the previous 2 months, or a history of fracture, neoplasm, or spinal, pelvic or femur surgery. The regional ethics committee approved the study (ö 414-00). Between August 2001 and September 2003 a cohort of 457 pregnant women attended the 2 antenatal care clinics in the community, and 308 were included in the study (17% declined participation, Fig. 1). Seven women were unable to perform any muscle tests in pregnancy and therefore excluded from this analysis, but were kept in the cohort for the postpartum analysis. At the evaluation between weeks 12 and 18, 116/301 (39%) women were classified as having no LBP and 185/301 (61%) as having some form of LBP. The women with LBP were classified into 3 subgroups: PGP (99/301, 33%), lumbar pain (32/301, 10%) and combined PGP and lumbar pain (54/301, 18%).
Fig. 1. Enrolment at evaluations between gestational weeks 12 and 18, and at 3 months postpartum.
Assessment
All participants completed questionnaires and were physically evaluated by one physiotherapist (AG) at a primary care clinic during gestational weeks 12–18 and again 3 months after giving birth. The questionnaires included background data and questions about household/leisure activity levels (17) (Table I).
| Table I. Characteristics for the women at the evaluation between gestational weeks 12–18 and at 3 months postpartum |
| Variables | Total n = 301 | No low back pain n = 116 | Lumbar pain n = 32 | Pelvic girdle pain n = 99 | Combined pain n = 54 |
| During pregnancy | | | | | |
| Age (years), median (range) | 29 (17–44) | 29 (20–39) | 30 (19–37) | 28 (18–44) | 28 (17–41) |
| Gestational week at inclusion, median (25,75 percentile) | 15 (14–16) | 15 (14–16) | 15 (14–16) | 15 (14–16) | 15 (14–16) |
| BMI, median (25,75 quartile) | 24 (22–27) | 24 (22–27) | 24 (22–26) | 24 (23–28) | 25 (23–28) |
| Parity, median (range) | 1 (0–4) | 1 (0–4) | 0.5 (0–2) | 1 (0–4) | 1 (0–3) |
| Urine leakage, n (%) | 60 (20) | 22 (19) | 1 (3) | 19 (19) | 18 (33) |
| Fulltime employment, n (%) | 153 (51) | 65 (56) | 20 (64) | 44 (45) | 24 (45) |
| Activity level last 6 months, n (%) 0–3 = household, gardening, light physical activity 4–6 = the above + exercise at increasing intensity | 207 (69) 93 (31) | 77 (67) 38 (33) | 25 (78) 7 (22) | 67 (68) 32 (32) | 38 (70) 16 (30) |
| Low back pain before first pregnancy, n (%) | 119 (40) | 30 (26) | 24 (75) | 36 (36) | 29 (54) |
| Post-partum | n = 262 | n = 176 | n = 27 | n = 45 | n = 14 |
| Weight of newborn (grams), mean (SD) | 3689 (542) | 3682 (520) | 3770 (436) | 3642 (656) | 3777 (624) |
| Delivery method caesarean, n (%) | 21 (8) | 11 (6) | 2 (7) | 5 (11) | 3 (21) |
| BMI, median (25, 75 quartile) | 25 (22–28) | 24 (22–28) | 26 (24–28) | 26 (24–30) | 25 (24–27) |
| Combined pain: combined pelvic girdle and lumbar pain. BMI: body mass index; SD: standard deviation. |
Classification into subgroups of low back pain
Participants were assigned to one of 4 groups based on the type of pain experienced: no LBP, PGP, lumbar pain, and combined PGP and lumbar pain (combined pain). Participants were assigned to the no LBP group if they had no subjective LBP complaint or fewer than 2 positive pelvic pain provocation tests and no lumbar pain or change in range of motion from repeated movements, according to the Mechanical Diagnosis and Therapy (MDT) classification (18). Assignment to the 3 LBP groups was made following examination by a specialized physiotherapist (AG). The examination included a standard history that focused on characteristics of lumbar pain (18) and PGP (2, 4, 6), mechanical assessment of the lumbar spine based on the MDT protocol, pelvic pain provocation tests (distraction test, posterior pelvic pain provocation test bilaterally, Gaenslen’s test bilaterally, compression test, sacral thrust) (19), the active straight leg raising test (20), neurological examination (muscle testing, reflex testing in the lower extremities, sensation and the straight leg raising test) and a hip rotation range-of-motion test. Pain location was indicated by participants on a pain drawing. The procedures and the 5 pelvic pain provocation tests are described in a previous publication (19).
