Lise Kay, MD and Merete Bertelsen, PT
From the Danish Society of Polio and Accident Victims, Rødovre, Denmark
OBJECTIVE: To describe bladder symptoms among polio survivors and the inconvenience they cause.
DESIGN: A survey using the validated Danish Prostatic Symptom Score questionnaire concerning bladder symptoms.
SUBJECTS: A random age- and gender-stratified sample of polio survivors drawn from members of the Danish Society of Polio and Accident Victims.
METHODS: Eligible subjects were sent the questionnaire by post.
RESULTS: Of 453 eligible subjects 272 responded. Within 2 weeks 87.5% of respondents had experienced at least one bladder symptom, and 76.5% reported that they had been bothered by a bladder symptom. Out of the 12 symptoms in the questionnaire we found a significant gender difference, with straining and weak stream reported more often among men, and urge incontinence reported more often among women. Incontinence occurred significantly more often among women (73.3%) than among men (40.9%). Compared with a similar study of the background population, bladder symptoms overall occurred approximately twice as often among polio survivors.
CONCLUSION: The majority of polio survivors experience bladder symptoms, prevalences being approximately twice as high as in the background population. Furthermore, polio survivors to a much larger extent find their bladder symptoms bothersome. A successful rehabilitation programme should therefore also focus on these symptoms.
Key words: urinary bladder; lower urinary tract symptoms; incontinence; polio; rehabilitation; population study; quality of life; voiding.
J Rehabil Med 2013; 45: 560–564
Correspondence address: Lise Kay, Fjeldhammervej 8, DK-2610 Rodovre, Denmark. E-mail: lka@ptu.dk
Accepted Jan 17, 2013; Epub ahead of print May 17, 2013
Introduction
It is well-known that the polio epidemics of the mid-20th century left many young people with sequelae in the form of second neurone paresis and that, after rehabilitation and a stable period of muscle strength, these people once again experience muscle weakness, a condition known as post-polio syndrome (PPS) (1).
It is, however, less well-known, that reports from the time of the polio epidemics (2–5) also described that patients with acute polio had bladder symptoms. For example, Skinhøj (2) reported that 42 out of 199 surviving patients had disturbances of the bladder, Russell Taylor (3) reported that 8% of cases had urinary retention and 6% had incontinence, and Wright (4) reported that 20% of the children and 65% of the adults had urinary tract symptoms. From a theoretical view, these problems may return with the decline of function experienced by the polio patients in the long run. Furthermore, the acute polio and subsequent rehabilitation may have had an influence on upbringing, habits and physical ability/disability of the patient; factors that are also important in relation to the occurrence of bladder symptoms.
Bladder symptoms, especially incontinence, are known to have major influence on quality of life (6, 7); thus, it is of relevance to the rehabilitation of polio survivors to address their bladder symptoms.
The aim of this study was to describe bladder symptoms in a random population of polio patients in terms of prevalence, correlation to gender and age and to the inconvenience they cause.
Methods
A random sex- and age-stratified sample of 453 polio survivors was drawn up from a list of polio members of PTU (The Danish Society of Polio and Accident Victims). The age groups are shown in Table I. The aim was to draw 100 members from each age group, but because polio was almost eradicated from Denmark in the mid-1950s, we were able to find only 27 men and 26 women between the ages of 40 and 49 years, making the total sample 453 and not 500. A Danish Prostatic Symptom Score (DAN-PSS-1) questionnaire, a letter of introduction, and a prepaid return envelope were sent by standard post to all eligible subjects. After 1 month non-responders were sent a reminder.
The results were compared with those of a similar study of the normal Danish population (8).
Questionnaire
The DAN-PSS-1 questionnaire (9) comprises 12 questions related to symptoms occurring 2 weeks previous to the response. Questions 1–4 concern the voiding process (formerly known as “obstructive symptoms”), i.e. hesitancy, weak stream, incomplete emptying and straining. Questions 5–8 concern storage symptoms (formerly known as “irritative” symptoms), i.e. frequency, nocturia, urgency, and urge incontinence. The final 4 questions concern dysuria, dribbling, stress incontinence, and other incontinence.
Each symptom is described on a 4-ranked scale (0–3) in relation to frequency and in relation to the bother that it causes the subject. A score of zero refers to the absence of symptoms or inconvenience, while 3 refers to maximal frequency or inconvenience.
