Liesbeth Daenen, PT, MSc1,2,3, Jo Nijs, PhD, PT3,4, Bonny Raadsen, PT3, Nathalie Roussel, PhD, PT3,4,5, Patrick Cras, MD, PhD1,2 and Wim Dankaerts, PhD, PT6
From the 1Department of Neurology, Faculty of Medicine, University of Antwerp, 2Department of Neurology, Born-Bunge Institute and Antwerp University Hospital, Antwerp, 3Department of Human Physiology, Faculty of Physical Education and Physiotherapy, Vrije Universiteit Brussel, Vrije, 4Division of Musculoskeletal Physiotherapy, Department of Health Sciences, University College Antwerp, 5Faculty of Medicine, University of Antwerp, Antwerp and 6Department of Rehabilitation Sciences, Faculty of Kinesiology and Rehabilitation Sciences, KU Leuven, Leuven, Belgium
OBJECTIVE: To study the presence of cervical motor dysfunctions in acute whiplash-associated disorders, evaluate their course and assess their predictive value for long-term recovery.
DESIGN: Systematic literature review.
METHODS: PubMed and Web of Science databases were used to select studies of the presence of cervical motor dysfunctions within the acute stage (< 6 weeks) after whiplash trauma and/or their predictive value for the development of chronic whiplash-associated disorders.
RESULTS: The presence of cervical motor dysfunctions in the acute stage after whiplash trauma was investigated in 4 cohorts. The course of cervical motor dysfunctions in whiplash-associated disorders was examined in 4 cohorts, and the predictive value on outcome one year post-whiplash trauma was assessed in 3 cohorts. Reduced cervical mobility, disturbed kinaesthesia, and altered muscle activity were found in the acute stage, and these persisted over time in the moderate/severe group. The predictive value of examining the presence of cervical motor dysfunctions was doubtful. The course and predictive value of initial reduced cervical mobility was inconsistent.
CONCLUSION: Cervical motor dysfunctions are present soon after whiplash trauma persisting in those with moderate/severe symptoms. However, these dysfunctions have limited predictive value, and hence may not explain the complex clinical picture of whiplash-associated disorders. This systematic review highlights the need for differentiating between patients with acute whiplash-associated disorders taking into account the biopsychological framework.
Key words: cervical motor dysfunctions; acute whiplash; course; predictive value.
J Rehabil Med 2013; 45: 00–00
Correspondence address: Jo Nijs, Vrije Universiteit Brussel, Building L-Mfys, Pleinlaan 2, BE-1050 Brussels, Belgium. E-mail: jo.nijs@vub.ac.be
Submitted February 21, 2012; accepted September 17, 2012
INTRODUCTION
The term “whiplash” refers to an acceleration-deceleration mechanism and the associated energy transfer to the cervical region as result of trauma, often due to a car crash or fall. This sudden impact at the cervical spine may result in injuries to the bony structures, joints/ligaments, and/or stabilizing muscles, and to nerve injuries and entrapments, and the development of a wide range of clinical manifestations commonly termed whiplash-associated disorder (WAD) (1). Most patients with whiplash trauma recover within 3 months. However, up to 50% of patients with acute WAD develop chronic pain and/or disability (2–4).
Chronic WAD is characterized by general symptoms, such as persistent neck pain, headache, dizziness, fatigue, sleep difficulties and concentration disturbances. In order to establish the underlying mechanism of chronic WAD, the involvement of several factors, including cognitive and psychosocial factors, the central nervous system (CNS) and motor system, have been studied. In chronic WAD, there have been numerous investigations into cervical motor dysfunction (CxMD). There is substantial evidence for the presence of various CxMDs in this patient population (5–14). Those persons with persistent symptoms (longer than 3 months after initial injury) often display reduced neck mobility (10, 13), impaired cervico-cephalic kinaesthesia (6, 7, 10, 12, 14) and altered cervical muscle activation patterns (5, 8, 9, 11, 13).
In contrast, research evaluating the development of CxMDs in the early stage after whiplash trauma is scarce. Gaining better insight into this process and its predictive value may help in developing efficient intervention strategies for patients with WAD in the acute stage. This is especially important since there is often little spontaneous improvement beyond 3 months post-whiplash trauma (1). Insight into the early development of CxMD and its predictive value for long-term recovery may enhance identification of those patients who are at risk for persistent symptoms, and facilitate the development of appropriate intervention strategies.
Previous reviews have attempted to synthesize the literature with regard to risk factors for persistent pain and disability after whiplash trauma. High levels of initial pain and disability were found to be a strong predictor of ongoing problems at long-term follow-up (3, 15–18). Furthermore, there is evidence that pain catastrophizing, female gender, not using a seat belt at the time of collision, history of previous neck pain, neck pain and headache at baseline, decreased neck movement, cold hyperalgesia, lower self-efficacy, post-traumatic stress, self-efficacy and expectations of recovery may predict poor outcome after whiplash trauma (15, 16, 18, 19). However, inconsistency concerning the predictive capacity of these risk factors remains.
