Murat Kara, MD1, Tülay Tiftik, MD1, Öznur Öken, MD1, Nuray Akkaya, MD2, Hakan Tunç, MD1 and Levent Özçakar, MD3
From the 1Ankara Physical Medicine and Rehabilitation Education and Research Hospital, Ankara, 2Pamukkale University Medical School, Department of Physical Medicine and Rehabilitation, Denizli, 3Hacettepe University Medical School, Department of Physical Medicine and Rehabilitation, Ankara, Turkey
OBJECTIVE: To assess femoral cartilage thickness in patients with spinal cord injury.
SUBJECTS: Forty-six patients with SCI (35 men, 11 women; mean age: 33.6 years (standard deviation 8.1) and 46 age-, sex- and body mass index (BMI)-matched healthy subjects were enrolled.
METHODS: Patients were evaluated with the American Spinal Injury Association (ASIA) Impairment Scale, Modified Ashworth Scale, Walking Index for Spinal Cord Injury, and Functional Independence Measurement. Mid-point ultrasonographic femoral cartilage thickness measurements were taken from the right lateral condyle, right intercondylar area, right medial condyle, left medial condyle, left intercondylar area and left lateral condyle.
RESULTS: Ultrasonographic measurements revealed significantly thicker values in the intercondylar areas (bilaterally) and the medial condyle (left knee) of patients with spinal cord injury compared with those of controls. When the subgroups were compared with their paired healthy controls, measurements pertaining to the motor complete group were found to be significantly thicker in the intercondylar areas (bilaterally) and the medial condyle (left knee). Cartilage thickness values correlated negatively with the duration of immobilization (for bilateral intercondylar areas), and with BMI and ASIA level (for bilateral lateral condyles).
CONCLUSION: Femoral cartilage thicknesses were found to change after spinal cord injury, and to have a negative correlation with disease duration and severity. Future studies including histological evaluations may elucidate whether such changes are favourable for the knee joints of patients with spinal cord injury.
Key words: spinal cord injury; femoral cartilage; thickness; ultrasound; immobilization.
J Rehabil Med 2013; 45: 00–00
Correspondence address: Murat Kara, Ankara Fizik Tedavi Rehabilitasyon Eğitim ve Araştırma Hastanesi, Sıhhıye, Ankara, Turkey. E-mail: mkaraftr@yahoo.com
Submitted December 12, 2011; accepted September 26, 2012
INTRODUCTION
Spinal cord injury (SCI) is one of the most common causes of long-term unloading and immobilization, whereby changes in the periarticular connective tissue, contractures, periarticular osteoporosis, joint space narrowing and articular cartilage degeneration have been described (1–10).
A literature search into the effects of unloading, due to immobilization, on the joint cartilage, revealed a number of reports showing increased, decreased or unchanged thickness in animal models (11–14). However, there are very few studies in humans that have evaluated the knee cartilage of patients with SCI using magnetic resonance imaging (MRI). The thickness of knee cartilage in patients with SCI has been shown to be decreased, both in cross-sectional comparison with healthy controls (1) and during a 1-year prospective follow-up (2). However, these studies were performed in a very limited number of patients with inhomogeneous disease course. Focussing on the possible impact of cartilage alterations later in their lives, we reasoned that assessment of the femoral cartilage in a larger group of patients with SCI would elucidate the relevant consequences.
The objectives of this study were therefore: (i) to compare the femoral cartilage thicknesses of patients with SCI with those of healthy subjects; (ii) to study the correlation between cartilage thickness and disease-related parameters in these patients. Ultrasonography, which has been shown previously to be a valid and reliable method for evaluating femoral cartilage, was used in this study (15–19).
METHODS
A total of 46 patients with SCI (35 men, 11 women) and 46 able-bodied age-, sex- and BMI-matched controls (35 men, 11 women) were enrolled in this multi-centre cross-sectional study. Subjects with a history of knee arthritis or surgery before SCI were excluded. All patients were informed about the study procedure and consented to participate. The study protocol was approved by the local ethics committee of one of the attending centres.
Initially, demographic features of the subjects, including age, sex, body weight/height, occupation and other clinical characteristics, were noted. Patients were asked to evaluate their average daily standing/not standing time since their injury. Immobilization duration was defined as the time since injury for which patients reported daily standing with a standing frame or crutches and braces of less than 1 h daily, or staying in a bed or wheelchair all day.
Outcome measures
The functional status of the patients was scored according to the American Spinal Injury Association (ASIA) Impairment Scale (20). Accordingly, the patients were divided into two groups, motor complete (ASIA A and B) and motor incomplete (ASIA C and D).
The Modified Ashworth Scale (MAS) was used to grade the spasticity of the knee flexor and extensor muscles (21). Walking ability was evaluated with the Walking Index for Spinal Cord Injury (WISCI II), which assesses the amount of physical assistance, braces or devices required to walk 10 m. The scores on the WISCI II ranged from 0 (unable to stand and/or participate in walking) to 20 (ambulates with no devices, with brace and no assistance is designated) (22). Motor items of the Turkish version of the Functional Independence Measurement (FIM) scale (scoring from 13 to 91) were used to evaluate motor functioning (23–25).
