OBJECTIVE: To investigate the validity and reliability of the Tampa Scale for Kinesiophobia Heart (TSK-SV Heart), a brief questionnaire to detect kinesiophobia (fear of movement) in patients with coronary artery disease.
DESIGN: Methodological research (cross-sectional study).
SUBJECTS: A total of 332 patients, mean age 65 years (standard deviation 9.1) diagnosed with coronary artery disease at a university hospital were included in the study.
METHODS: The psychometric properties of the TSK-SV Heart were tested. The tests of validity comprised face, content, and construct validity. The reliability tests included composite reliability, internal consistency and stability over time.
RESULTS: In terms of reliability, the TSK-SV Heart was found to be stable over time (intra-class correlation coefficient 0.83) and internally consistent (Cronbach’s alpha 0.78). Confirmatory factor analysis provided acceptable fit for a hypothesized 4-factor model with inclusion of a method factor.
CONCLUSION: These results provide support for the reliability of the TSK-SV Heart. The questionnaire appears to be valid for use in patients with coronary artery disease. However, some items require further investigation due to low influence on some sub-dimensions of the test. The sub-dimensions of kinesiophobia require future research concerning their implications for the target group.
Key words: coronary artery disease; cardiac rehabilitation; Tampa Scale for Kinesiophobia; fear of movement; kinesiophobia; psychometrics; confirmatory factor analysis.
J Rehabil Med 2012; 00: 00–00
Correspondence address: Maria Bäck, Department of Physiotherapy, Vita stråket 13, Sahlgrenska University Hospital, Sahlgrenska, SE-413 45 Göteborg, Sweden. E-mail: maria.m.back@vgregion.se
Submitted May 11, 2011; accepted November 14, 2011
Introduction
Exercise-based cardiac rehabilitation decreases morbidity and mortality in patients with coronary artery disease (CAD) and has further favourable effects on the risk factors for atherosclerotic disease (1, 2). Despite strong evidence for the benefits of exercise-based cardiac rehabilitation, studies show poor attendance and adherence (3). There is a need to identify obstacles that prevent patients from participating in cardiac rehabilitation and increasing their levels of physical activity, including exercise.
Based on clinical experience, patients with CAD often have doubts that physical activity can be performed safely due to the disease, and consequently they may avoid physical activity and exercise. Avoidance behaviour is adaptive as a natural response to acute injury (4). However, for patients with chronic pain, it has been demonstrated that if an injury is interpreted as threatening it leads to the more specific fear that physical activity will cause (re)injury (also called fear of movement). This fear can subsequently cause long-term avoidance behaviour with respect to physical activity, leading to negative physical and psychological consequences (5). These avoidance concepts have, however, not been fully investigated in patients with CAD, in whom a similar process may operate.
Kinesiophobia was originally defined as “an excessive, irrational, and debilitating fear of movement and activity, resulting from a feeling of vulnerability to painful injury or re-injury” (6). Kinesiophobia has been shown to have a negative influence on the outcome of rehabilitation (7, 8), but its relationship to the outcome of cardiac rehabilitation in patients with CAD is not known. It has, however, been shown that fear of exercise correlates with poor quality of life for patients with an implantable internal cardiac defibrillator (9).
Only one questionnaire has been specifically designed to measure kinesiophobia, the Tampa Scale for Kinesiophobia (TSK) (10). The TSK was designed to measure kinesiophobia in patients with persistent musculoskeletal pain and has been found to be valuable in both research and clinical settings (11). The TSK has been translated into Swedish (TSK-SV) and has been found to be reliable and valid for patients with chronic back pain (12). The present study reports on an adaption of the TSK-SV for patients with CAD, TSK-SV Heart, and a subsequent evaluation of the validity and reliability of the questionnaire. Confirmatory factor analysis was used to investigate the factor structure of the TSK-SV Heart. A 4-factor model was hypothesized, including the following constructs: “Perceived danger for heart problem”, “Avoidance of exercise”, “Fear of injury” and “Dysfunctional self”, based on the original framework by Kori et al. (6) and on the Diagnostic and Statistical Manual of Mental Disorders (DSM) (13). The DSM describes a framework for typical mental imaginations and beliefs that occur with phobia of an object: the subject’s perceptions of the object, the subject’s avoidance of the object, and the consequences for the subject of having a phobic relationship to an object. From a secondary prevention point of view, it is desirable to have a self-reporting measure to identify high levels of kinesiophobia in patients with CAD. Early recognition may facilitate appropriate treatment for these patients.