Until now the literature addressing CxMDs in patients with acute WAD has not been systematically reviewed. The first aim of this study was therefore systematically to review the presence of CxMDs in the acute (0–6 weeks) stage after whiplash trauma and to evaluate the course of CxMDs in WAD. A further aim was to determine whether CxMDs in the acute stage after whiplash trauma are predictors of poor long-term recovery.
METHODS
Search strategy
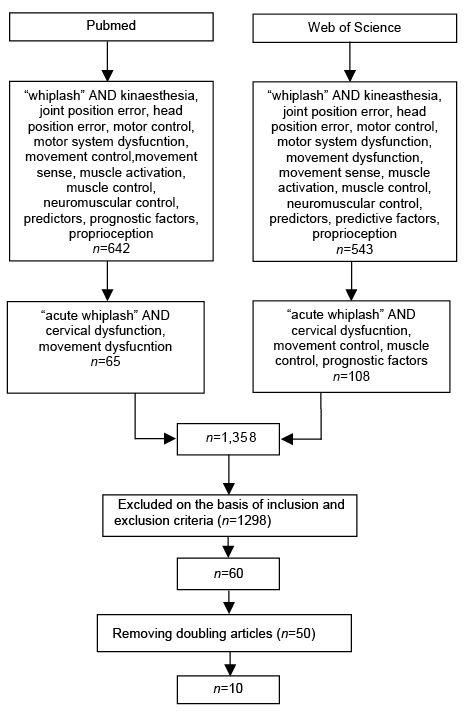
A flow chart of the search strategy is shown in Fig. 1. The search strategy was performed using the electronic databases PubMed (http://www.ncbi.nlm.nih.gov/pubmed/) and Web of Science (http://isiwebofknowledge.com) from their inception until October 2011. Two groups of keywords were used to identify articles concerning cervical motor (dys)function in acute WAD and/or its predictive value for long-term recovery: (i) whiplash; and (ii) cervical dysfunction, kinaesthesia, joint position error, head position error, motor control, motor system dysfunction, movement control, movement dysfunction, movement sense, muscle control, muscle activation, neuromuscular control, proprioception, predictive factors, prognostic factors, proprioception. The keyword for group 1 was combined with keywords for group 2. Since “whiplash” is a broad term it resulted in the identification of studies in the field of acute as well as chronic WAD. Since the primary aim of this study was to study the presence of CxMDs in the acute stage after whiplash trauma, the search strategy was refined if a combination (“whiplash” AND “search term of group 2”) delivered 100 or more items. In that case, “acute whiplash” instead of “whiplash” was used in combination with the respective keyword for group 2. Since we intended to integrate all available literature on cervical motor (dys)function in acute WAD in this systematic literature review, the keywords used were specific and broad. No limits were used during the search strategy.
Fig. 1. Study search strategy.
To identify relevant literature all titles and/or abstracts of the selected articles were screened for inclusion. Articles were eligible for this review if they fulfilled the following criteria: (i) prospective, population-based cohort studies or case-control studies investigating cervical motor (dys)function in acute WAD and/or its predictive value for long-term outcome; (ii) subjects of the study had to be diagnosed as WAD grade I, II or III, as defined by the Quebec Task Force (QTF) classification (i.e. grade 0 = no neck symptoms or physical sign(s); grade I = neck pain, stiffness, or tenderness but no physical sign(s); grade II = neck symptoms and musculoskeletal sign(s) such as decreased range of movement and point tenderness; grade III = neck symptoms and neurological signs) (1); (iii) studies evaluating properties of cervical motor (dys)function within the acute stage (0–6 weeks post-whiplash trauma) after the initial whiplash trauma and/or their predictive value for long-term outcome; (iv) studies presented in English written full text; (v) subjects in the study had to be 18 years or older. No clear definition for acute WAD is available in the literature. Since this literature review focused on CxMDs in the acute stage, it was decided to include articles only if they studied patients who had a whiplash trauma within 6 weeks after the trauma.
Articles were excluded from this systematic literature research if they: (i) were letters to the editor or reviews, hypotheses or papers without scientific data; (ii) included patients with WAD grade IV (fracture or dislocation of the cervical spine) as diagnosed by the QTF classification (1); (iii) studied cervical motor functioning in chronic non-traumatic neck pain and chronic WAD (>12 weeks post-whiplash trauma); (iv) investigated psychological factors and their predictive value for long-term outcome after whiplash trauma; (v) studied the effect of therapy strategies in patients with WAD. In case of doubt concerning the eligibility of the article based on the content of the title and abstract, the full-text version was retrieved and evaluated against the selection criteria, as described above.
Duplicate articles were removed and all remaining articles that met the inclusion criteria were independently reviewed by two reviewers (LD and BR), i.e. both reviewers independently evaluated the included studies. Articles were categorized by the reviewers following study design (case-control, prospective cohort study) and study aim (presence of CxMDs in the acute stage, course of CxMDs in WAD and/or predictive capacity of CxMDs for long-term outcome).
