Pelagia Koufaki, PhD1, Thomas H. Mercer, PhD1, Keith P. George, PhD2 and James Nolan, MD3
From the 1School of Health Sciences, Rehabilitation Sciences, Queen Margaret University Edinburgh, Edinburgh, 2Research Institute for Sport and Exercise Sciences, Liverpool John Moores University, Liverpool and 3Department of Cardiology, University Hospital of North Staffordshire, Staffordshire, UK
OBJECTIVES: The health benefits of high-intensity interval training in cardiac rehabilitation warrant further research. We compared the effectiveness of low-volume high-intensity interval training vs continuous aerobic exercise training in chronic heart failure.
Design/Settings: Unblinded, two arm parallel design with random assignment to exercise interventions in out-patient hospital rehabilitation gym.
METHODS: Patients with signs of chronic heart failure and ejection fraction < 45%, (mean age: 59.1 years (standard deviation (SD) 8.6); 3 women) completed 6 months of exercise using continuous aerobic exercise training (n = 9) or high-intensity interval training (n = 8). Cardiorespiratory fitness was determined during cycle ergometry using respiratory gas exchange analysis. Functional capacity was assessed via sit-to-stand and gait speed. Quality of life was assessed using the MOS Short-Form 36 and Minnesota living with heart failure questionnaires. Cardiac autonomic regulation was assessed using Heart Rate Variability.
RESULTS: Analysis of Covariance revealed significant time effects but no group × time interactions for exercise and functional capacity outcomes. Peak oxygen uptake (VO2peak) improved by a mean of 14.9% (SD 16.3%) from baseline and by 22% (SD 28.3) at ventilatory threshold in both groups. Sit-to-stand (11.9 (SD 11%)) and gait speed (16.0 (SD 19%)) improved similarly in both groups. No changes in quality of life or heart rate variability were noted. Training adaptations in high-intensity interval training were achieved despite a significantly reduced time commitment and total work volume compared to continuous aerobic exercise training.
CONCLUSION: Low-volume high-intensity interval training is a feasible and well tolerated training modality in cardiac rehabilitation settings, but is not more effective than continuous aerobic exercise training.
Key words: exercise therapy; heart disease; gait; physical fitness; heart rate variability.
J Rehabil Med 2014; 46: 00–00
Guarantors address: Dr Pelagia Koufaki, School of Health Sciences, Rehabilitation Sciences, Queen Margaret University, Edinburgh, EH21 6UU, Scotland, UK. E-mail: Pkoufaki@qmu.ac.uk
Accepted Nov 25, 2013; Epub ahead of print 20 Jan, 2014

*Part of this work has been presented as an oral communication at 8th World Congress of Cardiac Rehabilitation and Secondary Prevention. Dublin 23–26th May, 2004.
INTRODUCTION
Current cardiac rehabilitation guidelines recommend between 1,000–2,000 kcal or 150–180 min per week of moderate intensity aerobic exercise (50–70% of peak oxygen uptake (VO2peak) for the delivery of health benefits (1, 2). Recent reports suggest that high-intensity interval training (HIT), eliciting an isocaloric work volume to continuous moderate intensity aerobic exercise (CAT), is feasible, safe, and probably more effective than CAT for the improvement of VO2peak in patients with cardio-metabolic disease (3, 4). In contrast, no systematic differences were identified between HIT and CAT for cardiometabolic outcomes of glucose and lipid metabolism, body weight or blood pressure (3, 4). The lack of an unequivocal evidence base for the benefits of HIT is such that it is not yet recommended in clinical practice.
Although no universal definition exists for HIT, it is understood to consist of short bouts of exercise exceeding 90% of VO2peak interspersed by recovery periods of no or very low intensity activity (< 40% of VO2peak) (3–11). The utility of lower volume HIT applications in rehabilitation settings (< 200–250 kcal/session) (11), which may offer the potential to deliver benefits in a more time efficient manner (5–7, 11) remains unclear. Initial evaluations of low-volume HIT in the form of walking and cycling, 5 times a week for 3 weeks, reported it to be safe and effective in delivering stronger exercise stimuli, in a group of hospitalised patients with chronic heart failure (CHF) (5–7). HIT elicited similar improvements in exercise capacity compared with CAT whilst also reducing exercise-related cardiac stress. However, the short duration and the high frequency delivery of this intervention limits its generalizability to more conventional out-patient rehabilitation.