The aims of the study were to investigate: (i) face validity, content validity, and construct validity of the TSK-SV Heart; and (ii) composite reliability, internal consistency, and stability over time.
Methods
Patients
In total, 332 patients (75 women; mean age 65 years (standard deviation (SD) 9.1) were recruited between 2007 and 2009 at Sahlgrenska University Hospital/Sahlgrenska, Gothenburg, Sweden. The patients were included a median of 6 months (range 3–10) after hospital discharge. A study nurse contacted and informed the patients about the study via a telephone call. If the patient was interested in participating in the study, a visit to the physiotherapy department was arranged within the next few days. Informed written consent was obtained from all patients before the TSK-SV Heart was completed. The inclusion criterion was a principal diagnosis of CAD. Exclusion criteria were: death during the hospital period, serious diseases interfering with participation in the study, inability to understand Swedish, and a time period of more than 10 months after hospital discharge. From a total of 1,112 patients who fulfilled the inclusion criteria, 332 took part in the study. The main reasons for exclusion were: delayed evaluation >10 months after hospital discharge due to lack of organizational capacity, i.e. logistic problems (n = 553), no contact by telephone (n = 157), and unwillingness to participate (n = 65). The baseline characteristics of the patients are shown in Table I. The regional ethics review board in Gothenburg approved the research protocol.
| Table I. Descriptive characteristics of the study population (n = 332) |
| Characteristics | |
| Age, years, mean (SD) (min–max) | 65 (9.1) (26–85) |
| Women, n (%) | 75 (22.6) |
| Height, cm, mean (SD) | 174 (9) |
| Weight, kg, mean (SD) | 82 (14) |
| Previous history, n (%) | |
| Myocardial infarction | 99 (29.8) |
| Angina pectoris | 161 (48.5) |
| PCI | 83 (25) |
| CABG | 35 (10.5) |
| Heart failure | 21 (6.3) |
| Diabetes | 57 (17.2) |
| Hypertension | 157 (47.3) |
| Stroke | 28 (8.4) |
| Peripheral artery disease | 21 (6.3) |
| Atrial fibrillation | 33 (9.9) |
| Malignant disease | 24 (7.2) |
| Other severe disease | 56 (16.9) |
| Current smoking, n (%) | 63 (19) |
| Type of CAD, n (%) | |
| STEMI | 100 (30.1) |
| Non-STEMI | 52 (15.7) |
| Unstable angina | 123 (37) |
| Stable angina | 57 (17.2) |
| Complications/interventions in hospital, n (%) | |
| PCI | 215 (64.8) |
| CABG | 63 (19) |
| Heart failure | 33 (9.9) |
| Cardiac rehabilitation, n (%) | 189 (56.9) |
| Shoulder flexion, n, mean (SD) | 40 (21.5) |
| Shoulder abduction, s, mean (SD) | 104 (42.3) |
| IPAQ Category 1/2/3, n | 58/175/77 |
| Steps/day, pedometer, mean (SD) | 7,278 (3,764.7) |
| Physical component summery (SF-36), mean (SD) | 45.3 (10.2) |
| Mental component summery (SF-36), mean (SD) | 47.3 (11.1) |
| Anxiety (HADS), mean (SD) | 4.3 (3.8) |
| Depression (HADS), mean (SD) | 3.4 (3.2) |
| SD: standard deviation; PCI: percutaneous coronary intervention; CABG: coronary artery bypass grafting; CAD: coronary artery disease; STEMI: ST elevation myocardial infarction; IPAQ: International Physical Activity Questionnaire; SF-36: Short-Form 36; HADS: Hospital Anxiety and Depression Scale, internal missing: Shoulder flexion n = 8, shoulder abduction n = 30, IPAQ n = 21, steps/day n = 19. |
Methods
Kinesiophobia. The TSK-SV Heart comprises 17 statements that assess the subjective rating of kinesiophobia. The statements are rated from “strongly disagree” (score =1) to “strongly agree” (score =4) on a 4-point Likert scale. Four items (4, 8, 12, 16) are phrased in reversed key. The total score varies between 17 and 68. The higher the value, the greater the degree of kinesiophobia (11).