Criteria for PGP were 2 or more positive pelvic pain provocation tests, the absence of centralization or peripheralization phenomena during repeated movement assessment (18, 21) and no lumbar pain or change in range of motion from repeated movements according to the MDT classifications. PGP onset was during pregnancy or within 3 weeks after delivery (4).
Lumbar pain was classified based on change in pain and/or a change in range of motion from repeated movements or different positions of the lumbar spine or based on experience of centralization and peripheralization phenomena during examination and fewer than 2 positive pelvic pain provocation tests.
Participants in the combined pain group had 2 or more positive pelvic pain provocation tests as well as a change in pain and/or a change in range of motion from repeated movements/different positions of the lumbar spine or experienced centralization and peripheralization phenomena.
In order further to analyse the possible association between muscle function and PGP, analyses based on the course of PGP were carried out. The analysed subgroups were: (i) no PGP in pregnancy or postpartum (n = 87), (ii) no PGP at first evaluation in pregnancy-week 12–18, but developed PGP later in pregnancy or postpartum (n = 9), (iii) PGP in pregnancy but no PGP postpartum, i.e. recovered (n = 55), and (iv) PGP both in pregnancy and postpartum (n = 18).
Physical functioning
We assessed muscle function with the identical procedure in pregnancy and in postpartum as follows: the gait test (modified from Ljungquist et al. (22)), maximal voluntary isometric hip extension (Fig. 2), and isometric endurance of back flexors (modified from McQuade et al. (23)). At the evaluation 3 months postpartum, a test of isometric endurance of back extensors (24) was added. This test was considered inappropriate in pregnancy due to the pressure on the lower abdomen. Pain intensity was rated on a visual analogue scale (0–100 mm) before and after each test.
For various reasons certain muscle tests were sometimes inappropriate (e.g. participants reported discomfort during tests in the prone position due to pregnancy, they felt sick, premature uterine contractions, there was a risk that discogenic problems would become worse, pain, and the subject’s lack of time). Pain as the reason for not participating in the tests in pregnancy was at most 2/54 (4%) in the combined pain group and postpartum 1/27 (4%) in the lumbar pain group.
Back flexors. To test isometric endurance of back flexors, participants laid supine with arms crossed over the chest, hands on the opposite shoulders, hips bent, and knees and feet apart. Participants were asked to nod and continue to lift their head and shoulders until the inferior angle of the scapula was lifted from the couch, and maintain the position as long as possible (modified from McQuade et al. (23)). We recorded the number of seconds that the position was maintained for a maximum of 120 sec.
Back extensors. To measure the isometric endurance of the back extensors, participants lay prone with their arms crossed and the trunk horizontal off the couch. The pelvis was fixed to the couch by straps and the lower legs were held in place by the tester (modified from Biering-Sörensen (24)). The time that this position was maintained was recorded in seconds and the test was discontinued after a maximum of 120 sec.
Hip muscles. Maximal voluntary isometric hip extension (Fig. 2) was measured with a dynamometer (Chatillon CSD 500 strength dynamometer, Ametek, Largo, FL, USA) with a fixed sensor. Each participant held a sling around the thigh at the distal end of the femur and pulled in hip extension. Participants were instructed to “pull as hard as you can until I stop you after 5 sec”. No encouragement was given during the tests. Participants started with the right leg. Two training repetitions were performed and the mean of the next 3 repetitions was analysed. Each repetition consisted of 5 sec of activity and 5–10 sec of rest. The same procedure was repeated on the left side.
Fig. 2. The hip extension test, left side.
Gait. Activity limitation when walking was studied in a gait test (modified from Ljungquist et al. (22)). The participants were asked to walk barefoot for a distance of 20 m “at a comfortable speed” on a horizontal indoor floor. The “natural customary walking speed” is considered to result in the least mechanical and physiological expenditure (25). The time (in sec) it took to travel 20 m was recorded.