The questionnaire has been validated in terms of reliability, internal consistency, responsiveness, construct and content validity among male patients (10, 11) and repeatability among community dwelling men (12).
Statistics
Symptom prevalence (S) was calculated as the percentage of all the responders scoring more than zero among those answering the questionnaire. In a similar way, the prevalence of subjects who were bothered by a symptom among all the responders (B) was calculated. The prevalence of subjects who were bothered among those experiencing a symptom (B/S) was also calculated.
The prevalence of subjects with incontinence was calculated as the percentage of subjects scoring more than 0 on any of the 3 questions about incontinence (questions 8, 11 and 12).
A χ2 test was calculated using the SPSS 19 and used to describe differences in symptom prevalence in relation to gender. Confidence limits were used to determine significant differences between the polio population and the normal population. For all tests, the level of significance was set at 5%.
Results
Participation
The participation rate in relation to age and gender is shown in Table I. The overall participation rate was 60.0%, being 59.8% among men and 59.7% among women. The participation rate was significantly lower among the youngest (40–49 years old) compared with the 4 older groups (p = 0.003).
|
Table I. Distribution of age and gender in responders and the total eligible polio population |
||
|
Polio population, age range |
Men n/N |
Women n/N |
|
40–49 years |
9/29 |
6/26 |
|
50–59 years |
32/50 |
38/50 |
|
60–69 years |
35/50 |
36/50 |
|
70–79 years |
33/50 |
30/50 |
|
80–89 years |
28/50 |
25/50 |
|
Total |
137/229 |
135/226 |
|
n: number of responders; N: number of eligible subjects. |
||
Single symptoms
Single symptoms occurred with prevalences of between 13.0% and 76.5% (S), in the range 16.3–76.5% among men and 13.0–75.6% among women. The prevalence of being bothered by the different symptoms ranged between 26.0% and 66.4% (B) (26.3–67.7% among men and 24.1–68.6% among women).
Depending on the symptom, 61.7–96.6% of men and 58.3–91.2% of women were bothered by the symptom they experienced (B/S). These differences were not significant.
Overall, bladder symptoms occurred very frequently among both genders, as 87.5% (88.3% men, 86.7% women) experienced at least one symptom within 2 weeks (S), and 76.5% (74.5% men and 78.5% women) were bothered by at least one of the voiding symptoms (B). These gender differences were not significant. Among those experiencing at least one symptom 87.5% (B/S) reported that they were bothered (88.3% among men and 86.7% among women, with no significant difference among the genders).
Symptoms related to the voiding process (former obstructive symptoms)
Table II shows prevalences of the various symptoms related to the voiding process (questions 1–4).
|
Table II. Prevalence of voiding (obstructive) symptoms (questions 1–4) and the corresponding bother in a polio population with 95% confidence interval (CI) |
|||||||
|
Men |
Women |
||||||
|
Symptoma % (95% CI) |
Botherb % (95% CI) |
B/Sc % (95% CI) |
Symptoma % (95% CI) |
Botherb % (95% CI) |
B/Sc % (95% CI) |
||
|
Hesitancy |
33.3** (26–43) |
34.4** (18–34) |
65.9 (50–80) |
23.3** (17–32) |
24.4** (9–22) |
61.3 (42–78) |
|
|
Weak stream |
56.2*,** (47–65) |
46.3*,** (36–55) |
68.1 (56–79) |
29.7*,** (22–38) |
24.7* (16–35) |
58.3 (41–74) |
|
|
Incomplete emptying |
55.4** (46–64) |
52.3** (43–63) |
75.7 (64–85) |
53.4** (46–63) |
42.5** (33–53) |
67.2 (55–78) |
|
|
Straining |
36.4** (29–46) |
37** (27–48) |
61.7 (46–75) |
23.5 (17–32) |
25.6 (16–37) |
65.5 (46–82) |
|
|
Any of above |
70.1 (60–76) |
61.3 (51–68) |
76 (66–84) |
60.0 (49–66) |
65.9 (55–71) |
81.5 (71–89) |
|
|
*Significant gender difference (χ2 test). **Significant difference between 95% confidence interval between polio population and normal population. aPercentage of subjects experiencing a symptom among the total number of responders; bPercentage of subjects being bothered among the total number of responders; cB/S: percentage of subjects being bothered by the symptom among those experiencing the symptom. |
|||||||
As seen, single symptom prevalences (S) varied from 33.3% to 56.2% among men and from 23.3% to 53.4% among women, with incomplete emptying being the most frequent symptom. The symptoms occurred more often among men than among women, the differences being significant for weak stream (p = 0.000). The prevalences of being bothered (B) ranged from 34.4% to 52.3% among men and 24.4% to 42.5% among women. Men were significantly more bothered by weak stream than were women (p = 0.002).
