OBJECTIVE: To explore and describe factors associated with occupational gaps and to identify factors at 3 months that predict occupational gaps one year post-stroke. A gap, a restriction in participation, is considered to be present when there is a discrepancy between what the individual wants to do and what they actually do in everyday life.
DESIGN: Prospective longitudinal study.
SUBJECTS: Two hundred persons with stroke.
METHODS: Data from the Occupational Gaps Questionnaire, one year post-stroke, was used as the dependent variable in 3- and 12-month regression analyses. Domains of the Stroke Impact Scale, global life satisfaction, demographic and medical factors were used as independent variables.
RESULTS: At 3 months, activities of daily living abilities, social participation and not being born in Sweden predicted occupational gaps at 12 months. Stroke severity and not being born in Sweden and 3 factors at 12 months: social participation, self-rated recovery, and global life satisfaction were associated with occupational gaps.
CONCLUSION: Activities of daily living ability at 3 months predicted occupational gaps after stroke. Thus, it is possible to identify early on, and provide interventions for, those that risk participation restrictions. Not being born in the country might be an indicator of a risk for participation restrictions.
Key words: stroke; social participation; activities of daily living; rehabilitation; occupational therapy.
J Rehabil Med 2012; 44: 36–42
Correspondence address: Aileen L. Bergström, Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, Karolinska Institutet, Box 23200, SE-141 83, Huddinge, Sweden. E-mail: Aileen.Bergstrom@ki.se
Submitted March 10, 2011; accepted August 23, 2011
Introduction
Participation in everyday occupations (1) is a dimension of the World Health Organization (WHO)’s term of participation, which is defined as involvement in a life situation (2). Participation in everyday occupations incorporates the term “occupations”, which is defined as groups of activities of everyday life that are given value and meaning by the individual (3). Participation is considered to have a positive influence on health and well-being and is vital for all humans (1). Participation is also considered to provide structure and meaning to daily life (4, 5) and leads to life satisfaction (1). Hence, maximizing persons’ participation is a goal for rehabilitation (6–8). Participation after a stroke has been explored in a number of studies with a number of different instruments (9–12). Research shows that the sequel of stroke affects community and social participation (9–11). However, little is known about participation in everyday occupations after stroke, and therefore this is the focus of this study.
It has been shown in a number of studies that people with stroke still perceive participation restrictions 12 months after stroke onset (9–11, 13). The rehabilitation process after stroke takes time, and during the first year the needs of the individuals involved can change. A study by Mayo et al. (14) has shown that during the second half of the first year after stroke individuals perceived the effects of not being able to do usual activities, indicating that measuring participation in everyday occupations after stroke is relevant one year post-stroke. Several studies have focused on predictors of participation in general and at different time-points, i.e. 6 months post-discharge (9), 2–4 years post-discharge (10) and 2 years post-stroke (12). However, these studies do not have unanimous results and do not focus on participation in everyday occupations one year post-stroke.
Participation in everyday occupations, which includes the choosing and performing of activities desired by the person, has been operationalized and is measured in the Occupational Gaps Questionnaire (OGQ) (15). A gap, or a restriction in participation, is considered to be present when there is a discrepancy between what the individual wants to do and what he or she actually does. The number of occupational gaps was shown to have increased after acquired brain injury (ABI) (16). Furthermore, it was shown that there was a relationship between occupational gaps and life satisfaction for persons with ABI (15); however, there is no empirical evidence for this relationship for persons with stroke.
Considering the different factors focused on in stroke rehabilitation, such as physical functioning, activities of daily living (ADL)s, and life satisfaction, and the need for more knowledge regarding factors associated with participation (10) this study seeks to explore factors that predict persons at risk for occupational gaps. Thus, the aims of this study were to explore occupational gaps at 12 months after stroke and the factors associated with occupational gaps. The specific aims were:
• To describe the extent of occupational gaps at 12 months after stroke.
• To describe factors associated with occupational gaps at 12 months after stroke.
• To identify which factors at 3 months after stroke predict occupational gaps at 12 months after stroke.
Methods
This prospective longitudinal study was performed using data collected at inclusion and at 3 and 12 months post-stroke.