Reliability. The reliability of the hip muscle extension test was investigated in a pilot study (n = 20). Spearman’s rho was 0.82 for the right leg and 0.88 for the left leg; the intercorrelation coefficient (model 2) was 0.87 for the right leg and 0.85 for the left leg. The measurement error was 53 N on the right leg and 50 N on the left leg. The measurement error was 15% of the range of hip extension values. In a small unpublished study, the above classification protocol was reliability tested on 31 pregnant women (mean age 28 years, range 20–36; median gestational week 26, range 13–38) with some type of LBP, by 2 independent examiners, specialized in LBP. Agreement between examiners for the 3 syndromes (lumbar pain, PGP, combined pain) was 87% (27/31), giving a substantial kappa coefficient of 0.79.
Statistics
In analyses of continuous parametric variables for the 4 groups, a one-way ANOVA was performed. In analyses of non-parametric data on a nominal level, the χ2 test was used, and for data on an ordinal level the Kruskal-Wallis test for multi-group comparisons was used. Correction for multiple analyses was made using the Bonferroni correction. General Linear Model analyses were performed to evaluate the association between muscle test results and classification group when controlling for pain intensity.
The power to detect a 20% difference in back flexors was 52% (pregnancy) and 39% (postpartum); for back extensors it was 69% and for hip extensors it was 94%. Statistical significance was accepted at alpha level 0.05. The statistical software package used was SPSS 11.0.
Results
At the postpartum evaluation, 41 of the women had delivered but were not included in the analysis (Fig. 1). Out of those 41 women 19 declined to participate due to a lack of time, feeling too tired or without giving a reason. Postpartum, 262 women remained for analysis (Fig. 1). The 41 women not included in the postpartum analysis did not differ from the 262 women in the analysis regarding age, parity, body mass index (BMI), back pain before first pregnancy, whether LBP impeded work, exercise frequency or muscle function. The 41 women were less active (p = 0.03) than the 262 women in the analysis.
Postpartum one-third of the women (86/262, 33%) had LBP, with the subgroups as follows: PGP (45/262, 17%), lumbar pain (27/262, 10%) and combined PGP and lumbar pain (14/262, 6%).
Back flexors
Early in pregnancy, the women with PGP had lower endurance of back flexor muscles as compared to the women without LBP (mean difference 17.9 sec, p = 0.001, Table II). Postpartum, the women with combined PGP and lumbar pain had lower endurance of back flexor muscles compared with the women without LBP (mean difference 33 sec, p = 0.01, Table III).
| Table II. Muscle test results in pregnancy in the four groups based on type of low back pain: no low back pain, lumbar pain, pelvic girdle pain and combined pelvic girdle pain and lumbar pain (combined pain). Values are given as mean (95% confidence interval) |
| | 1 No low back pain n = 116 | 2 Lumbar pain n = 32 | 3 Pelvic girdle pain n = 99 | 4 Combined pain n = 54 | Group comparison* |
| Back flexor endurance, sec | n = 100 | n = 27 | n = 83 | n = 40 | |
| | 52.6 (45.9–59.3) | 40.1 (28.4–51.9) | 34.7 (28.9–40.5) | 41.0 (30.7–51.4) | 1–3, p = 0.001 |
| Hip extension right, N | n =112 | n = 31 | n = 91 | n = 49 | |
| | 275 (254–295) | 220 (186–253) | 221 (200–242) | 216 (188–244) | 1–3, p = 0.001 1–4, p 0.006 |
| Hip extension left, N | n = 111 | n = 31 | n = 90 | n = 49 | |