The methodological quality of the selected full-text articles was evaluated independently by the same two reviewers using a literature assessment list for cohort and patient-control studies, respectively. These checklists were obtained via the manual of Evidence Based Guide Development (EBRO) at the Central Counseling Institution (CBO) website (www.cbo.nl). The checklists used to categorize and assess the search results are shown in Table I. After reviewing the selected articles, the results of both researchers were compared and differences were analysed. In case of disagreement in quality assessment, a third reviewer (JN) was asked to screen the manuscript, and in particular the item of disagreement, and make a judgement. To calculate a quality score only the criteria that were or could have been applied were taken into consideration. The total methodological score of each selected article was obtained by summing all the scores of the items that were fulfilled. For further appraisal in this literature study, the selected articles needed to obtain a positive score on at least half of the applicable evaluation criteria.
|
Table I. Evaluation criteria for the methodological quality of the studies |
|
|
Criteria – Prospective cohort study |
Criteria – Case-control study |
|
1. Study groups defined? |
1. Patient group defined? |
|
2. Selection bias avoided? |
2. Control group defined? |
|
3. Exposure clearly described and methodology adequately? |
3. Selection bias avoided? |
|
4. Outcome measurement clearly described and methodology adequately? |
4. Exposure clearly described and methodology adequately? |
|
5. Outcome measurement blind for exposure? |
5. Blind assessment? |
|
6. Follow-up? |
6. Confounders identified and adequately taking into account during the analysis? |
|
7. Selective loss-to-follow-up avoided? |
|
|
8. Confounders/prognostic factors identified and adequately taking into account during analysis? |
|
RESULTS
Study selection
Based on the above-mentioned literature research, a final total of 10 articles were selected for further appraisal (5, 20–28). Rejection was based mostly on the participants’ condition not meeting the inclusion criteria of acute WAD, e.g. studies investigating patients with chronic WAD (i.e. complaints persisting for at least 3 months after the whiplash trauma) and those with non-traumatic neck complaints. The manuscripts were independently screened and reviewed by the two researchers, using the literature assessment lists described above.
Study characteristics
Nine of the 10 selected articles were prospective studies (5, 20–26, 28), of which 2 also compared the findings between patients (persons with a whiplash injury) and control subjects (asymptomatic subjects and persons with an acute ankle distortion) (5, 22). One manuscript was a case-control study (27). The 10 selected articles comprised the findings concerning the presence of CxMDs, the course of CxMDs in WAD, and the predictive value of CxMDs for long-term recovery of 5 different cohorts. The characteristics of the various cohorts are shown in Table II.
|
Table II. Description of the cohorts included in the systematic review |
|||||||||
|
Cohort number |
Authors |
Study design |
Source |
Sample |
WAD classification |
Inception time |
Cervical motor function measures |
Follow-up |
Outcome measure at follow-up |
|
1 |
Kasch et al., 2001 (20) Kasch et al., 2001 (22) |
Prospective Prospective |
Emergency department |
141 132/141 |
Grade not mentioned |
1 week |
Active cervical range of movement |
1, 3, 6, 12 months |
Handicap described in terms of changes in pre-injury working hours and work capacity. |
|
2 |
Kasch et al., 2008 (21) |
Prospective |
The Danish Pain Research Centre, The Danish Back Research Centre |
625/688 |
Grade I–II–III (QTF classification |
1 week |
Active cervical range of movement |
3, 6, 12 months |
1. Handicap defined as more than 3 months sick leave during the last 6 months, work inability during the last month or not working anymore because of the accident. 2. Neck pain and headache (11-points box scales) |
|
3 |
Sterling et al., 2003 (5) Sterling et al., 2004 (27) Sterling et al., 2005 (28) Sterling et al., 2006 (26) |
Prospective Case-control Prospective Prospective |
Accident and emergency departments, primary care practices, advertisement on radio and in print media, Brisbane |
66 80 76/80 65/80 |
Grade II–III (QTF classification) |
4 weeks |
Active cervical range of movement, cervical kinaesthesia (joint position error), superficial neck flexor muscle activity |
2, 3, 6 months, 2–3 years |
Persistent pain and disability measured with the Neck Disability Index (Vernon & Mior 1991, (29)) – Recovered (< 8 NDI) – Mild pain and disability (10–28 NDI) – Moderate/severe pain and disability (> 30 NDI) |
|
4 |
Nederhand et al., 2003 (24) Nederhand et al., 2006 (23) |
Prospective Prospective |
Emergency department |
92 92 |
Grade I–II (QTF classification) |
1 week |
Muscle activation pattern of the upper trapezius muscles |
1, 2, 3, 6 months |
|
|
5 |
Oddsdottir & Kristjansson, 2011 (25) |
Prospective |
Emergency department, Iceland |
47/74 |
Grade I–II–III (QTF classification) |
4 weeks |
Cervical kinaesthesia (Fly test and head-neck relocation test) |
3, 6, 12 months |
|
|
Bold and underlined figure is the follow-up end-point used to examine prognostic associations. |
|||||||||
The diagnostic criteria used to include patients with WAD were not always clearly described. The severity of the symptoms was not mentioned within the inclusion and exclusion criteria in one cohort (20, 22). In the other cohorts (n = 4), the QTF classification was used to select the study participants based on the severity of the symptoms (1). Patients diagnosed as WAD grade II were mostly included (4 cohorts). Patients with WAD grade I and WAD grade III were included in 3 cohorts.