The participants in this study were part of a larger hospital-based study of all the persons with a stroke diagnosis admitted to the stroke units at Karolinska University Hospital, Stockholm, Sweden during the period of one year (May 2006 to May 2007). A total of 349 persons with a stroke diagnosis consented to involvement and constituted the main study. All study participants were informed both orally and in writing 3–5 days after the stroke and agreed to participate in the study. All descriptive characteristics and relevant medical information were extracted from the medical records. Other data were collected by specially trained research assistants (clinically experienced occupational and physical therapists) via standardized measures. Data at inclusion was collected on the stroke unit and at later time periods, in conjunction with a home visit or in the clinic by the research assistants. The criteria for inclusion in the present study were all persons in the main study that were administered the OGQ, one year post-stroke. The OGQ, administered as one instrument in a battery of standardized assessments, was considered the main outcome measure in the present study. The research assistant administering the assessments provided assistance in completing the questionnaire if needed.
This project was approved by the regional ethics committee, Stockholm, Sweden.
Instruments
Occupational Gap Questionnaire. OGQ (15, 16) is a checklist of 28 activities that deal with instrumental ADLs, work or work-related activities, leisure and social activities. There are two questions pertaining to each activity: (i) if the person performs the activity (yes/no), and (ii) if they wish to perform the same activity (yes/no). A gap is considered to be present when there is a discrepancy between the responses of the two questions. An optimal outcome is the absence of gaps (16).
Rasch analyses (17, 18) was performed on the raw scores of the OGQ to evaluate the psychometric properties before using the data in the statistical analyses. Rasch analysis converts raw scores into equal-interval measures or logits (log-odds probability units) and enables the use of the data in regression analyses. The results of the Rasch analysis demonstrated that the OGQ had acceptable internal scale validity, in that all 28 items demonstrated acceptable goodness-of-fit (mean square equal to or less than 1.4 with a corresponding z less than 2.0) (17). Person response validity was also acceptable, since all 200 persons demonstrated acceptable goodness-of-fit in their responses (mean square equal or less to 1.4 with a corresponding z less than 2.0) (18). Principal component analysis showed that the items explained 53% of the variance and that no additional factor explained more than 3.5%, indicating that the OGQ measured only one construct and was considered to be a valid estimation of occupational gaps in further analyses (19). The OGQ results in logits were used as the dependent variable in the analysis.
Stroke Impact Scale. The Stroke Impact Scale (SIS) 3.0 (20, 21) measures the perceived impact of stroke and is made up of 59 items in 8 different domains. SIS scores range from 0 to 100 and the greater the score, the less the impact. The physical function domain is a combined score of the strength, hand function, mobility, and ADL/instrumental activities of daily living domains (21). The perceived recovery is measured on a visual analogue scale from 0 to 100. Zero indicates no recovery and 100 full recovery (21). The SIS was administered to the study participants at 3 and 12 months post-stroke and a proxy version (22) was used when appropriate. The SIS domain scores of emotions, ADLs, participation, physical functions and recovery were used as independent variables in both the 3- and 12-month analyses.
Life Satisfaction Checklist. The Life Satisfaction Checklist (LiSat-11) (23) assesses overall life satisfaction. The full scale responses to the first question concerning global life satisfaction were used because of the encompassing scope of the question. The validity of using only the response to global life satisfaction has been confirmed (24). An ordinal self-rating scale ranging from (6) “very satisfying” to (1) “very dissatisfying” is used. The checklist was administered at one year post-stroke and the responses were used as an independent variable due to the associations of life satisfaction with participation.
Mini Mental State Examination. The Mini Mental State Examination (MMSE) (25) is a short standardized instrument designed for testing cognitive functions (25). The MMSE was administered at inclusion, the scores were dichotomized (≤ 23 vs ≥ 24), and used as an independent variable in the analysis.
Barthel Index. The Barthel Index (BI) (26, 27) measures 10 aspects of self-care and mobility. Scores range from 0 to 100, with a lower score indicating greater dependency. The BI, administered at inclusion, was used to determine stroke severity, where scores of 51–100 represented mild stroke, 15–50 moderate and ≤ 14 severe stroke (28).
Statistics
Descriptive statistics (means and standard deviations (SDs) for interval or ratio level data, median and quartile range/range for ordinal level data, numbers and percentages for nominal level data) were used to report the characteristics collected at inclusion and the results of the OGQ, BI, MMSE, SIS and the LiSat-11. Results from the OGQ were presented with raw scores for descriptive purposes, while the OGQ in logits were used in performing regression analyses.