| | 254 (233–275) | 217 (182–251) | 209 (187–230) | 204 (177–232) | 1–3, p = 0.02 1–4, p = 0.04 |
| Gait speed, m/sec | n = 112 | n = 31 | n = 92 | n = 53 | |
| | 1.33 (1.30–1.36) | 1.31 (1.24–1.39) | 1.24 (1.20–1.29) | 1.25 (1.20–1.30) | 1–3, p = 0.008 |
| *p-values from ANOVA. All original 2-tailed p-values were multiplied by 6 (Bonferroni correction). Significant comparisons are shown. |
| Table III. Muscle test results postpartum in the 4 groups based on type of low back pain: no low back pain, lumbar pain, pelvic girdle pain and combined pelvic girdle pain and lumbar pain (combined pain). Values are given as mean (95% confidence interval) |
| | 1 No low back pain n = 176 | 2 Lumbar pain n = 27 | 3 Pelvic girdle pain n = 45 | 4 Combined pain n = 14 | Group comparison* |
| Back flexor endurance, sec | n = 166 | n = 20 | n = 44 | n = 12 | |
| 53.0 (47.4–58.6) | 56.5 (38.1–74.9) | 41.8 (30.9–52.7) | 20.0 (9.7–30.3) | 1–4, p = 0.01 2–4, p = 0.03 |
| Back extensor endurance, N | n = 162 | n = 17 | n = 36 | n = 9 | |
| 79.0 (73.7–84.4) | 59.8 (42.9–76.7) | 50.7 (39.1–62.3) | 56.3 (30.9–81.7) | 1–3, p < 0.001 |
| Hip extension right, N | n = 172 | n = 24 | n = 44 | n = 14 | |
| 256 (242–270) | 265 (219–311) | 211 (186–237) | 183 (156–210) | 1–3, p = 0.03 1–4, p = 0.03 |
| Hip extension left, N | n = 173 | n = 24 | n = 44 | n = 14 | |
| 239 (224–254) | 261 (209–313) | 217 (189–244) | 185 (148–222) | ns |
| Gait speed, m/sec | n = 171 | n = 21 | n = 44 | n = 12 | |
| 1.33 (1.31–1.36) | 1.27 (1.18–1.36) | 1.26 (1.21–1.30) | 1.28 (1.21–1.36) | 1–3, p = 0.03 |
| *p-values from ANOVA. All original 2-tailed p-values were multiplied by 6 (Bonferroni correction), Significant comparisons are shown. ns: not significant. |
Back extensors
The women with PGP had lower endurance of back extensor muscles compared with the women without LBP (mean difference 28.3 sec, p < 0.001, Table III).
Hip muscles
The women with PGP and those with combined PGP and lumbar pain had lower values for maximal voluntary isometric hip extension muscle strength (mean difference range 45–59 N for both legs in pregnancy; p = 0.001–0.04 Table II) and for the right leg postpartum (mean difference 45–73 N, p = 0.03, Table III) compared with the women without LBP. No pattern was found regarding dominant pain side and hip muscle results.
Gait
The women with PGP walked at a slower speed compared with the women without LBP both in pregnancy (mean difference 0.09 m/sec, p = 0.008, Table II) and postpartum (mean difference 0.07 m/sec, p = 0.03, Table III).
Pregnancy to postpartum
The women with PGP in early pregnancy as well as postpartum, had lower endurance of back flexor muscles compared with the women without LBP (Table IV).
Pain
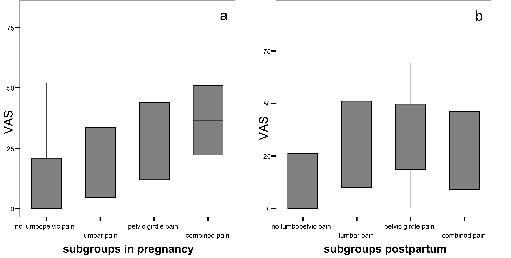
The general linear model analyses showed an association between classification group and trunk muscle endurance, hip extension muscle strength (bilateral in pregnancy and right leg postpartum), and gait speed (Table V). There was no significant difference in pain intensity between before and after the tests, which implies that the muscle tests did not cause increased pain. When controlling for pain differences before and after each test, the explanation of the association between muscle function and classification group did not improve. Thus the lower values in the tests of those women with some type of LBP could not be explained by an increase in pain during tests. Nor was there any improvement in the explanation when controlling for pre-test pain intensity (Fig. 3).