The presence of CxMDs, such as reduced active range of movement (aROM), altered muscle activation patterns and disturbed kinaesthesia, was investigated in 4 out of 5 cohorts within 6 weeks after the whiplash trauma (5, 22–25, 27). The aROM was examined in 2 out of the 5 cohorts (5, 22, 27), cervical kinaesthesia was evaluated in 2 cohorts (5, 25, 27), muscle activity in the upper trapezius muscles was described in 1 cohort (23, 24) and the activity of the superficial neck flexors was assessed in 1 cohort (5, 27). To evaluate the course of CxMDs in WAD, the patients of 4 cohorts were followed up to 3 months or 2–3 years post-whiplash trauma (5, 22–26). The predictive value of CxMDs on handicap, pain and disability at 6, 12 months or 2–3 years after the initial whiplash trauma was assessed in 3 cohorts (20, 21, 26, 28).
Two out of the 5 cohorts used the Neck Disability Index (NDI), measuring self-reported neck pain and disability, in order to segregate the patients into subgroups. Sterling et al. (5, 26, 27, 28) calculated the overall NDI score by totalling the individual items and multiplying by 2 (score out of 100), while Nederhand et al. (23, 24) used a score out of 50 (totalling the individual items) as overall NDI score. In order to correctly compare and interpret the findings of the different cohorts, the NDI scores reported in this literature study were overall scores out of 100. Therefore, the NDI scores as reported by Nederhand et al. (23, 24) were multiplied by 2 for interpretation in this literature study.
Methodological quality
The agreement in the methodological quality of the scoring between the two reviewers was 85% (66/78 items). Items of disagreement were further screened by a third reviewer (JN), who also made the final decision. A score, dependent on the applicable evaluation items, was given to the selected studies. The results of the methodological quality assessment are shown in Table III.
|
Table III. Methodological quality assessment of the included articles |
||||||||||
|
Design |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
Total |
|
|
Kasch et al., 2001 (20) |
Prospective |
+ |
+ |
/ |
+ |
/ |
+ |
– |
+ |
5/6 |
|
Kasch et al., 2001 (22) |
Prospective |
+ |
+ |
/ |
+ |
/ |
+ |
– |
+ |
5/6 |
|
Kasch et al., 2008 (21) |
Prospective |
+ |
+ |
+ |
+ |
– |
+ |
– |
– |
5/8 |
|
Sterling et al., 2003 (5) |
Prospective |
+ |
+ |
/ |
+ |
/ |
– |
– |
+ |
4/6 |
|
Sterling et al., 2004 (27) |
Case-control |
+ |
+ |
+ |
+ |
– |
+ |
5/6 |
||
|
Sterling et al., 2005 (28) |
Prospective |
+ |
+ |
/ |
+ |
/ |
+ |
+ |
+ |
6/6 |
|
Sterling et al., 2006 (26) |
Prospective |
+ |
+ |
/ |
+ |
/ |
+ |
+ |
– |
5/6 |
|
Nederhand et al., 2003 (24) |
Prospective |
+ |
+ |
/ |
+ |
/ |
+ |
+ |
+ |
6/6 |
|
Nederhand et al., 2006 (23) |
Prospective |
+ |
+ |
/ |
+ |
/ |
+ |
– |
– |
4/6 |
|
Oddsdottir & Kristjansson, 2011 (25) |
Prospective |
+ |
+ |
+ |
+ |
/ |
+ |
+ |
+ |
7/7 |
|
Prospective study design: 1: Groups defined?; 2: Selection bias?; 3: Exposure defined and methodology adequately?; 4: Outcome measurements defined and methodology adequately?; 5: Outcome measurement blind for exposure?; 6: Follow-up?; 7: Selective loss-to-follow-up avoided?; 8: Confounders/prognostic factors identified? Case-control study design: 1) Patient group defined?; 2) Control group defined?; 3) Selection bias avoided?; 4) Exposure defined and methodology adequately?; 5) Blind assessment?; 6) Confounders identified? +: clearly described; –: not mentioned; /: not applicable. |
||||||||||
Cervical motor (dys)function in the acute stage after whiplash trauma (<6 weeks) and its course in whiplash-associated disorders
Active cervical range of movement. Active range of movement (aROM) was studied in 2 out of the 5 cohorts. Reduced cervical aROM was demonstrated in all WAD groups (i.e. in those with mild as well as moderate and severe pain and disability) between 1 week and 1 month after the initial trauma (5, 22, 27). The most restricted movement was extension, followed by flexion. Neck mobility was inversely related to neck pain intensity (22). The group with severe pain and disability (mean NDI 69.5) demonstrated reduced extension and left rotation compared with the moderate (mean NDI 39.5) and mild (mean NDI 15.6) group within 1 month post-injury (27). Those with mild (NDI 10–28) and moderate/severe (NDI > 30) symptoms at 3 months demonstrated less range of flexion, extension, left and right rotation at 1 month post-whiplash trauma. The recovered (NDI < 8) group showed a greater range of extension at 1 month post-whiplash trauma than those with mild and severe symptoms, but less than controls (5). Increasing age was related to reduced cervical aROM, but gender had no effect on aROM (5, 22).