Ultrasonographic cartilage measurements
Ultrasonographic thickness measurements of the cartilage were made with a linear probe (7–12 MHz Logiq P5, GE Medical Systems, California, USA). With subjects sitting in a comfortable position on the examination table with their knees in maximum flexion, the probe was placed in an axial position on the suprapatellar area. The distal femoral cartilage was visualized as a strongly anechoic structure between the sharp bony cortex and the suprapatellar fat. Three (mid-point) measurements were taken from each knee, at the right lateral condyle (RLC), the right intercondylar area (RIA), the right medial condyle (RMC), the left medial condyle (LMC), the left intercondylar area (LIA), and the left lateral condyle (LLC) (Fig. 1).
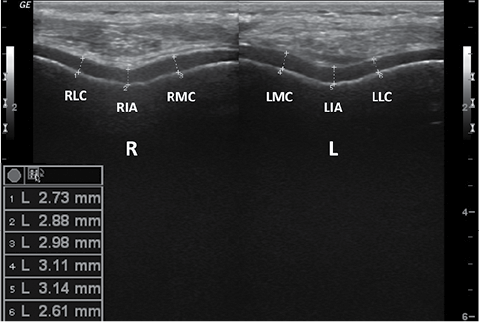
Fig. 1. Ultrasonographic images (suprapatellar axial view) demonstrating bilateral femoral cartilage measurements of patients with spinal cord injury. RLC: right lateral condyle, RIA: right intercondylar area, RMC: right medial condyle, LMC: left medial condyle, LIA: left intercondylar area, LLC: left lateral condyle, R: right, L: left.
Statistical analysis
Data were expressed as mean (standard deviation (SD)) for nominal variables, and as median (minimum–maximum) for ordinal variables. Paired samples t-test was used to compare mean knee cartilage thickness values (SCI vs able-bodied subjects). Correlations between patients’ characteristics and femoral cartilage thicknesses were analysed using Pearson’s correlation coefficients. Statistical analysis was performed with SPSS 15.0. Statistical significance was set at p < 0.05.
RESULTS
The demographic and clinical characteristics of the patients are shown in Table I. The mean age of the patients and controls was 33.6 years (SD 8.1) (age range 19–47 years). There was no statistical difference between the groups in terms of BMI; the mean BMI of the patients and controls were 23.4 kg/m2 (SD 3.7) and 24.1 kg/m2 (SD 2.9), respectively.
|
Table I. Clinical characteristics of patients with spinal cord injury (n=46) |
|
|
Patients |
|
|
Age, years, mean (SD) |
33.6 (8.1) |
|
Disease duration, months, mean (SD) |
26.3 (34.2) |
|
Duration of immobilization, months, mean (SD) |
11.5 (16.7) |
|
Level of the lesion, n (%) |
|
|
Cervical |
12 (26.1) |
|
Thoracic |
25 (54.3) |
|
Lumbar |
9 (19.6) |
|
ASIA level |
|
|
A |
17 (37.0) |
|
B |
9 (19.6) |
|
C |
10 (21.7) |
|
D |
10 (21.7) |
|
FIM motor score (median range) |
62 (13–91) |
|
WISCI-II (median range) |
5 (0–20) |
|
LE-MAS (median range) |
0 (0–4) |
|
SD: standard deviation; ASIA: American Spinal Injury Association; WISCI-II: Walking Index for Spinal Cord Injury; LE-MAS: Lower Extremity Modified Ashworth Scale; FIM: Functional Independence Measurement. |
|
Mean femoral cartilage thickness values of the subjects are shown in Table II. Compared with those of the controls’, cartilage measurements were significantly thicker at intercondylar areas bilaterally and at the medial condyle on the left knee.
When subgroups were compared with their paired healthy controls, cartilage measurements were significantly thicker at intercondylar areas (right knee p = 0.039, left knee p = 0.015) and at the medial condyle (left knee p = 0.028) only in the motor complete group.
|
Table II. Comparison of femoral cartilage thickness measurements (mm) |
|||
|
Patients Mean (SD) |
Controls Mean (SD) |
p-value |
|
|
RLC |
2.24 (0.5) |
2.22 (0.4) |
0.910 |
|
RIA |
2.54 (0.6) |
2.20 (0.5) |
0.007 |
|
RMC |
2.28 (0.5) |
2.19 (0.5) |
0.417 |
|
LMC |
2.31 (0.5) |
2.10 (0.4) |
0.028 |
|
LIA |
2.60 (0.7) |
2.19 (0.5) |
0.002 |
|
LLC |
2.29 (0.6) |
2.20 (0.5) |
0.399 |
|
SD: standard deviation; SCI: spinal cord injury; RLC: right lateral condyle; RIA: right intercondylar area; RMC: right medial condyle; LMC: left medial condyle; LIA: left intercondylar area; LLC: left lateral condyle. |
|||
Correlation coefficients between cartilage thickness values and patients’ characteristics showed that cartilage thickness values were significantly (all p < 0.05) negatively correlated with duration of immobilization at bilateral intercondylar areas (right knee r = –0.371, left knee r = –0.349), and with BMI (right knee r = –0.380, left knee r = –0.306) and ASIA level (right knee r = –0.408, left knee r = –0.424) at bilateral lateral condyles (Table III).