Muscle endurance. Muscle endurance was evaluated using two tests; unilateral isotonic shoulder flexion, and bilateral isometric shoulder abduction. The tests are described in detail elsewhere (14).
Physical activity. Physical activity was measured over a 7-day period. The categorical form of the International Physical Activity Questionnaire (IPAQ) was administered, identifying 3 levels of physical activity (1 = low, 2 = medium, 3 = high) (15). Furthermore, the patients were asked to wear a pedometer on their hip (Keep Walking LS 2000, KeepWalking Scandinavia AB, Kalmar, Sweden) for the same 7 consecutive days. The results were converted to mean steps per day (total steps during a week/7).
Health-related quality of life. The Short-Form 36 (SF-36) is a generic questionnaire measuring health-related quality of life across 8 dimensions, divided into 2 components. The physical component comprises physical functioning, role physical limitations, bodily pain, and general health perceptions. The mental component comprises vitality, social functioning, role emotional limitations, and mental health (16).
Anxiety and depression. The Hospital Anxiety and Depression Scale (HADS) comprises 7 anxiety and 7 depression items, from which separate anxiety and depression scores are calculated (17).
Procedure
The TSK-SV Heart (see Appendix I) was tested according to the following procedure. The items from the original version of TSK-SV were adapted to patients with CAD, and subsequent analyses of validity and reliability were performed. The TSK-SV Heart was translated into English by a professional translator.
Validity
Face and content validity. A pre-test in patients with CAD (n = 10) was performed to provide feedback on the items and to check the time required to complete the questionnaire. Furthermore, the patients gave their opinion on the face validity. Five experts (physiotherapists with experience from working with patients with CAD) were also asked to assess the face validity of the TSK-SV Heart. In addition, the experts were requested to form an opinion of the content validity through a pre-printed form.
Construct validity. Construct validity was investigated in two phases. Firstly, the TSK-SV Heart was conceived as a theoretical concept with 4 sub-dimensions. A model for this concept was based on a second-order confirmatory factor analysis (CFA). In addition, the proposed 4-factor model was compared with an often-used 2-factor model (18) based on 11 items (19). Secondly, 4 composite constructs were created and used separately as dependent variables in multiple regression on 9 sets of independent variables. These sets were comprised of demographics (gender, age), medical focus (cardiac rehabilitation, heart failure, muscle endurance), physical activities, health-related quality of life, anxiety, and depression.
Second-order CFA model. The choice of the model is based on a hierarchy of constructs of kinesiophobia. The 4 constructs “Perceived danger for heart problem” (Danger), “Avoidance of exercise” (Avoidance), “Fear of injury” (Fear), and “Dysfunctional self” (Dysfunction) were first-order latent (reflexive) indicators to the construct of kinesiophobia, and they were at the same time superior constructs of the 17 items of the TSK-SV Heart. Moreover, the first-order latent variables were assumed to be uncorrelated in the model, as were the residuals of the items within each construct. The following items were included in each of the constructs: Danger (3, 8, 11, 16), Fear (1, 7, 9, 13), Avoidance (2, 4, 12, 14, 17), and Dysfunction (5, 6, 10, 15). The factor loadings for the first-order constructs were controlled for Type 1 error by use of a Bonferroni correction at the 5% significance level (20).