Univariate regression analyses were performed to assess the association of occupational gaps with baseline factors: age, gender, born/not born in Sweden, MMSE dichotomized, and stroke severity, as well as factors at 3 and 12 months: the SIS domains of emotions, ADL/I-ADLs, participation, physical functions, self-rated recovery, and global life satisfaction at 12 months.
The results of the univariate regression analysis were used to guide the choice of which variables should be included in the multiple regression analysis, with the intention of exploring the association with the extent of occupational gaps. On the basis of the results of the univariate analysis, the variables that were significantly associated with occupational gaps (p < 0.05) were then selected as independent variables.
Thereafter, two multiple regression analyses were performed using a backward removal regression analysis. One analysis was performed to ascertain factors that were associated with the extent of occupational gaps one year post-stroke. For the 12-month model, the independent variables, based on the results of the univariate analysis, were baseline factors and factors at 12 months. The other analysis was performed to ascertain factors that could predict at 3 months the extent of occupational gaps one year post-stroke. For the 3-month model, the independent variables, based on the results of the univariate analysis, were baseline factors and factors at 3 months. Correlational analyses were performed between the independent variables to check for multicollinearity. One significant relationship concerning both models was found and that was between the variables born in Sweden and MMSE (p = 0.00). In the 3-month model, two significant relationships were found; born in Sweden and SIS participation (at 3 months) (p = –0.03) and born in Sweden and SIS recovery (at 3 months) (p = 0.00). In the 12-month model, 3 significant relationships were found; born in Sweden and SIS participation (at 12 months) (p = –0.02), born in Sweden and SIS recovery (at 12 months) (p = –0.04) and born in Sweden and global life satisfaction (p = –0.01). Normal distribution, linearity and equal variance were assessed according to Cohen et al. (29), and satisfied the assumptions.
Lastly, because of the findings in both the 3- and 12-month final models regarding those who were not born in Sweden, we analysed the findings for this group with descriptive statistics (means for interval or ratio level data, medians for ordinal level data, numbers, and percentages for nominal level data).
Statistical significance levels were set at p < 0.05. Confidence levels were set at 95%. All analyses were performed in Statistica (StatSoft Inc., version 8.0).
Results
The OGQ, the main outcome measure, was available for 200 persons and these persons constituted the participants in the present study. The descriptive characteristics of the participants and the responses on the SIS at 3 and 12 months are shown in Tables I and II, respectively. The mean age of the persons in this study was 69 (SD 14.3) years and 59% were men. The participants had both ischaemic and haemorrhagic strokes and represented a mixture of both first-ever and previous strokes. Thirty-five persons (18%) were not born in Sweden and 70% of the persons in the present study had a mild stroke. Eighteen of the study participants did not respond to all of the items on the OGQ, but only two of these persons had two unanswered items and the remainder, one unanswered item. Regarding global life satisfaction (n = 189), 23% were very satisfied, 26% were satisfied, 29% rather satisfied, 10% rather dissatisfied and 5% were dissatisfied or very dissatisfied.
| Table I. Characteristics of study participants at inclusion (n = 200) |