In those who recovered and reported mild symptoms at 3 months post-whiplash trauma, the aROM (in all directions) was improved and similar to the controls. In the moderate/severe group, the restricted aROM persisted at 3, 6 months and 2–3 years post-whiplash trauma (5, 26). Others found no significant differences in cervical aROM or in extension, flexion, lateral flexion, or rotation between patients with WAD and those with ankle distortion at 3 months post-whiplash trauma (22).
The range of active cervical movement was measured in 3 dimensions using a Cervical aROM instrument (performance Attainment Associates, Roseville, MN, USA) (22) and an electromagnetic motion tracking device (Fastrak, Polhemius, Colchester, USA) (5, 27). The Cervical aROM device has been shown to be an instrument with a good concurrent validity and acceptable to good reliability (30–37). The Fastrak system, used to evaluate cervical aROM in neck pain disorders, has been shown to be reliable and accurate to within ± 0.2º (38–41).
Cervical kinaesthesia. Cervical kinaesthesia was evaluated in 2 out of the 5 cohorts. Altered cervical kinaesthesia was observed in patients with moderate or severe symptoms within 1 month; this remained at 3, 6 months and 2–3 years post-whiplash trauma (5, 26, 27). The group with moderate and severe symptoms at 1 month and persistent moderate/severe symptoms at 3 months showed greater joint position errors (JPEs) only when relocating to neutral from right rotation compared with the recovered, mild and control group (5, 27). In addition, those with severe pain and symptoms also demonstrated greater JPEs only when relocating to neutral from extension at 1 month post-whiplash trauma. There were no group differences for JPE (left rotation) (27). No effect of age and gender on JPE was observed (5).
Oddsdottir & Kristjansson (25) observed two different courses of disturbed cervical kinaesthesia in patients with WAD (25). Approximately half of the patients who demonstrated decreased movement and relocation accuracy within 1 month showed improved movement and relocation accuracy 12 months post-whiplash trauma. The other half of the participants had better performances on the two kinaesthetic tests at 1 month post-whiplash trauma compared with 12 months post-whiplash trauma (25). We were not able to extract relevant information in relation to the primary aim of the literature research from the latter study (25).
The accuracy of head relocation to the neutral position (JPE) was measured according to Revel et al. (42) by using the Fastrak system (5, 25–27). The head-to-neutral head position test was found to be reliable (43). Disturbances of cervical movement control were evaluated with the Fly test (25). During this test, tracking sensors were attached to the head and subjects were asked to track a cursor (“the fly”) on a computer screen (6). The Fly method provides reliable and valid measures for movement control of the cervical spine (44).
Muscle activation patterns of the upper trapezius muscles. Muscle activation patterns of the upper trapezius muscles were measured in one cohort. The ability to relax the upper trapezius muscles after physical activity was, within 1 month post-whiplash trauma, similar in those who were recovered (0–8 NDI), had mild (10–28 NDI), moderate (30–48 NDI) and severe symptoms (50–100 NDI) at 24 weeks post-whiplash trauma. No differences in level of muscle reactivity between the 4 subgroups, or changes in muscle reactivity over time (1, 4, 8, 12 and 24 weeks post-whiplash trauma) were observed (24).
Decreased muscle activation in the upper trapezius during isometric and dynamic muscle activity was observed in the moderate (30–48 NDI) and severe (50–100 NDI) group compared with the mild (10–28 NDI) and recovered (0–8 NDI) group. No changes in muscle activity, isometric or dynamic, were observed over time (1, 4, 8, 12 and 24 weeks post-whiplash trauma) (24). Another study by Nederhand et al. (2003) revealed a lower level of electromyography (EMG) activity in the upper trapezius muscles at 1 week post-whiplash trauma in the group who was disabled (>10 NDI) at follow-up (24 weeks post-whiplash trauma) (23).
A decreased level of muscle activation in the upper trapezius muscles was associated with an increased level of fear of movement and pain intensity. The association between muscle activity and fear of movement was stronger in patients reporting high pain intensity. The association between pain level and muscle activity in the upper trapezius muscles decreased with time after the whiplash trauma (23).
The muscle reactivity (the difference in pre- and post-exercise EMG levels), isometric EMG levels during the performance of an isometric physical task) and dynamic muscle activity (EMG levels during the performance of a dynamic physical task) of the upper trapezius muscles were measured by surface EMG following the recommendations of the European Community concerted action Surface EMG for Non-invasive Assessment of Muscles project (45, 46).