Model fit. A χ2 test with maximum likelihood parameter estimation robust to non-normality was used (MLMV estimator mean- and variance-adjusted maximum likelihood). Moreover, approximate fit indices were reported to supplement a failed χ2 test. These were comparative fit index (CFI), and root mean square error of approximation (RMSEA). For good fit between the hypothesized model and the observed data, cut-off values often suggested are close to 0.95, and 0.06, for CFI and RMSEA, respectively (21). In addition, factor determinacy, reflecting the correlation between the estimated and true factor score, was reported.
Data preparation for CFA. Concerning missing data, the choice of MLMV estimation of the CFA model was combined with expectation maximization algorithm (Little’s missing completely random (MCAR) test), included in the SPSS package. In order to enhance external validity, a model-based selection of influential cases was performed (22). Each case was tested with respect to its contribution to model fit. If the removal of a case improved the model χ2 fit by at least 3.8, it was classified as an influential case.
Reliability
Composite reliability was analysed according to a procedure, described by Raykov & Shrout (23), for a scale with different subsets of items. The scale was assumed to be non-congeneric (non-homogenous scale). Based on the general definition of reliability, composite reliability was computed as a ratio of true composite variance (latent variables) to observed composite (items) variance of scores.
To measure internal consistency, Cronbach’s alpha statistics were calculated for the 17 items (24) and the item-total correlation coefficient was assessed. A coefficient > 0.40 is desirable (25). A test-retest procedure, including a Bland-Altman plot (26), was used for measuring stability over time. The first 88 patients were requested to complete another TSK-SV Heart at home after 2 weeks and to return it by post in a pre-paid envelope. In total, 79 questionnaires were used for the test–retest analyses. Six of the questionnaires had some missing data, and consequently, the total score for each subject was computed as a mean across the 17 items.
Statistical analyses
Descriptive statistics were used for the demographic data, which are presented as means and one standard deviation. The intra-class correlation coefficient (ICC), two-way mixed model was used for statistical analysis of the test-retest method (27). The computation of composite reliability and the CFA model was carried out with Mplus, version 6, (Muthén & Muthén, Los Angeles, CA, USA). All other data were analysed using the Statistical Package for the Social Sciences (SPSS 20.0, Chicago, IL, USA).
Results
Validity
Face and content validity. The patients with CAD and the panel of experts considered the TSK-SV Heart to have face validity. Some of the patients, however, found it difficult to understand the reversed items. On the whole, the experts agreed that the TSK-SV Heart appeared to have content validity. They found all items essential for the measurement of kinesiophobia and reported no missing aspects. However, one expert considered items 1 and 9 to be too similar and another expert believed items 3 and 11 to be equivalent. The formulation of items 10 and 14 were modified after comments from the experts, to make the items clearer and more understandable.
Construct validity related to factorial structure. The corrected item-total correlations for the reversed items (4, 8, 12, 16) were low. A response bias factor was included in the CFA model with the reversed items as indicators. The response bias factor was not included as an indicator to kinesiophobia, and was orthogonal to all the other factors (first- and second-order). Five cases had missing values and, in all, 13 values were missing. They were successfully imputed (Little’s MCAR test: χ2 (72, n = 332) = 56.50, p = 0.910). Five other cases suppressed the model χ2 by more than 3.8 and were excluded. The influential cases were excluded.
Model fit. The exclusion of the 5 influential cases improved the model fit for the second-order CFA model. The first-order latent residuals were constrained to be equal, since they were rather small and had similar values. The model fit was not significantly impaired by this constraint. The factor with the reversed items largely improved the model fit. Moreover, one ad-hoc modification was performed based on calculation of modification indices. The correlation (0.26) between the residuals of items 4 and 17 was set free. Since these items both concern benefit of physical activity, the modification seemed reasonable. The final model had an acceptable fit: χ2 (113, n = 327) = 145.98, p = 0.020; ratio χ2 degrees of freedom (df) = 1.29; CFI = 0.95, RMSEA = 0.030 (90% CI: 0.013–0.043).