Physical activities (PA) performed at higher intensity are associated with higher levels of fitness and enhanced vagal autonomic control, when compared to moderate intensity PA levels in healthy individuals (12). High-intensity exercise has also been reported to improve cardiac autonomic regulation in patients with coronary artery disease (CAD), with changes in VO2peak positively correlating with changes in heart rate variability (HRV) (13). This may indicate the potential of this more intense exercise stimulus to effectively elicit greater improvements in exercise tolerance and cardiac autonomic control in patients with CHF, both of which have been reported to be powerful predictors of morbidity, mortality and health related quality of life (HRQoL) (14, 15).
The benefits of exercise rehabilitation in the form of CAT in CHF are well established (15, 16). The current study therefore aimed to: (i) assess feasibility and tolerance of a low-volume HIT exercise protocol, delivered in an outpatient rehabilitation environment for people with CHF, and (ii) compare the relative effectiveness of low-volume HIT and conventional CAT interventions on indices of physical fitness, cardiac autonomic control, functional capacity and HRQoL. We hypothesised that, in comparison to CAT, HIT would elicit greater adaptations in the primary outcome variable (VO2peak), as well as in a range of secondary outcome variables.
METHODS
Design and randomisation
This was a pragmatic pilot feasibility study with a 2-arm parallel intervention design. Participants were randomly assigned (simple randomisation), to receive either 24 weeks of CAT or HIT. Participants were recruited on a continuous basis but completion of baseline assessments always preceded randomisation to an exercise group. All assessments were repeated after 12 and 24 weeks of training. Investigators were unblinded to group assignment. Fig. 1 provides details of patient flow through the study phases.
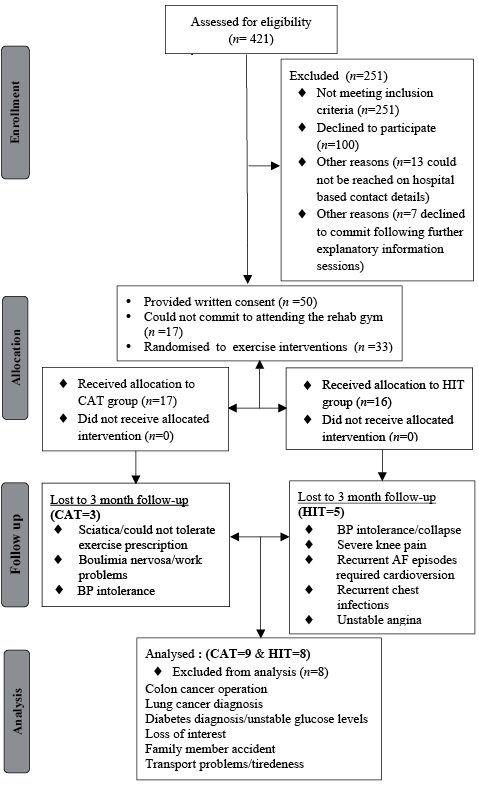
Fig. 1. Patient flow diagram. CAT: continuous aerobic exercise training; HIT: high-intensity interval training; AF: atrial fibrillation; BP: blood pressure.
Setting and participants
Recruitment followed distribution of invitation letters and public advertisement. Patients were considered for inclusion if they were adults over 18 years of age, had documented signs and symptoms of CHF with an ejection fraction (EF) < 45% and were in sinus rhythm. Exclusion criteria applied were diagnosis of diabetes, presence of pacemakers, major surgery or myocardial infarction within the previous 8 weeks.
The study was performed in accordance with the Helsinki declaration and was approved by the North Staffordshire Local Scientific Merit and Ethical Committees and by the local Research & Development office. All participants were informed about the procedures of testing and training and any risks associated with these. All participants provided written informed consent. All authors meet the criteria for authorship.
Outcomes assessments
Participants attended an outpatient rehabilitation gymnasium at North Staffordshire University Hospital, Newcastle-under-Lyme, UK on two separate occasions lasting about 2 h each, at baseline and after 3 and 6 months, to complete a range of assessments. The conduct of assessments was standardised in order to minimise any potential effects of assessment-related fatigue, with functional capacity tests preceding incremental exercise tests, interspersed by sufficient resting periods during which participants completed all HRQoL questionnaires.