Activity of the superficial neck flexors. The activity of the superficial neck flexors was examined in one cohort. There is evidence of increased activity of the superficial neck flexors (sternocleidomastoideus muscles) in patients with mild, moderate and severe pain and disability compared with controls within 1 month after whiplash trauma, with the severe group displaying significantly greater EMG activity than the mild and moderate group (27).
The differences in activity of the superficial neck flexors between the groups persisted over time. EMG activity of superficial neck flexors was still increased in the mild and recovered group compared with controls at 3, 6 months and 2–3 years post-whiplash trauma (5, 26). At 2–3 years post-whiplash trauma, higher EMG activity was observed in the moderate/severe group and no differences were found between the mild and recovered group (26). There was no effect of age and gender on activity of the superficial neck flexors (5).
While the moderate/severe group showed elevated levels of fear of movement (TAMPA scores), differences in motor function between the WAD groups remained even when TAMPA scores were included in the analysis. A weak correlation between TAMPA scores and motor function measurement was found (5).
Surface EMG was used to measure the activity of the superficial neck flexors (both sternocleidomastoideus muscles) during the craniocervical flexion test (CCFT). The CCFT is a test of progressive craniocervical flexion (head-nodding, such as in indicating “yes”) and aim at evaluating the activity and endurance in the deep neck flexors (longus capitis and colli muscles) (47). Data supporting the reliability and validity of the CCFT for patients with neck pain are available (48–50).
Predictive value of cervical motor dysfunction in the acute stage after whiplash trauma for long-term recovery
The predictive value of cervical neck mobility in the acute stage for long-term recovery was assessed in two cohorts. The predictive capacity of kinaesthesia and activity in the superficial neck flexors was evaluated in one cohort. Two studies demonstrated reduced aROM as a predictive factor for developing handicap at 1 year post-whiplash trauma (20, 21). The cervical aROM test predicted handicap with a sensitivity of 73% and a specificity of 91% 1 year after the acute whiplash trauma (20). Persons with initial reduced aROM had 4.6 times greater risk of developing persistent long-term (1 year post-whiplash trauma) disability. The initial reduced aROM was not associated with long-term neck pain or headache (21).
In contrast with latter studies (20, 21), Sterling et al. (26, 28) demonstrated that reduced aROM was a predictive factor for higher pain and disability at 6 months, but not at 2–3 years post-whiplash trauma.
Neither the JPE nor the activity of the superficial neck muscles during CCFT were predictive factors for poor outcome 6 months after the whiplash trauma (28).
A summary of the findings concerning the presence of CxMDs in the acute stage, the course of CxMDs in WAD, and the predictive capacity of CxMDs for long-term recovery is shown in Table IV.
|
Table IV. Summary of findings concerning cervical motor dysfunctions in the included cohorts: presence in the acute stage, course in whiplash-associated disorders (WAD), predictive value for long-term recovery |
||||
|
Cohort |
Authors |
Occurrence of CxMDs in the acute stage |
Course CxMDs in WAD |
Predictive value of CxMDs for long-term recovery |
|
1 |
Kasch et al., 2001 (20) Kasch et al., 2001 (22) |
– Reduced aROM (extension > flexion) – Inverse relationship between aROM and neck pain |
– No reduced aROM in patients with WAD at 3 months post-whiplash |
– Reduced initial neck mobility predicted handicap one year post-whiplash |
|
2 |
Kasch et al., 2008 (21) |
|
|
– Reduced initial neck mobility was associated with a 4.6-fold risk increase for handicap at 1 year post-whiplash – Initial reduced aROM was not associated with long-term neck pain or headache |
|
3 |
Sterling et al., 2003 (5) Sterling et al., 2004 (27) Sterling et al., 2005 (28) Sterling et al., 2006 (26) |
– Less range of motion (all directions) – Less extension and left rotation in patients with severe pain and disability – Less range of motion (all directions) in patients with mild and moderate/severe symptoms at 3 months – Greater range of extension in those who recovered at 3 months, but less than controls – Greater JPEs (right rotation) in the moderate and severe group – Greater JPEs (extension) in the severe group – Greater JPE (right rotation) in group with moderate/persistent symptoms at 3 months – Increased activity of superficial neck flexors in severe group – Increased activity of superficial neck flexors in moderate and mild group compared with controls – Increased activity of superficial neck flexors in group with moderate/severe symptoms at 3 months – Increased activity of superficial neck flexors in group with mild symptoms and recovered at 3 months compared with controls |
– No longer movement loss in the recovered and mild group at 3 months post-whiplash – Reduced aROM remained in the moderate/severe group at 3 months post-whiplash – Reduced cervical aROM remained in group with persistent moderate/severe symptoms at 2–3 years post-whiplash – Greater JPE remained in the moderate/severe group at 3 months post-whiplash – Greater JPE remained in the moderate/severe group at 2–3 years post-whiplash – Increased activity in superficial neck flexors persisted in all WAD groups at 3 months post-whiplash – Increased activity of superficial neck flexors persisted in moderate/severe, mild and recovered group at 2–3 years post-whiplash – No difference in EMG activity between mild and recovered group at 2–3 years post-whiplash |