|
Table III. Correlations between patients’ characteristics and cartilage thickness values |
|||||||
|
|
RLC |
RIA |
RMC |
LLC |
LIA |
LMC |
|
|
Age |
–0.063 |
–0.064 |
–0.051 |
–0.092 |
–0.061 |
–0.076 |
|
|
Disease duration |
–0.199 |
–0.163 |
–0.130 |
–0.123 |
–0.173 |
–0.051 |
|
|
Duration of immobilization |
–0.251 |
–0.371* |
–0.115 |
–0.163 |
–0.349* |
–0.053 |
|
|
BMI |
–0.380* |
–0.185 |
–0.130 |
–0.306* |
–0.243 |
–0.179 |
|
|
ASIA level |
–0.408* |
–0.137 |
–0.299 |
–0.424* |
–0.031 |
–0.203 |
|
|
LE-MAS |
0.113 |
0.197 |
0.080 |
–0.081 |
–0.142 |
–0.006 |
|
|
FIM motor score |
–0.286 |
–0.270 |
–0.278 |
–0.298 |
–0.260 |
–0.227 |
|
|
WISCI-II |
–0.218 |
0.023 |
–0.223 |
–0.144 |
–0.027 |
–0.093 |
|
|
*Correlation is significant at 0.05 level. RLC: right lateral condyle; RIA: right intercondylar area; RMC: right medial condyle; LMC: left medial condyle; LIA: left intercondylar area; LLC: left lateral condyle.; BMI: body mass index; ASIA: American Spinal Injury Association; LE-MAS: Lower Extremity Modified Ashworth scale; FIM: Functional Independence Measurement; WISCI-II: Walking Index for Spinal Cord Injury. |
|||||||
DISCUSSION
Femoral cartilage thickness in patients with SCI was evaluated in comparison with healthy subjects. Overall, cartilage measurements were thicker at both intercondylar areas and were negatively correlated with duration of immobilization and severity of injury.
Recent advances in musculoskeletal ultrasonography have enabled quantitative assessment of articular cartilage thickness in different joints. In addition, due to its several advantages (i.e. being a quick, dynamic and cost-effective method), we used ultrasonography as the imaging method in our study.
According to our results, the femoral cartilage was thicker in bilateral intercondylar areas and in left-sided medial femoral condyle. In the relevant literature for different animal models, increased, decreased or unchanged thickness of the articular cartilage has been found with different immobilization positions or with different measurement areas (i.e. different cartilage plates or layers of the knee) (3, 11–14, 26, 27). O’Connor (11) examined knee cartilage in a rat model after unloading combined with non-rigid immobilization in flexion. After 4 weeks, they observed that cartilage thickness had increased by 15–22% at the anterior femoral and by 10% at the anterior tibial regions, with no changes on the posterior sites. In a recent study with a SCI rat model, cartilage thickness has been shown to be increased at unapposed regions and decreased at apposed regions of the flexed knee joint (27). Furthermore, previous studies have also indicated that the contact areas and stresses substantially changed during knee flexion with or without quadriceps contraction (28). Similarly, as patients with SCI spend a lot of time sitting in wheelchairs with their knees in flexion, loading of the knee joint may naturally change after the injury.
In normal knee joints, the maximum femoral cartilage thickness is reported to be located in the middle of the femoral trochlea (29, 30), where high contact pressures are known to act (31, 32). On the other hand, when the immobilization in SCI is taken into account, our aforementioned finding might seem to be controversial at first glance. However, since previous reports have mentioned additional mechanisms (e.g. sensory denervation) that may play a role in the dynamics of the cartilage milieu (33), we suggest that a biomechanical model alone is not sufficient to explain the whole scenario. Likewise, our findings of thicker cartilage values in patients with SCI (probably due to oedema) might be caused by immobilization and denervation. Moreover, loading and/or long-lasting denervation in the chronic period might cause cartilage degeneration and atrophy, which may explain our finding of negative correlation between cartilage thickness and duration of immobilization. On the other hand, since thicker cartilage values of these patients might not necessarily indicate better/healthier cartilage, our findings need to be evaluated further.
A possible limitation of this study is that we assessed cartilage thickness only, and not volume. However, it has also been shown that differences in cartilage volume may result primarily from a difference in joint size rather than cartilage thickness (34, 35).
We conclude that central portions of the femoral cartilage tend to be thicker and negatively correlated with disease duration and severity after SCI. Future studies, including histological evaluations, could elucidate whether such cartilage changes are favourable for the knee joints of SCI patients, which might be functional thereafter.
The authors declare no conflicts of interest.
REFERENCES