More than half of the subjects who experienced a symptom were bothered by that symptom (B/S). No gender-related difference was found among those experiencing a symptom in relation to the bother it caused (B/S).
In relation to age groups, there was no difference in the prevalence of symptoms (S) of being bothered (B) and (B/S).
On the whole, 70.1% of the men and 60.0% of the women had experienced at least one voiding symptom (S), and 61.3% of the men and 65.9% of the women reported that they were bothered by a voiding symptom (B). Among those with voiding symptoms 76.0% of the men and 81.5% of the women were bothered (B/S). These gender differences were not significant (p = 0.380).
Symptoms related to storage function (former irritative symptoms)
Prevalences of storage symptoms (questions 5–8) are shown in Table III. The various storage symptoms (S) occurred with rather high prevalences, varying from 37.4% to 76.5% among men and from 59.2% to 75.6% among women, with urgency being the most prominent among both genders. A significant gender-related difference was found only for urge incontinence, which occurred more often among women (p = 0.000). The prevalences of being bothered by the different storage symptoms (B) ranged from 54.5% to 66.7% among men and 56.1% to 66.1% among women. There was no gender difference in being bothered by storage symptoms.
The majority of subjects who experienced storage symptoms were bothered by their symptoms (B/S), but no significant gender-related difference was found. Furthermore, prevalences of symptoms (S) or of being bothered by a symptom (B) and (B/S) did not reveal any significant differences in relation to age.
Overall, 83.1% of the men had experienced at least one storage symptom (S) and 65.0% were bothered by a storage symptom (B). The corresponding figures for women were 83.7% and 70.4%, respectively. These differences were non-significant. Among those with storage symptoms 77.0% were bothered by their symptoms (B/S), 80.5% among men and 73.5% among women.
|
Table III. Prevalence of storage (irritative) symptoms (questions 5–8) and the corresponding bother in a polio population with 95% confidence interval (CI) |
|||||||
|
Men |
Women |
||||||
|
Symptoma % (95% CI) |
Botherb % (95% CI) |
B/Sc % (95% CI) |
Symptoma % (95% CI) |
Botherb % (95% CI) |
B/Sc % (95% CI) |
||
|
Frequency |
55.9 (46–63) |
54.5** (45–64) |
78.3 (67–87) |
62.3** (53–71) |
56.1** (48–67) |
73.7 (62–83) |
|
|
Nocturia |
75.0** (68–83) |
59.5** (49–66) |
72.2 (63–81) |
71.2** (64–80) |
63.6** (53–71) |
77.4 (68–85) |
|
|
Urgency |
76.5** (68–83) |
66.7** (60–77) |
77.9 (68–86) |
75.6 (68–83) |
66.1** (56–74) |
82.4 (73–90) |
|
|
Urge incontinence |
37.4*,** (29–47) |
57.8** (47–68) |
95.9 (86–100) |
59.2*,** (50–68) |
63.6** (53–73) |
89.9 (80–96) |
|
|
Any of above |
83.1 (79–91) |
65.0 (55–71) |
73.5 (66–83) |
83.1 (79–91) |
70.4 (59–75) |
80.5 (74–89) |
|
|
*Significant gender difference (χ2 test). **Significant difference between 95% confidence interval between polio population and normal population. aPercentage of subjects experiencing a symptom among the total number of responders; bPercentage of subjects being bothered among the total number of responders; cB/S: percentage of subjects being bothered by the symptom among those experiencing the symptom. |
|||||||
Miscellaneous symptoms
Symptom prevalences (S) (questions 9–12) varied from 61.4% to 16.3% among men and from 63.8% to 13.0% among women. Prevalences are shown in Table IV. Compared with women, significantly more men experienced post-voiding dribbling (p = 0.010), whereas women significantly more often experienced stress incontinence (p = 0.000) compared with men. The prevalences of being bothered (B) by the single symptoms ranged from 26.6% to 64.3% among men and 25.4% to 68.6% among women. Men were significantly more bothered by dribbling (p = 0.006) and women were significantly more bothered by stress incontinence (p = 0.000).