Briefly, the assessments comprised:
i) Peak and sub-maximal exercise capacity (VO2peak and VO2 at ventilatory threshold (VT) during ramp incremental cycle ergometry (15 watts/min) using gas exchange measurements (K4B2 COSMED, Rome, Italy).VO2peak was defined as the highest value averaged over 30 s during the last stage of the incremental test and VT was determined using the V-slope method (2).
ii) Maximal short exercise capacity (MSEC) (maximum power output in watts) achieved during steep ramp cycle ergometry using 25 watt increments every 10 s as described by Meyer et al. (6).
iii) Cardiac autonomic function using HRV measures obtained from a continuous 3 channel ECG portable Holter device worn for 24 h (Tracker, Reynolds Medical Ltd, Hertfordshire, UK). The 24-h ambulatory ECG recordings were replayed and analysed using commercially available software, (Pathfinder, Reynolds Medical Ltd) in order to eliminate any random non-sinus rhythm beats, noise and artifacts as described by Nolan et al. (14). Only recordings with > 80% of total recording time suitable for analysis were used. Time and Frequency domain measures of HRV were calculated (Triangular Index of a 24 h recording (TI24), standard deviation of all normal to normal intervals (SDNN), total power (Tot P24), low frequency (LF), high frequency (HF) expressed in normalised units and corresponding ratios reflecting balance of sympathetic and parasympathetic system activity during day and night).
iv) Functional capacity/limitations were assessed via the Sit-to-Stand 5 (STS-5) and Sit-to-Stand 60 (STS-60) tests as proxy indices of muscular power and endurance and the North Staffordshire Royal Infirmary (NSRI) walk test (17), which consists of walking 50 m on flat ground, ascending and descending 22 steps and walking the same 50 m back, as fast as possible.
v) Health related quality of life via the Short-Form 36 (18) and the Minnesota Living with Heart Failure (MLWHF) questionnaires (19). The score for SF-36 can range from 0–100%, with a higher percentage indicating better total quality of life. The MLWHF score can range from 0–105 with higher scores indicating greater perception of severity and intrusiveness of heart failure related symptoms.
Exercise training interventions and management
Patients attended the rehabilitation gym for supervised exercise training, 3 times a week for 24 weeks (72 planned sessions). Patients in the CAT group cycled at an exercise intensity corresponding to 90% of their predetermined VT (corresponding to about 40–60% of VO2peak). Exercise stimulus progressed from 3 separate bouts of cycling of 7–10 min in duration, to a single 40 min of continuous cycling bout by 5–6 months.
Patients in the HIT group, performed 2 × 15 min bouts of cycling, comprising very low intensity active cycling phases of 1 min at 25–40 watts (equivalent to 20–30% of peak power output) followed by high intensity cycling for 30s at 50% of the maximum workload achieved during the MSEC test (equivalent to ~100% of peak power output during incremental exercise test), adhering to a work:recovery ratio of 1:2. Individualised patient exercise prescriptions were stored, for retrieval and implementation, on a programmable electronic cycle ergometer (Lode Corival, Groningen, The Netherlands).
For every training session, total cycling time, loaded cycling time (warm up, cool down and recovery periods excluded) and training workload (watts) were recorded, as well as Ratings of Perceived Exertion (RPE), HR and BP responses. Training RPEs, HRs and BPs were recorded at the mid-point and again at the end of the prescribed cycling sessions for each patient. Data included in the current analysis reflect the mean of 3 sessions within a single week at baseline, and after 12 and 24 weeks of training. Energy expenditure (EE) during training sessions was estimated using the American College of Sports Medicine’s metabolic calculation formula for leg cycling (VO2 = (10.8 × watts × body mass–1) + 7). The estimated training VO2 (L.min–1) was then converted into EE (kcal/min) by multiplying by 5 x total number of cycling minutes. At 3 months, exercise prescriptions were adjusted accordingly to reflect new tolerance/exercise capacity levels. All exercise sessions were supervised by an appropriately trained exercise physiologist and cardiac rehabilitation staff. An appropriately qualified clinical professional was always present during all incremental exercise tests.
Statistical analysis
Data are presented as mean (SD) or median (min–max) where appropriate. Sample size estimations were based on VO2peak as the primary outcome. For experimental power at 80% for an intended 0.5 effect size at a 0.05 significance level, 17 patients were needed to complete both arms of the study. Comparison of physical and clinical characteristics between patient groups at baseline, was performed using independent sample t-tests or non parametric equivalents. Mixed Model Factorial Analysis of Covariance with baseline VO2peak as a covariate was used to assess main effects of time and the interaction between modality of training and time. Where time effects were present, within group comparisons were performed using paired t-test if data were normally distributed or Wilcoxon signed rank tests if otherwise. In addition, we calculated bias corrected Hedge’s standardised effect sizes (ES) in order to establish the extent of pre-post HIT intervention difference (effect) in comparison to CAT (viewed as the standard reference point). This was accomplished using an on-line spreadsheet resource (20). To allow comparisons between groups with no pre test equivalence “adjusted” ESs were calculated by subtracting the pre-ES from the post-ES (21). All statistical analyses were performed using IBM statistics 19 for Windows.