– Decreased active range of left rotation was associated with higher NDI on 6 months – Reduced cervical aROM was no longer a predictor for higher pain and disability at 2–3 years post-whiplash – Neither JPE nor activity of superficial neck flexors were predictive factors for higher NDI at 6 months post-whiplash |
|
4 |
Nederhand et al., 2003 (24) Nederhand et al., 2006 (23) |
– No differences in muscle reactivity of the upper trapezius muscles between the recovered, mild, moderate and severe group – Decreased muscle activation in the upper trapezius during isometric and dynamic activity in the moderate and severe group – Decreased activity in the upper trapezius muscles in the group who was disabled at 6 months post-whiplash – Decreased activity in the upper trapezius muscles was associated with increased level of fear and pain intensity |
– No changes in muscle reactivity of upper trapezius muscles at 8, 12 and 24 weeks post-whiplash – Decreased isometric and dynamic muscle activity in the upper trapezius muscles remained at 8, 12 and 24 weeks post-whiplash – The effect of pain level on muscle activity decreased over time (1–24 weeks post-whiplash) |
|
|
5 |
Oddsdottir & Kristjansson, 2011 (25) |
– Two different courses of disturbed cervical kinaesthesia |
|
|
|
CxMD: cervical motor dysfunction; QTF: Quebec Task Force; aROM: active range of movement; JPE: joint position error; NDI: Neck Disability Index; WAD: whiplash-associated disorders; EMG: electromyography. |
||||
DISCUSSION
Cervical motor dysfunctions, such as reduced aROM, disturbed cervical kinaesthesia, and altered cervical muscle activity (upper trapezius and superficial neck flexors), are commonly demonstrated soon after the initial whiplash trauma (5, 22–25, 27).
Cervical motor dysfunction in acute whiplash-associated disorders and its predictive value for long-term recovery
While reduced aROM appears to be a key clinical finding in the acute stage after whiplash trauma (5, 22, 27), there seems to be conflicting evidence regarding the progression of the CxMD. Kasch et al. (22) demonstrated that cervical mobility improves, and neck mobility returns to normal, within 3 months after whiplash trauma. In contrast with this study (22), two studies that classified the patients in groups with mild to severe pain and disability report restricted neck mobility in patients with moderate/severe pain at 3, 6 months and 2–3 years post-whiplash trauma (5, 26). The findings of these studies appear to be at odds. The methodological quality of the above-mentioned studies was equivalent, suggesting that factors other than study quality may explain the opposing findings. Kasch et al. (22) did not subclassify the patients and did not take patients’ level of pain and disability into account. These findings suggest the need to differentiate between patients with a mild vs a complex clinical picture of WAD.
The findings addressing the predictive capacity of reduced neck mobility for long-term (poorer) primary outcome after whiplash trauma are inconsistent. Kasch et al. (20, 21) revealed that those with reduced neck mobility in the acute stage had an increased risk of chronic handicap at 1 year post-whiplash trauma. No associations between initial reduced cervical aROM and secondary outcome measurement (i.e. neck pain and headache assessed by means of the Copenhagen Neck Disability Scale and an 11-point box scale) were found at 1 year post-whiplash trauma (21). Sterling et al. (26) showed that reduced neck mobility was not a significant predictor of higher pain and disability levels at 2–3 years post-whiplash trauma. It is important to point out that different outcome measurements to evaluate recovery were used in both studies (i.e. handicap and level of pain and disability, respectively). Only 1 study used a validated instrument to measure outcome (i.e. NDI) (26), which may explain the discrepancy across studies. In addition, these results should be interpreted with regard to the methodological quality of the studies. Sterling et al. (26) and Kasch et al. (20) found a positive score for 5/6 items, while Kasch et al. (21) found a score of 5/8. In the latter study, participants were divided into low-risk and high-risk treatment groups receiving different treatment strategies. The treatment strategies were not identified as possible confounders. The assessor was only blinded for treatment within each group, and not for belonging to the low-risk or high-risk treatment group, and the loss-to-follow up was not sufficiently described. In addition, there was a substantial proportion of drop-outs and the reasons for dropping out were not explained in detail. Hence, the contribution of these factors to the outcome measurements cannot be ruled out.
The varying results concerning the presence and predictive capacity of reduced cervical aROM for long-term outcome are probably due to heterogeneity of included WAD population and different outcome measurements. In some cohorts only patients with WAD grade I–II or WAD grade II–III were included, while in others patients with WAD grade I, II and III (as defined by the QTF classification (1)) were recruited. In addition, some authors differentiated between patients with mild, moderate and severe symptoms following acute whiplash trauma based on the level of pain and disability (NDI score) (5, 26, 27), while others did not differentiate (22). There is a need to differentiate between patients and to identify subgroups in the WAD population. Furthermore, it is recommended that researchers use validated instruments to evaluate the level of recovery (primary outcome).