|
Table IV. Prevalence of various urological symptoms (questions 9–12) and the corresponding bother in a polio population with 95% confidence interval (CI) |
|||||||
|
Men |
Women |
||||||
|
Symptoma % (95% CI) |
Botherb % (95% CI) |
B/Sc % (95% CI) |
Symptoma % (95% CI) |
Botherb % (95% CI) |
B/Sc % (95% CI) |
||
|
Dysuria |
16.7 (11–25) |
26.6** (17–38) |
81.8 (60–95) |
13.0 (8–20) |
25.4** (16–37) |
88.2 (64–99) |
|
|
Dribbling |
61.4*,** (53–71) |
64.3*,** (54–74) |
80.8 (70–89) |
39.8* (31–48) |
44.3*,** (34–55) |
77.1 (63–88) |
|
|
Stress incontinence |
22.1*,** (16–30) |
37.7*,** (27–49) |
96.6 (82–100) |
63.8* (53–71) |
68.6*,** (60–79) |
87.2 (78–94) |
|
|
Other incontinence |
16.3** (10–24) |
32.4** (22–45) |
90.5 (70–99) |
28.0** (20–35) |
41.3** (30–53) |
91.2 (76–98) |
|
|
Any of above |
64.7 (54–71) |
55.5 (46–63) |
85.2 (76–92) |
69.6 (64–80) |
63.7 (53–69) |
89.4 (81–95) |
|
|
*Significant gender difference (χ2 test). **Significant difference between 95% CI between polio population and normal population. aPercentage of subjects experiencing a symptom among the total number of responders; bPercentage of subjects being bothered among the total number of responders; cB/S: percentage of subjects being bothered by the symptom among those experiencing the symptom. |
|||||||
Among those reporting a symptom 81.8–96.6% of men and 77.1–91.2% of women were bothered by the symptom (B/S).
No difference in prevalence of problems related to miscellaneous symptoms between age groups.
Incontinence
Incontinence (symptoms scores > 0 in questions 8, 11 or 12) had occurred within 2 weeks among 40.9% of the men and 73.3% of the women. This difference was highly significant (p = 0.000). Of the subjects with incontinence, 94.5% of the men and 84.8% of the women were bothered by their incontinence (B/S). This difference was not significant. Comparing the different age groups no difference was found in relation to the prevalence of incontinence (S) or of being bothered by incontinence (B/S).
Discussion
The results of this study show that lower urinary tract symptoms occur frequently among polio survivors, and that they, to a large extent, are bothersome to those who experience them. It is noteworthy that 40.9% of the men and 73.3% of the women had experienced incontinence within the last 2 weeks, and that this incontinence very bothersome. Compared with reports from the acute polio attacks, where voiding symptoms in form of retention was the most prominent symptom, the most frequent symptoms among polio survivors today are storage symptoms with urgency and incontinence.
A study similar to ours has been carried out in a random sample of the general population in a Danish municipality (8). Compared with this study (Figs 1 and 2), we found that symptom prevalences among polio survivors were approximately twice as high as prevalences in the background population and that polio survivors, to a greater extent, were bothered by their bladder symptoms.
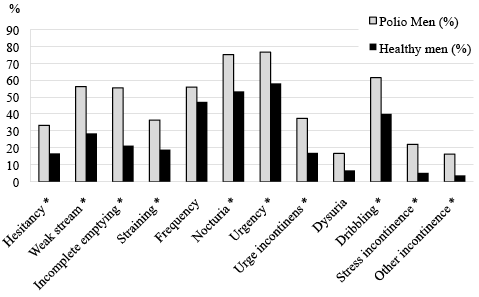
Fig. 1. Symptom prevalences among men with polio and men in the background population (8). *Significant difference between 95% confidential intervals.
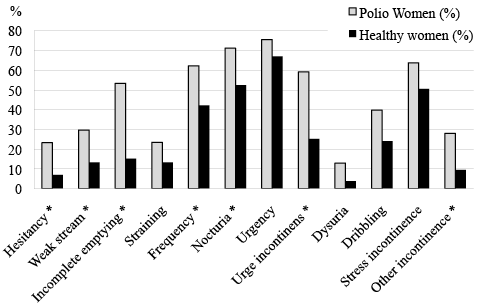
Fig. 2. Symptom prevalences among women with polio and women in the background population (8). *Significant difference between 95% confidential intervals.