RESULTS
Table I outlines the physical and clinical characteristics of the groups at baseline and indicates that no statistically significant differences existed at study entry. Aetiology of CHF included: idiopathic dilated cardiomyopathy, CAD and viral cardiomyopathy. Medications were optimised across the observation period. From the CAT group, one patient had bisoprolol increased at 3 months and warfarin at 6 months and one patient was taken off statins and had ramipril increased at 3 months. In the HIT group, one patient had bisoprolol reduced, one was taken off ramipril, one had bisoprolol increased, with another started on diuretics at 3 months. At 6 months, one patient was started on statins and one on warfarin. Seventeen patients completed all requirements of the study and remained in the final analysis. Patients who did not complete the study were physically weaker, reported worse social functioning and perceived greater severity of CHF related symptoms at baseline (p < 0.05) (Table II).
Table I. Physical and clinical characteristics of the exercise groups at baseline |
||
Variables |
CAT (n = 17) |
HIT (n = 16) |
Male/female, n |
13/4 |
14/2 |
Age, years, mean (SD) |
59.7 (10.8) |
59.8 (7.4) |
BMI, kg.m2 –1 mean (SD) |
29.5 (4.7) |
28.9 (4.7) |
NYHA, median (min–max) |
2.0 (1–3) |
2.0 (1–3) |
EF, %, mean (SD) |
35.2 (6.4) |
41.7 (10.3) |
VO2peak, ml.kg–1.min–1, mean (SD) |
15.5 (15.9) |
14.6 (4.8) |
SBP rest, mmHg–1, mean (SD) |
125 (15) |
114 (14) |
DBP rest, mmHg–1, mean (SD) |
73 (11) |
71 (10) |
Diuretics, n |
11 |
9 |
ACE inhibitors, n |
13 |
10 |
b-blockers, n |
10 |
11 |
Statins, n |
9 |
14 |
Ca channel blockers, n |
1 |
2 |
Nitrates & nitroglycerin, n |
6 |
6 |
VO2peak: peak oxygen uptake: CAT: continuous aerobic exercise training; HIT: high-intensity interval training; SD standard deviation; BMI: body mass index; NYHA: New York Heart Association Classification; EF: ejection fraction; SBP: systolic blood pressure; DBP: diastolic blood pressure; ACE: angiotensin converting enzyme inhibitors. |
||
Table II. Physical and clinical characteristics of people who completed and not completed the study |
||
Variables |
Completed (n = 17) |
Not completed (n = 16) |
Male/female, n |
14/3 |
13/3 |
Age, years, mean (SD) |
59.1 (8.6) |
60.5 (9.9) |
BMI, kg.m2 –1, mean (SD) |
29.2 (5.1) |
29.2 (4.3) |
NYHA, median (min–max) |
2 (1–3) |
3 (2–3) |
EF, %, mean (SD) |
38.4 (6.6) |
37.7 (13.4) |
VO2peak, ml.kg–1.min–1, mean (SD) |
16.5 (6.3) |
13.3 (3.5) |
SBP rest, mmHg–1, mean (SD) |
115 (6) |
124 (9) |
DBP rest, mmHg–1, mean (SD) |
70 (11) |
75 (11) |
MLWHFq total, mean (SD) |
24.6 (15.3) |
50.2 (25.3)a |
SF36-SF, mean (SD) |
77.2 (24.7) |
56.7 (32)a |
STS-5, s, mean (SD) |
8 (2.9) |
11 (4.7)a |
STS-60, mean (SD) |
34.4 (12.9) |
22.1 (13.4)a |
Peak Power Output, W, mean (SD) |
116.2 (34.9) |
91.3 (30.4)a |
aDifferent from completed p < 0.05. MLWHFq: Minnesota Living with Heart Failure questionnaire; SF36-SF: Short-Form-36-Social functioning component; STS-5: 5 Sit to Stand transfers; STS-60: Sit-to-Stand transfers in 60 s; VO2peak: peak oxygen uptake. |
||
Exercise training progression and tolerance
In comparison to HIT, patients in CAT, exercised for longer (p < 0.01, F = 35.2), at lower relative power outputs (p < 0.01, F = 20.5), but at similar levels of RPE and cardiovascular stress as indicated by calculated Rate Pressure Products (RPP = (SBP × HR)/1000) (Table III). Total EE per session was significantly lower in the HIT group (p < 0.01, F = 31.7) and significantly increased over time (p < 0.01, F = 108.9) (Table III).