The factor loadings of the second-order model are shown in Table II. Some results should be noted. First, all factor loadings for the 4 theoretical constructs, with the exception of 3 of the 4 reversed items, were significant when tested against a critical value (Z = 3.351) based on the Bonferroni correction for the 5% p-level (0.05/62). Secondly, the factor determinacy for the construct of kinesiophobia was 0.92, and the same measure for the 4 indicators ranged between 0.89 and 0.92, and the squared multiple correlation coefficient (R2) ranged evenly between 0.87 and 0.95.
Two additional tests of factorial structure for test of construct validity were performed by use of the items of the TSK11. As in the previous tests, second-order CFA models were used, and the residual variances of the first-order latent factors were constrained to equality.
The first model was built on the TSK11-items and on the following 4 factors: Danger (items 8, 16 excluded), Fear (item 9 excluded), Avoidance (items 4, 12, and 14 excluded), and Dysfunction. This model had a good fit: χ2 (43, n = 327) = 58.84, p = 0.054; ratio χ2/df = 1.37; CFI = 0.97, RMSEA = 0.034 (90% CI: 0.0–0.053). The first- and second-order factor loadings were similar to those of the full model in Table II.
The second model used the TSK11-items with the following two original factors: Somatic focus (items 3, 5, 6, 7, 11 included), and Activity avoidance (items 1, 2, 10, 13, 15, 17 included). This model also had a good fit: χ2 (43, n = 327) = 57.77, p = 0.066; ratio χ2/df = 1.34; CFI = 0.97, RMSEA = 0.032 (90% CI: 0.0–0.052). Again, the first- and second-order factor loadings were similar to those of the full model in Table II.
| Table II. Standardized factor loadings (FL) for second- and first-order latent variables (n=332) |
| | FL | SE | FL/SE | Two-tailed p-value |
| Second-order |
| Kinesiophobia |
| Danger | 0.960 | 0.019 | 50.330 | < 0.001 |
| Fear | 0.935 | 0.031 | 29.983 | < 0.001 |
| Avoidance | 0.953 | 0.021 | 45.229 | < 0.001 |
| Dysfunction | 0.973 | 0.014 | 69.056 | < 0.001 |
| First-order |
| Perceived danger for heart problem (Danger) |
| Item 3 | 0.631 | 0.045 | 13.942 | < 0.001 |
| Item 11 | 0.565 | 0.051 | 10.985 | < 0.001 |
| Item 8 | 0.110 | 0.061 | 1.812 | 0.070 |
| Item 16 | 0.087 | 0.063 | 1.371 | 0.170 |
| Fear of injury (Fear) |
| Item 9 | 0.556 | 0.055 | 10.063 | < 0.001 |
| Item 1 | 0.499 | 0.054 | 9.258 | < 0.001 |
| Item 7 | 0.319 | 0.065 | 4.927 | < 0.001 |
| Item 13 | 0.315 | 0.058 | 5.389 | < 0.001 |
| Avoidance of exercise (Avoidance) |
| Item 2 | 0.659 | 0.051 | 12.829 | < 0.001 |
| Item 14 | 0.692 | 0.045 | 15.407 | < 0.001 |
| Item 17 | 0.357 | 0.064 | 5.575 | < 0.001 |
| Item 4 | 0.090 | 0.061 | 1.480 | 0.139 |
| Item 12 | 0.295 | 0.069 | 4.287 | < 0.001 |
| Dysfunctional self (Dysfunction) |
| Item 5 | 0.308 | 0.060 | 5.126 | < 0.001 |
| Item 6 | 0.607 | 0.043 | 14.062 | < 0.001 |
| Item 10 | 0.677 | 0.042 | 16.046 | < 0.001 |
| Item 15 | 0.766 | 0.035 | 22.015 | < 0.001 |
| Method Factor (orthogonal to all factors) |