| Characteristics | At inclusion |
| Mean age, years (SD) | 69 (14.3) |
| Male/female, n (%) | 117 (58.5)/83 (41.5) |
| Born in Sweden, yes/no, n (%) | 165 (82.5)/35 (17.5) |
| Civil status, na (%) | |
| Married/co-habitating | 113 (56.5) |
| Single/living alone | 85 (42.5) |
| Working/studying, na (%) | 58 (29) |
| MMSE, meanb (SD) | 25.4 (4.2) |
| Barthel Index (BI), median (QR) | 85 (55) |
| Hemisphere lesion, n (%) Right | 88 (44) |
| Left | 80 (40) |
| Unspecifiedc | 32 (16) |
| Stroke severityd, n (%) | |
| Mild | 139 (69.5) |
| Moderate | 43 (21.5) |
| Severe | 18 (9) |
| a n = 198. bn = 161. ce.g. cerebral infarction-unspecified, deep inter-cerebral haemorrhage, haemorrhage with multiple localizations. dBI scores 51–100 = mild, 15–50 = moderate,< 14 = severe (28). SD: standard deviation; MMSE: Mini Mental State Examination; QR: quartile range. |
| Table II. Results of domains of the Stroke Impact Scale at 3 and 12 months post-stroke (n = 200) |
| SIS domains | Three months post-stroke Mean (range) | Twelve months post-stroke Mean (range) |
| SIS domain 3 emotions | 75.03 (16.6–100) | 78.27 (13.8–100) |
| SIS domain 5 ADL/IADL | 77.35 (0–100) | 78.39 (0–100) |
| SIS domain 8 participation | 69.62 (0–100) | 72.18 (0–100) |
| SIS physical functions | 74.27 (0–100) | 76 (0–100) |
| SIS recovery level scale | 62.74 (0–100) | 69.56 (0–100) |
| SIS: Stroke Impact Scale; ADL/IADL: activities of daily living/instrumental activities of daily living. |
Occupational gaps at one year post-stroke
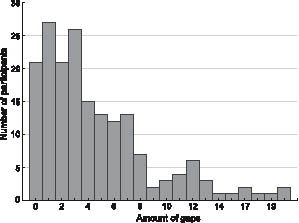
Table III depicts all of the activities in the OGQ and the number of gaps (raw scores) experienced by the participants. The mean number of occupational gaps experienced by 182 participants was 4.6 (median 3, range 0–22). The remaining 18 persons who did not respond to all of the items on the OGQ had a mean of 7.2 gaps (range 0–16). The greatest percentage of occupational gaps for the 200 participants was found in the activity travelling for pleasure, where 38% of the persons experienced a gap. Thirty-three percent of the persons experienced gaps in outdoor life. Four or more occupational gaps were experienced by 45% of the respondents. In order to better describe the extent of occupational gaps we depict them in frequencies (Fig. 1).
| Table III. Numbers of reported occupational gaps and the percentages of persons reporting specific occupational gaps (n = 200) |
| Activity | Occupational gaps n (%) |
| Instrumental ADL | |
| Grocery shopping | 40 (20) |
| Cooking | 43 (21) |
| Doing the laundry | 33 (16) |
| Cleaning | 58 (29) |
| Performing light maintenance | 41 (20) |
| Performing heavy duty maintenance | 48 (24) |
| Managing personal finances | 27 (13) |
| Transportation | 43 (21) |
| Leisure activities | |
| Sports | 58 (29) |
| Outdoor life | 67 (33) |
| Hobbies | 52 (26) |
| Cultural activities | 59 (29) |
| TV/video/radio | 2 (1) |
| Reading newspaper | 13 (6) |
| Reading books or periodicals | 34 (17) |
| Writing | 45 (22) |
| Playing the lottery, etc. | 27 (13) |
| Playing computer games | 29 (14) |
| Social activities | |
| Visiting partner/children | 9 (4) |
| Visiting relatives/friends | 19 (9) |
| Engaging in societies, clubs or unions | 27 (13) |
| Participating in religious activities | 13 (6) |
| Visiting restaurants and bars | 32 (16) |
| Travelling for pleasure | 76 (38) |
| Work or work-related activities | |
| Working | 25 (12) |
| Studying | 27 (13) |
| Taking care of and raising children | 6 (3) |
| Performing voluntary work | 12 (6) |
| ADL: activities of daily living. |
Fig. 1. Distribution of the numbers of perceived occupational gaps.
Factors associated with occupational gaps
The results of the univariate regression analysis are presented in Table IV.