Table III. Progression of exercise training prescription and associated training tolerance indices |
||||
CAT (n = 9) HIT (n = 8) |
Baseline |
12 weeks |
24 weeks |
|
MSEC, watts, mean (SD) |
CAT |
233.7 (47.5) |
250 (44.3) |
253.1 (36.4) |
HIT |
228.1 (60.4) |
244.3 (54.2) |
250 (61.2) |
|
Total cycling time, min, mean (SD) |
CAT |
26.8 (3.09) |
39.5 (1.4)b |
40 (0.0)a |
HIT |
30 (0.0) |
31 (1.052)b |
33.6 (1.21)a, b |
|
EE for total cycling time, kcal, mean (SD) |
CAT |
145.5 (39.3) |
234.9 (43.8)b |
260.8 (61.9)b |
HIT |
177.3 (39.3)a |
196 (30)a, b |
215.9 (33.4)b |
|
Loaded cycling time, min, mean (SD) |
CAT |
21.8 (3) |
34.5 (1.4)b |
36.2 (2.3)b |
HIT |
10 (0.0) |
10.3 (0.5)a, b |
11.4 (0.8)a, b |
|
EE for loaded cycling time, kcal, mean (SD) |
CAT |
123.5 (39.4) |
212.9 (43.8)b |
238.9 (62.3)b |
HIT |
85.9 (17.9)a |
100.4 (24.9)a, b |
114.4 (31.2)a, b |
|
Training Power Output, watts, mean (SD) |
CAT |
52.2 (24.6) |
62.5 (23)b |
70 (27.3)b |
HIT |
107 (36) |
126.6 (40.8)b |
137.5 (45.3)b |
|
Training Power Output, watts.kg–1, mean (SD) |
CAT |
0.69 (0.37) |
0.88 (0.42) |
1 (0.53) |
HIT |
1.26 (0.41)a, b |
1.47 (0.48)a, b |
1.58 (0.56)a, b |
|
Training RPP, bpm.mmHg–1, mean (SD) |
CAT |
13.2 (2.6) |
13.7 (3) |
13.6 (3.3) |
HIT |
10.9 (2.5) |
12 (3.2) |
12.6 (3.1) |
|
Training RPE, median (min-max) |
CAT |
13 (11,15) |
13 (12,15) |
12 (11–15) |
HIT |
11 (10,12) |
12 (11,12) |
11 (11,12) |
|
aDifferent from CAT p < 0.05; bdifferent from baseline p < 0.05. CAT: continuous aerobic exercise training; HIT: high-intensity interval training; MSEC: Maximum Short Exercise Capacity; EE: Energy Expenditure; RPP: Rate Pressure Product; RPE: BORG Rating of Perceived Exertion; SD: standard deviation. |
||||
During the observation period there was one episode of syncope during exercise (HIT) and one episode of what turned out to be an anxiety/panic attack (CAT). Two patients (CAT) although very keen to exercise, could not tolerate the exercise prescription due to severe orthopaedic pain. On several occasions, patients attended the exercise gym, but were not subsequently allowed to exercise due to presence of cardiac rhythm abnormalities (2 patients developed atrial fibrillation and had to be referred to a specialist for re-evaluation), BP instability with symptoms, resting angina episodes, abnormal glucose levels. A number of patients were diagnosed with additional medical conditions during the training period. Although, some of these patients continued to attend the gym sporadically, maintenance of their exercise prescription could not be achieved so these patients were excluded from the final analysis. Patients included in the final analysis had completed at least 65 out of the planned 72 sessions.
Peak and submaximal exercise capacity
Table IV summarises selected indices of exercise responses at peak effort and at VT level. Over time, both groups significantly improved peak exercise capacity and tolerance indices (Table IV, Fig. 2). CAT, but not HIT, significantly improved VO2 and power output at VT at 3 and 6 months compared to baseline. This was achieved at a similar level of cardiovascular stress as indicated by unchanged RPP (Table IV). No significant interaction effects (group × time) were observed for any of the assessed outcomes, indicating that both interventions had similar impact on reported outcomes (Table IV and Fig. 2). Standardised ESs, adjusted for small sample sizes and for inequalities at baseline (Hedges bias corrected) indicate that the standardised difference in all assessment outcomes between the 2 groups, was always less than half a SD of the pooled SD.