| Table V. Muscle test result in pregnancy. The cohort divided based on the course of the classification of pelvic girdle pain. Values are given as mean (95% confidence interval) |
| | 1 No PGP/no PGP n = 87 | 2 No PGP/PGP n = 9 | 3 PGP/no PGP n = 55 | 4 PGP/PGP n = 18 | Group comparison* |
| Back flexor endurance test, sec | n = 74 | n = 7 | n = 45 | n = 16 | 1–4, p = 0.03 |
| 52.5 (44.6–60.5) | 26.8 (0.3–53.3) | 41.5 (32.3–50.7) | 27.8 (17.1–38.5) | |
| Hip extension, right, N | n = 83 | n = 9 | n = 51 | n = 16 | ns |
| 270 (247–294) | 256 (207–305) | 230 (201–260) | 226 (171–281) | |
| Hip extension, left, N | n = 82 | n = 9 | n = 50 | n = 17 | ns |
| 247 (224–270) | 252 (191–312) | 210 (180–240) | 217 (158–277) | |
| Gait speed, m/sec | n = 83 | n = 9 | n = 53 | n = 15 | ns |
| 1.33 (1.29–1.36) | 1.34 (1.22–1.46) | 1.25 (1.19–1.31) | 1.29 (1.20–1.40) | |
| 1: no PGP in pregnancy or postpartum (n = 87). 2: no PGP at first evaluation in pregnancy-week 12–18, but developed PGP later in pregnancy or postpartum (n = 9). 3: PGP in pregnancy, but no PGP postpartum, i.e. recovered (n = 55). 4: PGP both in pregnancy and postpartum (n = 18). *p-values from ANOVA. All original 2-tailed p-values were multiplied by 6 (Bonferroni correction), significant comparisons are shown. ns: not significant. PGP: pelvic girdle pain. |
Fig. 3. Pre-test pain intensity on a 100-mm visual analogue scale (VAS) at evaluation (A) between gestational weeks 12 and 18 and (B) at 3 months postpartum. Pain intensity was regarded as an ordinal scale. The median value, the quartiles and the range of values are shown.
Discussion
The main findings of this study were that the women with PGP and/or combined PGP and lumbar pain had lower muscle function in trunk endurance and hip extension muscle strength as well as slower preferred gait speed compared with the women without LBP. The findings were seen early in pregnancy as well as postpartum. The women with PGP throughout the study had lower back flexor muscle endurance than the women who did not have LBP at any evaluation. The result strengthens the hypothesis that there is an association between muscle dysfunction and women who develop or have persistent PGP.
The studied cohort is representative considering the prevalence of LBP. Women with mild symptoms who nevertheless fulfilled the criteria for PGP and/or lumbar pain were classified in our study. It has been estimated that the overall prevalence of LBP in relation to pregnancy increases by 20% when women with mild symptoms are included (26).
One weakness of the study is the small size of the lumbar pain subgroup and the postpartum combined pain subgroup and thereby the statistical power of some of the muscle tests. Thus no conclusions can be drawn regarding the lumbar pain group or potential difference between PGP and lumbar pain. However, despite the low power for some tests there was a difference between women with PGP (in some tests women with combined pain) and women without LBP that suggest an association between muscle dysfunction and at least the subgroup of women with PGP in pregnancy. The dropouts in the separate tests are not expected to influence the results, since the reasons for not performing a test were mostly not related to the LBP per se but rather to pregnancy itself. Participants were asked to indicate spinal or pelvic pain location and its pain intensity (Figs 3 and 4). The women with no LBP could experience pain in other locations as the neck or thoracic spine. This may have weakened the comparison of subgroups and may have resulted in an underestimation of the difference.
Pelvic pain provocation tests are often used to identify PGP (5, 6, 27). Most authors identify and exclude women with lumbar pain by means of a neurological test and/or a test of spinal range of motion, but the test reaction in terms of pain or stiffness is not specific. Using the pelvic pain provocation tests within the context of the standardized mechanical assessment of the lumbar spine as in the present study is of higher diagnostic value than pain provocation tests alone (28).
No study was found that had investigated muscle function in pregnant women with LBP and thereby the comparison is with studies on non-pregnant persons with LBP. Several studies suggest an association between non-pregnancy-related SIJ pain and decreased stability of the pelvis due to dysfunction of the muscles contributing to force closure of the pelvic joints (12–14, 29, 30). When performing poorly on the back extensor muscle endurance test, defined as less than 58 sec, the odds ratio for developing LBP was reported to be 3.4 (31). The women with PGP in our study had mean endurance values below 58 sec, indicating that these subgroups might be at higher risk. Back extensors are reported to be important muscles for force closure of the SIJ (13) and low isometric endurance of the back extensors has been suggested as part of the aetiology of non-specific non-pregnancy-related LBP (5, 24, 31) as well as persistent combined PGP and lumbar pain (5). It has been proposed that the relationship is non-linear and that those performing the poorest are at greatest risk for back pain (31). The difference in back extensor endurance between women with PGP and women without LBP in our study strengthen the hypothesis of muscle dysfunction in PGP.