| Table IV. Univariate analyses of the associations between occupational gaps at 12 months (in logits) and demographic, medical, 3 and 12 month factors (n = 200) |
| Independent variable | B | 95% CI | p-value | R2 (adjusted) |
| Lower | Upper |
| Inclusion | | | | | |
| Age | 0.01 | –0.002 | 0.025 | 0.114 | 0.01 |
| Gender | 0.14 | –0.271 | 0.554 | 0.500 | –0.00 |
| Born/not born in Sweden | 0.81 | 0.287 | 1.335 | 0.002 | 0.04 |
| MMSE (≤ 23/ ≥ 24) | 0.74 | 0.238 | 1.240 | 0.004 | 0.04 |
| Stroke severity | 0.94 | 0.653 | 1.225 | 0.000 | 0.17 |
| 3 months | | | | | |
| SIS emotions | –0.03 | –0.044 | –0.021 | 0.000 | 0.15 |
| SIS ADL/I-ADL | –0.03 | –0.039 | –0.024 | 0.000 | 0.27 |
| SIS participation | –0.03 | –0.038 | –0.025 | 0.000 | 0.30 |
| SIS physical functions | –0.03 | –0.038 | –0.038 | 0.000 | 0.26 |
| SIS recovery | –0.03 | –0.032 | –0.018 | 0.000 | 0.19 |
| 12 months | | | | | |
| SIS emotions | –0.04 | –0.050 | –0.029 | 0.000 | 0.23 |
| SIS ADL/I-ADL | –0.03 | –0.039 | –0.026 | 0.000 | 0.32 |
| SIS participation | –0.03 | –0.038 | –0.025 | 0.000 | 0.32 |
| SIS physical functions | –0.05 | –0.056 | –0.036 | 0.000 | 0.29 |
| SIS recovery | –0.03 | –0.039 | –0.025 | 0.000 | 0.29 |
| Global life satisfaction | –0.56 | –0.709 | –0.412 | 0.000 | 0.22 |
| MMSE: Mini Mental State Examination; SIS: Stroke Impact Scale; ADL/I-ADL: activities of daily living/instrumental activities of daily living; CI: confidence interval. |
The independent variables that were ascertained through univariate regression analysis and used in the 12-month model and analysed for association with the extent of occupational gaps at 12 months were: SIS domains for emotions, ADL/IADLs, participation, physical function, and self-rated recovery as well as the global LiSat-11 responses, all measured at 12 months post-stroke, and stroke severity, born in Sweden or not and the results of the MMSE score 24 or more or 23 or less at stroke onset. The independent variables that were ascertained through univariate regression analysis and used in the 3-month model as plausible predictors of the extent of occupational gaps were: SIS domains for emotions, ADL/IADLs, participation, physical function, and self-rated recovery all measured at 3 months post-stroke as well as stroke severity, born in Sweden or not and the MMSE score 24 or more or 23 or less at stroke onset.
The final models (Tables V and VI) showed that, at 12 months, social participation (domain 8 of the SIS), if the person was born in Sweden or not, stroke severity, global life satisfaction and self-perceived recovery were associated with the extent of occupational gaps. At 3 months, social participation (SIS domain 8), if the person was born in Sweden or not and perceived ADL ability (SIS domain 5) predicted the extent of occupational gaps at one year after stroke. In the 12-month model 37% of the variance (R2 adjusted) was explained by the 5 variables, while 27% of the variance (R2 adjusted) was explained by the 3 variables in the 3-month model.
| Table V. Multiple regression analysis; factors associated with occupational gaps (in logits) at 12 months (n = 189) |
| Variable | B | Beta | SE | 95% CI | p-value |
| Lower | Upper |
| SIS participation (12 months) | –0.02 | –0.28 | 0.00 | –0.025 | –0.006 | 0.001 |
| Born/not born in Sweden | 0.80 | 0.22 | 0.24 | 0.319 | 1.270 | 0.001 |
| SIS recovery (12 months) | –0.01 | –0.17 | 0.00 | –0.020 | –0.000 | 0.033 |
| Global life satisfaction | –0.20 | –0.18 | 0.09 | –0.383 | –0.021 | 0.028 |
| Stroke severity | 0.43 | –0.15 | 0.20 | 0.031 | 0.832 | 0.035 |
| Adjusted R2 = 0.37. SIS: Stroke Impact Scale; CI: confidence interval. |
| Table VI. Multiple regression analysis; predictors at 3 months of occupational gaps (in logits) at 12 months (n = 200) |
| Variable | B | Beta | SE | 95% CI | p-value |
| Lower | Upper |
| SIS participation (3 months) | –0.02 | –0.31 | 0.01 | –0.029 | –0.009 | 0.000 |
| SIS ADL/I-ADL (3 months) | –0.02 | –0.24 | 0.01 | –0.028 | –0.004 | 0.006 |
| Born/not born in Sweden | 0.75 | 0.20 | 0.27 | 0.206 | 1.288 | 0.007 |
| Adjusted R2 = 0.27. SIS: Stroke Impact Scale; ADL/IADL: activities of daily living/instrumental activities of daily living; CI: confidence interval. |
Analysis of persons not born in Sweden
The mean number of gaps was 6.9 (median 5) for the persons not born in Sweden, compared with those born in Sweden, who had a mean of 4.2 (median 3) occupational gaps per person. This significant difference (p = 0.001) indicates that the persons who were not born in Sweden reported a greater extent of occupational gaps compared with native Swedes. Persons not born in Sweden experienced the greatest number of gaps in traveling for pleasure (46% for non-natives, cf. 36% for natives) and outdoor life 43% for non-natives, cf. 31% for natives). These were followed by gaps in cleaning, cultural activities, and sports (43%, cf. 25%, 37% cf. 28%, 34% cf. 28% for non-natives and natives, respectively). Of the 21 (60%) men and 14 (40%) women comprising the 35 participants that were not born in Sweden, their mean and median age was 67 (range 34–89) years. There were no differences regarding gender between the two groups; however, there was a greater percentage with a severe stroke (14%) (cf. 7% of those born in Sweden) and, consequently, a lower percentage (60%) with mild stroke.