| Reversed wording of items |
| Item 4 | 0.532 | 0.095 | 5.625 | < 0.001 |
| Item 8 | 0.344 | 0.082 | 4.207 | < 0.001 |
| Item 12 | 0.565 | 0.102 | 5.513 | < 0.001 |
| Item 16 | 0.184 | 0.077 | 2.407 | 0.016 |
| SE: standard error. |
Construct validity related to external measures. The results in Table III with the 4 constructs of the TSK-SV Heart as dependent variables are concerned with changes in the explained variance. Descriptive statistics of the independent sets is found in Table I. Some specific patterns of the results will be described. The variable sets with a medical focus had only a significant influence on the behaviourally oriented constructs (Avoidance and Dysfunction), but not on the constructs conceived of as beliefs and mental imaginations (Danger and Fear). A similar pattern was found for physical activities (IPAQ), which decreased for Dysfunction. An opposite pattern, not concerning the behavioural constructs, was found for gender (perceived danger higher for men) and for smoking (decreased fear of injury). Finally, some specific features were noted. Avoidance was not influenced by anxiety or depression, unlike Fear and Dysfunction. The physical components of the SF-36 did not influence Fear, but each of the three other constructs was influenced by these components.
| Table III. Regression analyses showing the change in explained variance of a dependent construct when a separate independent variable set was removed from the model |
| Independent variable sets | Dependent variable |
| Perceived danger for heart problem (R2 = 0.237) | | Fear of injury (R2 = 0.197) | | Avoidance of exercise (R2 = 0.241) | | Dysfunctional self (R2 = 0.402) |
| R2 change | p | | R2 change | p | | R2 change | p | | R2 change | p |
| 1 Demographics (gender, age) | 0.031 (13.1%) | 0.002 | | 0.001 | 0.909 | | 0.010 | 0.141 | | 0.003 | 0.469 |
| 2 Smoking | 0.002 | 0.339 | | 0.013 (6.6%) | 0.024 | | 0.002 | 0.399 | | 0.003 | 0.222 |
| 3 Cardiac rehabilitation | 0.003 | 0.309 | | 0.002 | 0.422 | | 0.026 (10.8%) | 0.001 | | 0.004 | 0.135 |
| 4 Heart failure (previous, present) | 0.001 | 0.818 | | 0.011 | 0.123 | | 0.004 | 0.411 | | 0.019 (4.7%) | 0.008 |
| 5 Muscle endurance (shoulder flexion and abduction) | 0.011 | 0.140 | | 0.006 | 0.343 | | 0.014 (5.8%) | 0.064 | | 0.013 (3.2%) | 0.046 |
| 6 IPAQ (M vs H), Pedometer | 0.001 | 0.800 | | 0.007 | 0.293 | | 0.002 | 0.633 | | 0.010 (2.5%) | 0.095 |
| 7 SF-36: (PF, RP, BP, GH) | 0.055 (23.2%) | 0.000 | | 0.015 | 0.229 | | 0.020 (8.3%) | 0.085 | | 0.068 (16.9%) | 0.000 |
| 8 SF-36: (VT, SF, RE, MH) | 0.005 | 0.728 | | 0.020 | 0.102 | | 0.014 | 0.222 | | 0.010 | 0.250 |
| 9 HADS: Anxiety, Depression | 0.010 | 0.134 | | 0.033 (16.8%) | 0.002 | | 0.008 | 0.202 | | 0.018 (4.5%) | 0.011 |