Likewise, our results from the back flexor muscle endurance test indicate that poor muscle function is associated with PGP in pregnancy. Early in pregnancy the women with PGP had below the cut-off point of 40 sec that has been proposed for discriminating between spinal pain and back-healthy persons (22). This indicates that muscle dysfunction is an early detectable prerequisite for developing PGP. Although only one comparison between women with persistent PGP and women with no LBP throughout the study was significant, the trend of lower values for PGP was consistent (Table IV). There was a tendency for women with moderate back flexor muscle endurance in early pregnancy to recover from PGP, while those with the poorest back flexor muscle endurance more often developed or had persistent symptoms (Table IV). The trunk muscle endurance test was discontinued after 120 sec. That is shorter than in other studies (22, 24), but was considered the most appropriate in pregnancy as well as 3 months postpartum. The ceiling effect (i.e. the proportion of women reaching the maximum test time) was 6 and11% (pregnancy and postpartum, respectively) for back flexors and 17% for the back extensor test postpartum. However, our conclusions did not change when the analysis was performed without those women reaching the maximum time.
| Table IV. Results from General Linear Model analyses in pregnancy and postpartum. The independent fixed factor was the subgroups of the cohort. In crude model 1 the association between muscle test results and the subgroups was analysed. In adjusted model 2 the difference in pain between before and after each test was added as covariate. In adjusted model 3 the pre-test pain intensity was added as covariate. The significant associations are shown |
| | Crude model 1 p-value | Adjusted model 2 for pain difference | Adjusted model 3 for pre-test pain |
| In pregnancy |
| Dependent Back flexor Fixed factor: subgroups of LBP | 0.002 | 0.001 | p = 0.014 |
| Dependent Hip extension, right Fixed factor: subgroups of LBP | < 0.001 | < 0.001 | p = 0.014 |
| Dependent Hip extension, left Fixed factor: subgroups of LBP | 0.006 | 0.006 | ns |
| Dependent Gait Fixed factor: subgroups of LBP | 0.004 | 0.005 | ns |
| Postpartum |
| Dependent Back flexor Fixed factor: subgroups of LBP | 0.007 | 0.008 | p = 0.017 |
| Dependent Back extensors Fixed factor: subgroups of LBP | < 0.001 | < 0.001 | ns |
| Dependent Hip extension, right Fixed factor: subgroups of LBP | 0.002 | 0.004 | p = 0.031 |
| Dependent Gait Fixed factor: subgroups of LBP | 0.019 | 0.020 | ns |
| LBP: low back pain; ns: not significant. Subgroups of LBP: no LBP, lumbar pain, pelvic girdle pain, combined pelvic girdle and lumbar pain. |
Studying muscle function while walking confirmed the gait difficulties previously reported by women with PGP (4, 5). Even early in pregnancy, the women with PGP walked at a slower speed than the women without LBP. The gait speed was below the cut-off level of 1.3 m/sec that has been proposed to differentiate between patients with LBP and healthy persons (22).
Muscle function was investigated 3 years postpartum in a study with similar subgroups as in the present study (5). The reported increased difficulty in walking among women with persistent PGP or combined pain is supported by the gait test in the present study. The women with persistent combined pain in the study by Noren et al. (5) had significantly reduced back extensor endurance compared with the women with PGP or lumbar pain. The women with combined pain in our study had a mean value below 58 sec, but the difference did not reach a significant level, which may be due to the small groups. The disparity in findings between the 2 studies may also be caused by our shorter follow-up.
Muscle test result was associated with classification of LBP in the general linear model analyses. When adding the pain difference between before and after each test no further explanation of the association between classification and muscle test result was seen. We also wanted to study whether pre-test pain intensity could further explain the association. When adding pre-test pain intensity to the model no improvement in the explanation was seen, which implies that pre-test pain intensity did not further explain the association. Consequently, the explanation for the difference in test results between women without LBP and those with PGP and/or combined pain must mainly be differences in muscle function. Additionally, we do not state that women with PGP have muscle weakness, but rather that they could not perform the test as well as the women without LBP, and that the result was not explained by pain intensity. Further studies are needed to understand the cause.