Table IV. Exercise capacity indices following 3 and 6 months of exercise training. Continuous aerobic exercise training (CAT) is assumed to be the standard cardiac rehabilitation reference point for the purposes of effect sizes (ES) calculations |
|||||||
CAT (n = 9) HIT (n = 8) |
Baseline Mean (SD) |
12 weeks Mean (SD) |
24 weeks Mean (SD) |
ES-pre (95% CI) |
ES-post (95% CI) |
Adjusted ES (95% CI) |
|
VO2peak, ml.min–1.kg–1 |
CAT |
17.6 (7.1) |
19.8 (7.8)a |
18.9 (7.5) |
–0.36 (–1.32 to 0.6) |
–0.18 (–1.13 to 0.78) |
0.18 |
HIT |
15.3 (4.7) |
17.3 (5.4)a |
17.7 (4.9)a |
||||
Power output, watts |
CAT |
121.1 (31.2) |
131.6 (37.5a |
129.1 (32.3) |
–0.28 (–1.24 to 0.68) |
0.12 (–0.83 to 1.07) |
0.4 |
HIT |
110.6 (40) |
131.2 (32)a |
133.7 (40.5)a |
||||
RER |
CAT |
1.27 (0.13) |
1.16 (0.07)a |
1.25 (0.14) |
–1.14 (–2.16 to 0.11) |
–1.01 (–2.02 to 0.00) |
0.13 |
HIT |
1.13 (0.1) |
1.12 (0.04) |
1.13 (0.07) |
||||
Peak RPP, mmHg.beats–1 |
CAT |
19.3 (6.5) |
18.9 (6.6) |
20.3 (5.2) |
–0.24 (–1.20 to 0.71) |
–0.13 (–1.09 to 0.82) |
0.11 |
HIT |
17.5 (7.5) |
19.5 (6.8) |
19.5 (6.3) |
||||
O2-pulse, ml.beat–1 |
CAT |
11.5 (3.3) |
13.1 (4.02) |
12.33 (3.44) |
–0.03 (–0.98 to 0.92) |
0.22 (–0.73 to 1.18) |
0.25 |
HIT |
11.4 (2.8) |
13.08 (3.21) |
13.03 (2.40) |
||||
VO2-VT, ml.min–1.kg–1 |
CAT |
10.8 (3.1) |
13.4 (4.2)a |
13.5 (5.4)a |
–0.10 (–1.06 to 0.85) |
–0.35 (–1.31 to 0.61) |
0.25 |
HIT |
10.4 (4.3) |
11.4 (2.8) |
11.9 (2.6) |
||||
Power output-VT , watts |
CAT |
58.8 (21.4) |
77.7 (17.5)a |
76.3 (29.6)a |
0.16 (–0.8 to 1.11) |
0.06 (–0.89 to 1.01) |
0.1 |
HIT |
63.7 (36.6) |
76.8 (24.3) |
78.1 (24.9) |
||||
RER-VT |
CAT |
1 (0.13) |
0.91 (0.04)a |
0.97 (0.09) |
–0.48 (–1.45 to 0.49) |
–0.05 (–1.01 to 0.90) |
0.43 |
HIT |
0.95 (0.04) |
0.90 (0.05) |
0.92 (1.3) |
||||
RPP -VT, mmHg.beats–1 |
CAT |
12.3 (3.9) |
12.6 (3.7) |
13.7 (4.7) |
0.10 (–0.85 to 1.05) |
–0.26 (–1.22 to 0.70) |
0.36 |
HIT |
12.7 (3.7) |
12 (2.8) |
12.6 (3) |
||||
O2-pulse-VT, ml.beat–1 |
CAT |
9.03 (2.4) |
11.3 (2.9)a |
10.8 (3.2)a |
0.34 (–0.78 to 1.13) |
0.17 (–0.78 to 1.13) |
0.17 |
HIT |
9.9 (2.4) |
10.9 (2.3) |
11.3 (2.1) |
||||
aDifferent from baseline p < 0.05. CAT: continuous aerobic exercise training; HIT: high-intensity interval training; RER: Respiratory Exchange Ratio; VT: ventilatory threshold; RPP: Rate Pressure Product; VO2peak: peak oxygen intake: 95% CI: 95% confidence interval: SD: standard deviation. |
|||||||
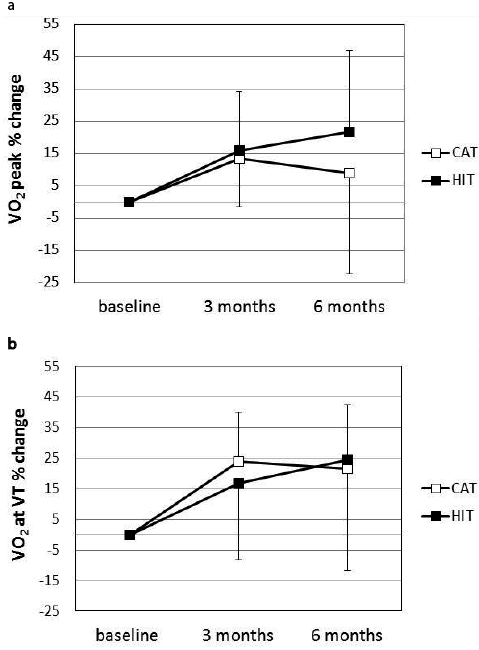
Fig. 2. Group mean percentage changes in peak oxygen intake (VO2peak) (a) and VO2 at the ventilatory threshold (VT) (b), following 3 and 6 months of continuous aerobic exercise training (CAT) and high-intensity interval training (HIT) exercise rehabilitation.