Discussion
The results of this study showed that the mean number of occupational gaps presented in raw scores was 4.6 per person one year post-stroke. Five factors were associated with occupational gaps at 12 months: social participation, not born in Sweden, recovery, life satisfaction, and stroke severity. The 3 factors: social participation and ADL ability at 3 months as well as not being born in Sweden predicted the extent of occupational gaps at one year and explained 27% of the variance.
Extent of occupational gaps
Approximately half of the respondents perceived 4 or more gaps one year after their stroke and approximately one-tenth did not have any gaps. This can be compared with a previous study of persons 1–4 years after ABI (16), where approximately 10% had 4 or more gaps and approximately 33% did not have any occupational gaps. The highest proportion of gaps found in the previous study was reported for work (34%), probably due to the younger sample (median age 50 years). The highest proportion of gaps found in the present study was in the activity travelling for pleasure (38%), followed by outdoor life (33%). These activities require a certain level of executive and motor functions, and stroke severity was found to be significantly associated with occupational gaps. A significant association between occupational gaps and perceived impairment was also found by Eriksson et al. (16). Another plausible explanation might be fatigue, which is common after a stroke (30). However, the present study did not measure this.
Factors associated with occupational gaps
The participation domain in the SIS was a factor that was associated with the extent of occupational gaps (in logits) in both the 3- and 12-month models. This was in accordance with our expectations, since both SIS participation and OGQ are considered to be measures of participation, albeit different types of participation. The OGQ is considered to measure participation in everyday occupations and the SIS participation domain is considered to be a measure of social functioning (31). However, the greatest difference in these two measures is not the activities covered, but the underlying construct reflected in the general questions. The SIS asks about the individuals’ feelings of limitations for each activity (i.e. none of the time/all of the time). In contrast, the OGQ asks if the individual does, and wants to do, the activity, measuring the discrepancy of the responses and suggesting that the individual connects a certain desire to perform the activity. The notions of meaning, value and choice are considered to be pre-requisites for effective participation (32, 33) and are considered important to measure (34). Since the OGQ measures participation in everyday occupations and does not appear to measure the same type of participation as the SIS, the OGQ can be used as a complement to other participation measures, adding a different dimension to participation.
Another factor associated with the extent of occupational gaps was the subjective rating of recovery one year after stroke. Subjective evaluation by a person of his or her own health status has shown to have high predictive value for outcome (34), which is in line with the results of the present study that show individuals’ perception of a low level of recovery to be associated with restrictions in participation.
Forty-nine percent of the persons in the present study rated their global life satisfaction as satisfied or very satisfied, which is in agreement with a Swedish study using the same measure (LiSat-11) (35). Due to the results of a previous study showing a relationship between the perception of occupational gaps and life satisfaction (15), we hypothesized that life satisfaction would have an association with participation in everyday occupations one year post-stroke and this was confirmed in the 12-month model.
The individuals’ perception of ADL/I-ADL ability rated at 3 months post-stroke was found to be a predictor of occupational gaps at one year. Since ADL interventions are common within rehabilitation and ADL outcomes are modifiable, this finding warrants special attention for possible implications in rehabilitation programmes. The findings also support the recommendations of ADL training in a sub-acute phase of rehabilitation, found in the National Swedish Guidelines (36).