Based on this systematic review, there is evidence of altered neck muscle activity in patients with acute WAD, which remained over time (6 months to 2–3 years after whiplash trauma) (5, 24, 26, 27). Again, differences between patients, based on the level of disability, were present. Patients with severe symptoms demonstrated decreased activity in the upper trapezius and increased activity in the sternocleidomastoideus muscles compared with those with mild symptoms soon after the whiplash trauma (24, 27). Furthermore, Sterling et al. (27) found altered activity in the sternocleidomastoideus muscles in the moderate and mild WAD groups (compared with controls) (24, 27). It is important to note that Nederhand et al. (24) did not include a healthy control group.
The above-mentioned CxMDs (i.e. reduced cervical aROM, deficits in kinaesthesia, and altered cervical muscle activation patterns) were of limited predictive value for long-term recovery (26, 28). In addition, these findings were non-specific for WAD (8, 13, 51). It has been suggested that the observed CxMDs are unable to explain the complex clinical picture of WAD.
Further research is needed into the underlying mechanisms of CxMDs in WAD. Further work concerning predictive factors for poor long-term recovery within a biopsychosocial framework is also recommended. In addition to CxMDs and sensory disturbances, the role of psychosocial factors (e.g. post-traumatic stress, fear avoidance, social support) have been studied in patients with WAD (26, 28, 52, 53). In concordance with current knowledge and insight in WAD, which points towards physiological, psychological as well as central underlying mechanisms, a new classification system reflecting the complexity of WAD, taking into account the role of motor, psychosocial as well as sensory (e.g. hypersensitivity of the central nervous system (CNS) (54–56)) disturbances, has been proposed (57). However, none of the 10 selected studies used this new multi-faced WAD classification system. This should be incorporated into future research in this area.
Kasch et al. (58) recently developed a risk assessment tool that aims to identify those patients who are at risk for non-recovery at an early time-point after whiplash trauma. They attempted to segregate patients early after trauma into different risk strata based on predictive factors (i.e. active neck mobility, pain score of combined headache and neck pain together, and summation of non-painful symptoms). The risk assessment score was found to be a valuable tool for grading patients soon after whiplash trauma. In addition, the risk strata appeared to be associated with measurements of sensitization of the nociceptive system, severity of psychological distress, and measures of neck strength and duration, reflecting the biopsychological nature of WAD (58). Further research is needed to consolidate this model in new and different settings. From the clinical viewpoint, it makes sense to develop a prediction model (based on previous findings concerning prediction of poor outcome after whiplash trauma) that can grade patients early after whiplash trauma, and that can identify those at risk for developing persistent problems. Internal and external validation is important prior to the use of such a prediction model in clinical practice.
Methodological issues of the included studies
Based on the methodological issues identified in the selected articles, it is recommended that future studies take into account possible confounders in order to prevent bias. Statistical adjustment for variables that may confound the relationship between the proposed predictive factor and the outcome is required. Four out of the 9 prospective studies did not clearly describe potential confounders and, consequently, it is not obvious how these factors could have influenced the findings (21, 23, 25, 26). Although accounting for all possible confounders is nearly impossible, statistical adjustment for variables that may definitely impact the outcome is warranted. For example, the influence of therapy strategies on the outcome measurement cannot be ruled out if this is not taken into account in the statistical analyses. In the study of Kasch et al. (21), participants were divided into high-risk and low-risk treatment groups receiving different treatment strategies, such as verbal information, immobilization and McKenzie physiotherapy. It is likely that the applied strategies had an effect on the outcome (i.e. handicap 1 year post-whiplash trauma). Care must be taken when interpreting these results. Furthermore, drop-outs must be described clearly in order to avoid selective loss to follow-up. Four out of the 9 prospective studies failed on these criteria, mostly due to insufficient information concerning the reason for drop-out and baseline/demographic characteristics of those who drop out.
Limitations of the present study
It was not possible to perform a meta-analysis in the present study due to the variability in the cervical motor function and outcome measurements. In addition, the results reported in the selected articles contained those of only 5 different cohorts, and the various cervical motor functions (i.e. active cervical aROM, cervical kinaesthesia and cervical muscle activity) were not examined in each cohort. The data necessary for meta-analysis (e.g. degree of variability, strength of association or effect size) were frequently not reported. It is recommended that future studies take into account the methodological quality criteria, use validated measurements, and report strength of association and degree of variability. A summary of important criteria with regard to the design and reporting of prognostic studies in the field of WAD is provided in a recent paper by Kamper et al. (59).
In conclusion, there is consistent evidence for CxMDs soon after whiplash trauma. While these CxMDs are greater in subjects reporting higher levels of pain and disability, they are also apparent in those with mild pain and disability and even in those who recover from the injury. The CxMDs persist over time in those with moderate/severe pain and disability. However, there is some inconsistency concerning the course of the CxMD in WAD, probably due to a lack of subclassification of the patients in some studies. These CxMDs are of limited predictive value for long-term recovery. Further studies are warranted to investigate the complex nature of all underlying mechanism(s) within a biopsychosocial framework.
ACKNOWLEDGEMENT
This study was financially supported by a grant (41/FA020000/3/3995) from the research council of the University of Antwerp, Belgium.
The authors declare no conflicts of interest.
REFERENCES