Cardiac autonomic function
Time and frequency domain HRV indices remained unchanged at follow up assessment points. No significant time or group × time interactions were detected (Table V).
Table V. Time and frequency domain heart rate variability (HRV) indices |
||||||
Variables |
CAT (n = 9) |
HIT (n = 8) |
||||
Baseline Mean (SD) |
12 weeks Mean (SD) |
24 weeks Mean (SD) |
Baseline Mean (SD) |
12 weeks Mean (SD) |
24 weeks Mean (SD) |
|
Analysable recording (%) |
97 (3.21) |
96 (4.39) |
95.7 (3.41) |
96.85 (4.84) |
96.42 (5.15) |
95.1 (5.98) |
TI24 |
35.3 (13.3) |
35.2 (16.5) |
38.14 (19.8) |
31.5 (8.2) |
28.1 (5.8) |
33.4 (9) |
SDNN, ms |
131 (49) |
128 (53) |
130.7 (53.6) |
112 (22) |
101 (23) |
117.4 (37.4) |
Tot P24, ms2 |
2,188 (1,692) |
2,247 (1,494) |
2,811.87 (3,268) |
3,342 (3,600) |
2,669 (3,006) |
1,757.14 (929.56) |
LF/HF day |
2.9 (1.8) |
2.9 (2.2) |
4.17 (3.7) |
3.2 (3.1) |
2.5 (2) |
4.48 (3.07) |
LF/HF night |
3.3 (2.6) |
2.4 (1.1) |
2.06 (1.08) |
3 (3.2) |
2.8 (3.2) |
3.10 (3.97) |
CAT: continuous aerobic exercise training; HIT: high-intensity interval training; TI24: Triangular Index over a 24-h period; SDNN: standard deviation of all normal to normal beat intervals; TotP24: total power; LF/HF: low-frequency/high-frequency ratio. |
||||||
Functional capacity and health related quality of life
Self reported NYHA symptom classification improved over time in the CAT group. Objectively-measured functional capacity improved over time in both groups (Table VI). Indices of HRQoL remained unchanged at follow-up assessment points. None of the 8 subcomponents that make up the total score for the SF-36 questionnaire (physical function, role physical, general health, mental health, social functioning, vitality, bodily pain, role emotional) and for the MLWHF questionnaire (physical and emotional sub-scores) were significantly modified over time (data not shown). No significant group × time interactions were detected (Table VI). The calculated standardised ESs indicate that our interventions differed by less than half a SD of the pooled SD for all outcomes.
Table VI. Objective and self report functional capacity and quality of life following 3 and 6 months of exercise training |
|||||||
CAT (n = 9) HIT (n = 8) |
Baseline |
12 weeks |
24 weeks |
ES-pre (95% CI) |
ES-post (95% CI) |
Adjusted ES (95% CI) |
|
NYHA class |
CAT |
2 (1–3) |
2 (1–2)a |
2 (1–2)a |
0.00 (–0.95 to 0.95) |
0.42 (–0.55 to 1.38) |
0.42 |
HIT |
2 (1–3) |
2 (1–2) |
2 (1–2) |
||||
STS-60 |
CAT |
37 (14.4) |
41.1 (16.4)a |
40.7 (15.1)a |
–0.40 (–1.37 to 0.56) |
–0.24 (–1.20 to 0.71) |
0.16 |
HIT |
31.5 (11) |
35.7 (13.3) |
37.3 (11)a |
||||
STS-5, s |
CAT |
7.5 (2.1) |
6.3 (1.6)a |
6.6 (2.1)a |
0.39 (–0.57 to 1.35) |
0.13 (–0.82 to 1.08) |
0.26 |
HIT |
8.7 (3.6) |
7.8 (2.5) |
6.9 (2.3)a |
||||
NSRI total, s |
CAT |
83.9 (18.6) |
73.8 (17.1)a |
71.4 (16.1)a |
0.51 (–0.45 to 1.48) |
0.75 (–0.23 to 1.74) |
0.24 |
HIT |
101.4 (43) |
90.5 (25.3) |
87.8 (24.8)a |
||||
Gait speed, m.s–1 |
CAT |
1.33 (0.32) |
1.53 (0.43)a |
1.56 (0.38)a |
–0.42 (–1.38 to 0.54) |
–0.77 (–1.76 to 0.22) |
0.35 |
HIT |
1.18 (0.36) |
1.24 (0.29) |
1.28 (0.30)a |
||||
MLWHFq total |
CAT |
22.8 (12.9) |
24.6 (20.3) |
37 (24) |
0.23 (–0.73 to 1.19) |
–0.17 (–1.12 to 0.79) |
0.40 |
HIT |
26.6 (18.3) |
29.1 (15.7) |
33.3 (17.6) |
||||
SF36-total |
CAT |
67 (20.2) |
71.8 (19.1) |
62.7 (24.8) |
–0.31 (–1.27 to 0.65) |
–0.28 (–1.24 to 0.68) |
0.03 |
HIT |
59.8 (24.1) |
59.7 (18.9) |
56.3 (17.1) |
||||
aDifferent from baseline p < 0.05. CAT: continuous aerobic exercise training; HIT: high-intensity interval training; NYHA: New York Heart Association classification; STS-60: Sit-to-Stand transfers in 60 s; STS-5: time for 5 Sit-to-Stand transfers; NSRI: North Staffordshire Royal Infirmary; MLWHFQ: Minnesota Living with Heart Failure Questionnaire; SF36-total: Short-Form 36 Health Survey total score; 95% CI: 95% confidence interval. |