Being born outside of Sweden was also found, at both 3 and 12 months, to be associated with occupational gaps one year post-stroke. Even though these results were not expected, the results were not surprising taking into account the literature analysing migrants or non-natives. Huot & Rudman (37) analysed the changes in occupations in everyday life that migrants face and challenges to their personal and social identity. The greatest percentage of occupational gaps experienced by those not born in Sweden were in the same activities as native Swedes, i.e. travelling for pleasure and outdoor activities. These activities were followed by gaps in cultural activities, sports and cleaning. However, the differences were greater percentage-wise in the non-native group and, most noteworthy, the greatest difference was found in cleaning. This is an interesting finding, which could be explored further in future studies.
In addition, a recent study showed that migrants living in Sweden experience poorer health compared with natives. This is considered to be related to a number of different factors, such as lower socioeconomic standing, poor integration and discrimination (38). The fact that the variable being born outside of Sweden was found to be associated with occupational gaps needs further analysis because of different considerations. First, in the present study, the group of those not born in Sweden had a larger percentage of severe strokes and, secondly, the group was younger compared with native Swedish persons with stroke. Both of these factors may have had an effect on the outcome.
Three factors at 3 months predicted occupational gaps one year post-stroke and explained 27% of the variance. Even though these findings contribute to our knowledge concerning factors predicting a risk for participation restrictions in everyday occupation one year post-stroke, further research is needed in order to develop rehabilitation interventions to prevent participation restrictions.
Methodological considerations
Empirical studies guided our choices of the independent variables used to predict occupational gaps, and we aspired to consider those factors that theoretically could affect the outcome. Multicollinearity was detected, which could have possibly limited our choices of certain independent variables, but was not remediated. According to Cohen et al. (29), multicollinearity has little effect on the regression analysis if the sole interest of the analysis is the prediction of the outcome variable, or in the value of R2, as in the present study.
There were, however, certain limitations in our choices of independent variables, for example regarding depression. Depression, per se, was not measured in the present study. Even though high rates of depression associated with low levels of life satisfaction have been found in a previous study of persons with stroke (39), depressive mood was found to have a weak association with the extent of occupational gaps for persons with acquired brain injury (15). The emotions domain in the SIS, albeit not a depression measure, reflects the general mood state of the individual. However, the emotions domain was not associated with the extent of occupational gaps either at 12 months or as a 3-month predictor.
The generalizations of the findings, despite that this was a hospital-based population study, should be understood with caution. Those with minor stroke symptoms may not have been admitted to the stroke unit and those with massive strokes, admitted to intensive care, are likely to be under-represented in the main population of 349 persons. Also, the aim was to administer all of the assessments to the 349 persons included in the main study population. However, those persons who did not have the endurance, or otherwise did not respond to the OGQ, the main outcome assessment, were not included in the present study, which may limit the generalization of the findings.
Clinical implications
The knowledge generated from this study adds to the emerging literature on participation in everyday occupations and contributes information on factors that predict persons at risk for occupational gaps. Measuring participation in everyday occupations is a supplement to already existing participation measures and is needed in order to provide a broader description of individuals’ health and well-being and to illuminate individuals’ needs for rehabilitation interventions.
Rehabilitation interventions should aim at reducing the extent of occupational gaps (16). Approximately half of the participants in the present study experienced occupational gaps one year post-stroke, indicating restrictions in their participation. Thus, long-term rehabilitation interventions with the aim of reducing the number of occupational gaps are indicated for persons who perceive participation restrictions.
This study sought to explore factors that would predict, in the sub-acute stage, persons at risk for occupational gaps. It is imperative that rehabilitation professionals can identify these persons and implement relevant and effective interventions in order to minimize this risk. Participants with self-perceived lower levels of ADL ability, measured at 3 months post-stroke, were found to risk restrictions in participation at one year. This may indicate the need for ADL evaluations at this time-point and the determination of any further ADL interventions required. Moreover, if persons with stroke are not born in Sweden, more extensive rehabilitation interventions may be indicated. More knowledge is needed regarding occupational gaps in different samples of persons with stroke, such as those who are not native to the country, in order to develop effective client-centred intervention strategies with the goal of reducing the extent of occupational gaps.
Acknowledgements
Financial support was provided by the Health Care Sciences Postgraduate School at Karolinska Institutet, the Swedish Brain Foundation (Hjärnfonden), Stroke-Riksförbundet, The Swedish Research Council, and The Swedish Council for Working Life and Social Welfare, the regional agreement on medical training and clinical research (ALF) between Stockholm County Council and Karolinska Institutet.
The authors would like to thank Anders Kottorp, Karolinska Institutet, for support regarding Rasch analysis.
References