| The percentage (change/total) of a significant (p < 0.010) change in R2 is noted within brackets. Figures in bold are significant at p < 0.05. IPAQ: International Physical Activity Questionnaire; M: medium level (or medium-level) of physical activity and high-level of Physical activity; H: high-level of physical activity; Pedometer: mean/steps day; SF-36: Short-Form 36; PF, physical functioning; RP: role physical limitations; BP: bodily pain; GH: general health perceptions; VT: vitality; SF: social functioning; RE: role emotional limitations; MH: mental health; HADS: Hospital Anxiety and Depression Scale. |
Reliability
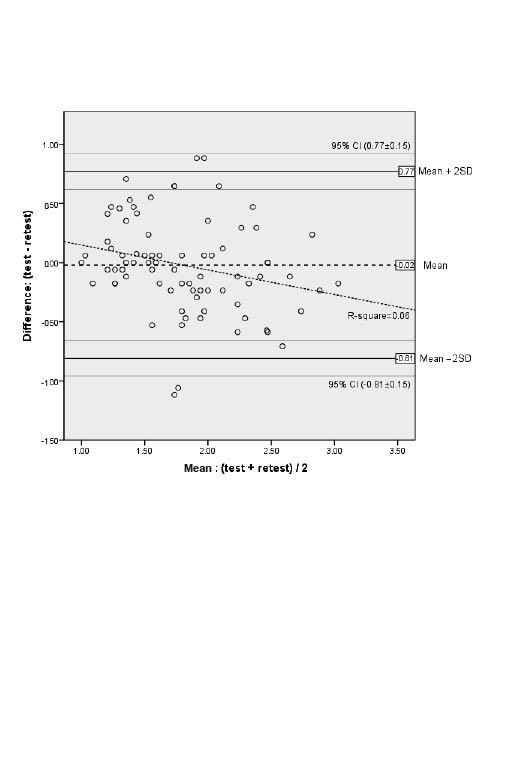
Composite reliability for the TSK-SV Heart was a ratio of the following estimates. If the method factor with reversed items was controlled for, the variance of the true scores was estimated as 50.178, and of the observed scores as 64.859. Composite reliability was computed as 0.77. If the reversed factor had been excluded, the composite reliability would be increased to 0.80, but with a clearly impaired model fit. Internal consistency assessed with Cronbach’s alpha was 0.78. The results for the corrected item-total correlation coefficients are presented, with greater values indicating better consistency with the total score: values between 0 and 0.20 (items 4, 8, and 16), values between 0.20 and 0.40 (items 5, 7, 12, 13, and 17). All other items had values > 0.40. The TSK-SV Heart was stable over time, evaluated with a two-week test-retest of the total score (ICC 0.83, 95% CI 0.73–0.89). Moreover, a Bland-Altman plot showed that the mean difference between the test and retest scores was close to zero. Either skewness or kurtosis for test and retest was significant. These findings were confirmed in the Bland-Altman plot. There were no obvious patterns of heteroscedasticity or proportionality. Although the regression of difference on mean scores showed a non-zero slope, the explained variance was small (6.3%). Four observations (< 5% of 332) were positioned outside the limits of agreement (2*SD). However, two of these were found within a 95% CI of the upper limit of agreement. Further information is given in Fig. 1.
Fig. 1. Bland-Altman plot showing difference against mean of test-retest values (range 1–4; n = 79) with mean (long-dashed line) and limits of agreement (thick solid lines), including 95% confidence intervals (thin solid lines), and with a regression line (short-dashed line). SD: standard deviation.
Discussion
The results of this study support the reliability and validity of the TSK-SV Heart questionnaire for use in patients with CAD.
The TSK-SV Heart was found to be stable over time, and this result is consistent with the previously reported test-retest reliability of the TSK in patients with chronic pain (12, 28).
The composite reliability for a test with non-homogenous subsets was acceptable (> 0.70) (23), as well as the Bland-Altman plot. The Cronbach’s alpha for the overall scale is also in agreement with prior studies (5, 12, 28).
According to content validity, the experts found some items too similar, and these items were also included in the same construct in the CFA model. The inter-item correlation coefficient for these items, however, was > 0.4, which supported the usefulness of these items for gaining knowledge of kinesiophobia.