In the present study, many of the women with PGP at the first evaluation had a short duration of their current symptoms, suggesting that the muscle dysfunction was present before pain onset. The combined effect of the muscle dysfunction identified in this study and the hormone-induced increased ligament and joint capsule laxity in pregnancy may increase the risk of insufficient force closure of the pelvis (12), resulting in pain. The present study suggests that one of the components probably required for developing PGP, i.e. muscle dysfunction, can be identified early in pregnancy.
The mechanism to explain the association between muscle function and LBP in relation to pregnancy is not clear. The clarification of background mechanism needs multidisciplinary research, not only in mechanical, but also taking into consideration hormonal pathophysiology, although the role of individual hormone variations and pregnancy-related LBP is as yet uncertain. In that way it enables appropriate prevention and therapy.
The idea that impaired stability is due to altered force closure of the pelvis has been converted into treatment strategies for PGP with specific stabilizing exercises (32). The strategy has been shown to decrease symptoms of PGP during pregnancy (16) as well as afterwards (27). Back extensor muscle endurance as well as hip muscle strength has shown significant improvement after exercise therapy in muscle function as well as in pain intensity and function (27). Although there were some differences in test performance in the now mentioned study by Stuge et al. and the present study, the results of the back extensor test at baseline postpartum were similar. The hypothesis of muscle dysfunction in women with PGP is supported by our new findings, irrespective of having PGP in early pregnancy or having persistent PGP postpartum.
AcknowledgementS
This study was supported by grants from The Swedish Research Council, The Vardal Foundation, Foundation of the Region Västra Götaland, Trygg Hansa Research Foundation, and The Rehabilitation and Medical Research Foundation. We thank Olle Ericsson for statistical advice.
References
1. Borkan JM, Koes B, Reis S, Cherkin DC. A report from the Second International Forum for Primary Care Research on Low Back Pain. Re-examining priorities. Spine 1998; 23: 1992–1996.
2. Ostgaard HC, Roos-Hansson E, Zetherstrom G. Regression of back and posterior pelvic pain after pregnancy. Spine 1996; 21: 2777–2780.
3. Vleeming A, Albert H, Östgaard H, Stuge B, Sturesson B. European guidelines on the diagnosis and treatment of pelvic girdle pain, 2005. Eur Spine J in press 2008.
4. Mens JM, Vleeming A, Stoeckart R, Stam HJ, Snijders CJ. Understanding peripartum pelvic pain. Implications of a patient survey. Spine 1996; 21: 1363–1369; discussion 1369–1370.
5. Noren L, Ostgaard S, Johansson G, Ostgaard HC. Lumbar back and posterior pelvic pain during pregnancy: a 3-year follow-up. Eur Spine J 2002; 11: 267–271.
6. Sturesson B, Uden G, Uden A. Pain pattern in pregnancy and “catching” of the leg in pregnant women with posterior pelvic pain. Spine 1997; 22: 1880–1883; discussion 1884.
7. Ostgaard HC, Zetherstrom G, Roos-Hansson E, Svanberg B. Reduction of back and posterior pelvic pain in pregnancy. Spine 1994; 19: 894–900.
8. Kristiansson P, Svardsudd K. Discriminatory power of tests applied in back pain during pregnancy. Spine 1996; 21: 2337–2343; discussion 2343–2344.
9. Schwarzer AC, Aprill CN, Derby R, Fortin J, Kine G, Bogduk N. The prevalence and clinical features of internal disc disruption in patients with chronic low back pain. Spine 1995; 20: 1878–1883.
10. van Tulder M, Becker A, Bekkering T, Breen A, del Real MT, Hutchinson A, et al. Chapter 3. European guidelines for the management of acute nonspecific low back pain in primary care. Eur Spine J 2006; 15 Suppl 2: S169–S191.
11. Vleeming A, Snijders C, Stoeckart R, Mens JM. The role of the sacroiliac joints in coupling between spine, pelvis, legs and arms. In: Vleeming A, Mooney V, Dorman T, Snijders C, Stoeckart R, editors. Movement, stability & low back pain. The essential role of the pelvis. London: Churchill Livingstone; 1997, p. 53–71.
12. Pool-Goudzwaard AL, Vleeming A, Stoeckart R, Snijders CJ, Mens JM. Insufficient lumbopelvic stability: a clinical, anatomical and biomechanical approach to ‘a-specific’ low back pain. Man Ther 1998; 3: 12–20.