In the community study women generally experienced more symptoms than did men, and were more bothered by their symptoms. This tendency is not pronounced among our polio survivors, which might indicate that bladder symptoms among polio survivors are distinct symptoms that derive from causes other than those found in the normal population.
Both studies found a preponderance of men reporting weak stream, and a preponderance of women reporting stress incontinence and other incontinence, suggesting that the causes of these symptoms may also be gender related.
The study of community dwelling Danes showed that weak stream, incomplete emptying, stress and urge incontinence increase with age among men, and that nocturia and mixed incontinence increased with age among both genders, but this was not the case in the polio population. A reason could be that the polio survivors acquire their symptoms at an earlier age than persons without polio; some may even have had symptoms ever since the acute polio infection.
Compared to the background population more polio patients reported that they were bothered by their bladder symptoms. In contrast to the population of polio survivors, in which many more reported that they were bothered by their bladder symptoms. This difference may appear either because polio survivors experience more severe symptoms and/or because their physical immobility may mean that they have more difficulty in compensating for the symptoms.
To our knowledge only one other study of bladder symptoms has been carried out among polio survivors (13). This study describes bladder symptoms among polio survivors with and without PPS. Compared with our study, symptom prevalences were found to be lower, but the respondents were younger (mean age 55 years) and the phrasing of the questions was different. The study by Johnson et al. (13) found no major gender-related differences in symptom prevalences, except that weak stream occurred significantly more often among men. In contrast to this we found significant gender differences in 6 out of the 12 bladder symptoms. In parallel with our findings, Johnson et al. (13) found a high prevalence of incontinence among polio survivors with or without PPS. In their study incontinence was reported by approximately half of the men and two-thirds of the women; but, in contrast to our study, this difference was not significant. As mentioned, their study did not include data from subjects without polio, but they found that polio survivors with PPS reported bladder symptoms more often compared with polio survivors without PPS. In line with the results of our study, this indicates that polio can cause bladder symptoms not only in the acute phase, but also later in life.
There may be several explanations for why bladder symptoms occur more frequently among polio survivors. In addition to primary nerve and muscle dysfunction caused by the acute polo virus infection, secondary causes are also possible. The upbringing of children with polio in hospital wards in the mid-20th century often meant a fixed schedule of access to the potty, teaching the children to suppress their need to void urine until the next ward round. This supported a habit of having an over-distended bladder, which in turn weakens the detrusor muscle. Physical difficulties in getting to the toilet may result in fewer toilet visits, which also tend to make the bladder overdistended and weaken the detrusor. Furthermore, as a consequence of physical disabilities, extra time may be needed, not only for moving to the toilet, but also for undressing, which in turn may mean that a polio survivor cannot withhold the desire to void for as long as it takes to get seated at the toilet.
Finally, it is also possible that bladder symptoms may be caused by other urological diseases, since it is known that polio patients in general have more co-morbidity than the average population (14–16).
Whatever the reason, the treatment of bladder symptoms among polio survivors does not differ from the usual treatment of bladder symptoms: the major points are to exclude that other diseases, such as infection or neoplasms, account for the symptoms, then take a full patient history, adjust habits and surroundings and, finally, refer to a urologist for a urodynamic study.
Validity of the study
The participation rate was 60%, which is an acceptable level and in line with most other surveys. Unfortunately we recruited significantly (p = 0.01) fewer participants in the young age group (40–49 years) and none of these participants were free of symptoms. This situation may constitute a selection bias in two ways. The reported prevalences are, to a lesser extent, influenced by the youngest age group, and symptom prevalences in the youngest group may be overestimated. These two biases influence our results in opposite ways.
The population for this study was persons who had signed up as polio members in the PTU. However, they may not be completely representative of all polio survivors, since they could be subjects who experience the greatest number of symptoms from late polio. On the other hand, compared with polio survivors presenting themselves to a rehabilitation centre, the symptoms may be underestimated.
The DAN-PSS questionnaire has been validated among men. If the female experience of bladder problems differs greatly from that of men, this validation may not necessarily account for women.
Conclusion
In conclusion, the results of this study show that the great majority of polio survivors experience bladder symptoms, prevalences being approximately twice as high compared with in the background population. Furthermore, polio survivors, to a much larger extent, find their bladder symptoms bothersome. A successful rehabilitation programme should therefore also focus on these symptoms and, if necessary, refer polio survivors to urological assessment and treatment.
References