The factorial structure of the TSK-SV Heart in this study had an acceptable model fit, although the reversed items (items 4, 8, 12, and 16) did not contribute significantly. We do not expect that a response bias factor for the reversed items should be included in the CFA model; therefore it is important to determine why the reversed items did not function as intended in the present study. However, the content of these reversed items are relevant, and the experts did not find them difficult to interpret. We propose that these items should be examined further.
The two alternative tests of models with 11 items from the reduced version of TSK (19) did not dispute the construct validity of the proposed 4-factor model in this study. As expected, model fit was improved when some items with the lowest factor loadings were removed, but the 4-factor model performed similarly to the 2-factor model. These results suggest that whether the proposed 4-factor model is appropriate does not seem to be a question of model fit.
Construct validity with respect to external measures was also investigated in the present study. Regression analyses showed rather distinct features for each construct. In contrast to the constructs concerned with beliefs and mental imaginations (Danger and Fear), it was advantageous from a theoretical point of view that only the behavioural constructs (Avoidance and, especially, Dysfunction) were associated with medical states, and physical activity. For example, if irrational perceptions and beliefs are held about rehabilitation, it is most reasonable that these are not tied to real-state circumstances. Instead these constructs were characterized by bodily-oriented perceptions (Danger) and by anxiety and depression (Fear), respectively. Moreover, it was reasonable that Avoidance was not associated with anxiety, since this is the very function of avoidance. On the other hand, fear of injury was specifically characterized by anxiety and depression. We conclude that the construct validity of the 4-factor model presented in this study is acceptable.
In the light of this discussion, it is also worth noting the theoretical distinction between fear and anxiety. These terms are often used interchangeably, although fear, by definition, is usually an unpleasant feeling that arises as a normal response to realistic danger, while anxiety is a future-oriented state arising without any objective source of danger (29).
We believe that some important aspects have been neglected in previous studies of kinesiophobia where TSK has been used. The focus has often been reduced to fear-avoidance, which is essential but not sufficient for investigation of kinesiophobia in the sense Kori et al. (6) have conveyed. The 4 concepts we propose give better theoretical prerequisites for screening for the perceptions and consequences of kinesiophobia. Being a short screening test, the TSK may not safely screen for kinesiophobia, but if phobic imaginations are present, then high ratings are required on more factors than just fear-avoidance. In general, a group with phobic imaginations has high estimates in all 4 concepts. However, the screening must be followed by more detailed diagnostics.
The limitations of our study must be discussed in terms of generalization. The exclusion rate was quite high in the study, which means a potential risk for selection bias. However, the effective participation rate among the patients actually contacted (n = 397) was 83%. Furthermore, we decided not to include patients with significant co-morbidities, which may have resulted in a relatively healthy population of patients with CAD.
Our findings provide preliminary support for the TSK-SV Heart as an appropriate questionnaire for measuring kinesiophobia in patients with CAD. However, it would be of interest to investigate the predictive validity, as level of physical activity before and after intervention. In the future, it would be desirable to design optimal interventions for these patients, with the overall target of enhancing levels of physical activity and adherence to exercise-based cardiac rehabilitation.
In conclusion, we have provided introductory support for the TSK-SV Heart as a reliable instrument for use in patients with CAD, and have established its face, content and construct validity. Further research is needed in this area to deepen our understanding of kinesiophobia and its meaning for physical activity and exercise in patients with CAD.
Acknowledgements
The authors would like to thank Lillemor Stensdotter, John Gillström and Susanna Wittboldt from the Sahlgrenska University Hospital for their help with data collection.
This study was supported by grants from the Swedish Heart and Lung Association, Rehabilitation Research Foundation, Allied Health Professional within Cardiology, Renée Eander’s Foundation, the Memorial Foundation and government grants under the ALF agreement.
The authors declare no conflicts of interest.
References