13. van Wingerden JP, Vleeming A, Buyruk HM, Raissadat K. Stabilization of the sacroiliac joint in vivo: verification of muscular contribution to force closure of the pelvis. Eur Spine J 2004; 13: 199–205.
14. Richardson CA, Snijders CJ, Hides JA, Damen L, Pas MS, Storm J. The relation between the transversus abdominis muscles, sacroiliac joint mechanics, and low back pain. Spine 2002; 27: 399–405.
15. Stuge B, Veierod MB, Laerum E, Vollestad N. The efficacy of a treatment program focusing on specific stabilizing exercises for pelvic girdle pain after pregnancy: a two-year follow-up of a randomized clinical trial. Spine 2004; 29: E197–E203.
16. Elden H, Ladfors L, Olsen MF, Ostgaard HC, Hagberg H. Effects of acupuncture and stabilising exercises as adjunct to standard treatment in pregnant women with pelvic girdle pain: randomised single blind controlled trial. BMJ 2005; 330: 761.
17. Frändin K, editor. Physical activity and functional performance in a population studied longitudinally from 70 to 75 years of age. Gothenburg: Göteborg University; 1995.
18. McKenzie R, May S, editors. The lumbar spine. Mechanical diagnosis & therapy. Waikanae: Spinal Publications New Zealand Ltd; 2003.
19. Gutke A, Ostgaard HC, Oberg B. Pelvic girdle pain and lumbar pain in pregnancy: a cohort study of the consequences in terms of health and functioning. Spine 2006; 31: E149–E155.
20. Mens JM, Vleeming A, Snijders CJ, Stam HJ, Ginai AZ. The active straight leg raising test and mobility of the pelvic joints. Eur Spine J 1999; 8: 468–474.
21. Donelson R, Silva G, Murphy K. Centralization phenomenon. Its usefulness in evaluating and treating referred pain. Spine 1990; 15: 211–213.
22. Ljungquist T, Fransson B, Harms-Ringdahl K, Bjornham A, Nygren A. A physiotherapy test package for assessing back and neck dysfunction – discriminative ability for patients versus healthy control subjects. Physiother Res Int 1999; 4: 123–140.
23. McQuade KJ, Turner JA, Buchner DM. Physical fitness and chronic low back pain. An analysis of the relationships among fitness, functional limitations, and depression. Clin Orthop Relat Res 1988: 198–204.
24. Biering-Sörensen F. Physical measurements as risk indicators for low-back trouble over a one-year period. Spine 1984; 9: 106–119.
25. Waters RL, Lunsford BR, Perry J, Byrd R. Energy-speed relationship of walking: standard tables. J Orthop Res 1988; 6: 215–222.
26. Wu WH, Meijer OG, Uegaki K, Mens JM, van Dieen JH, Wuisman PI, et al. Pregnancy-related pelvic girdle pain (PPP), I: terminology, clinical presentation, and prevalence. Eur Spine J 2004; 13: 575–589.
27. Stuge B, Laerum E, Kirkesola G, Vollestad N. The efficacy of a treatment program focusing on specific stabilizing exercises for pelvic girdle pain after pregnancy: a randomized controlled trial. Spine 2004; 29: 351–359.
28. Laslett M, Young SB, Aprill CN, McDonald B. Diagnosing painful sacroiliac joints: a validity study of a McKenzie evaluation and sacroiliac provocation tests. Aust J Physiother 2003; 49: 89–97.
29. O’Sullivan PB, Beales DJ, Beetham JA, Cripps J, Graf F, Lin IB, et al. Altered motor control strategies in subjects with sacroiliac joint pain during the active straight-leg-raise test. Spine 2002; 27: E1–E8.
30. Hungerford B, Gilleard W, Hodges P. Evidence of altered lumbopelvic muscle recruitment in the presence of sacroiliac joint pain. Spine 2003; 28: 1593–1600.
31. Alaranta H, Luoto S, Heliovaara M, Hurri H. Static back endurance and the risk of low-back pain. Clin Biomech (Bristol, Avon) 1995; 10: 323–324.
32. Richardson CA, Jull GA. Muscle control-pain control. What exercises would you prescribe? Man Ther 2000; 1: 2–10.