|||||||
DISCUSSION
Our study contributes to the extremely limited knowledge base for the potential use of low-volume HIT in the clinical rehabilitation of patients with CHF. Our findings indicate that: i) low-volume HIT cycling is feasible and well tolerated by patients with CHF, ii) HIT elicited a broadly similar degree of improvement in physical function as CAT, despite a significantly lower total training volume and exercise time commitment, that were accompanied by similar levels of perceived effort and cardiovascular stress, iii) neither intervention was effective in favourably modifying cardiac autonomic function nor in favourably modifying HRQoL.
Based on adjustment for baseline inequalities ESs, we consistently observed less than half a SD difference between the means of the 2 groups, for all exercise capacity indices, at the end of the follow up period. Group mean VO2peak improved by 13% (SD 18.3%) and by 8.9% (SD 25.3%) from baseline, after 3 and 6 months in the CAT group. In comparison, the HIT group demonstrated a 15% (SD 15%) and 21.6% (SD 31.2%) improvement after 3 and 6 months, respectively. This level of improvement is in agreement with improvements ranging from 8 to 16% for CAT and ~18% for HIT, reported in other studies comparing HIT vs CAT (22, 23). In contrast, Wilsøff et al. (8) and Tjønna et al. (24) reported increases in VO2peak of 35–46%, corresponding to a gain of 4–6 ml/kg/min in VO2peak following HIT, even though their HIT protocols were very similar to ones used in other studies reporting much less marked improvements (22, 23, 25, 26). A meta-analysis of exercise rehabilitation trials in people with CHF (16) concluded that on average, a 2.16 ml/kg/min increase in VO2peak is commonly observed. A meta-analysis on the efficacy of HIT applications in people with CV disease (3), reported that VO2peak was improved by at least 3.6 ml/kg/min. Myers et al. (27) observed that an increase in VO2peak by an equivalent amount (1 MET) is associated with 9% reduction in mortality over a year in people with CV conditions. In the context of these clinically important evaluation criteria, although both our interventions met the minimum expected mean improvement (Table IV) they fell short of reaching the 1 MET level of improvement. A closer examination of individual responses and group trends (Table IV, Fig 2a), seem to suggest that HIT was associated with a continuous fashion of improvement for VO2peak, whereas CAT improvements seemed to have levelled off after 36 training sessions (Fig 2a). It is possible that the significantly higher relative workload prescribed during HIT training (see Table III), can improve tolerance of higher power outputs which in turn could sustain/enhance VO2peak gains.
Conversely, if one considers the time pattern of adaptations at moderate levels of physiological demand (VT and functional capacity, Tables IV and VI), CAT seemed to produce faster adaptations, even though the overall adjusted ESs suggest no substantial difference between the groups at the end of the observation period. Improvements at this level reflect an enhanced cardiovascular/metabolic efficiency in sustaining higher levels of energy demands. It is possible that the greater total volume of exercise achieved by CAT at 3 months (Table III), was the main driver for the faster adaptations at VT level. Time effects of CAT on O2-pulse (Table IV), that may suggest underlying improvements in stroke volume and/or O2 extraction ability, could partially explain these adaptations, especially in the absence of any substantial changes in HR and SBP (RPP-VT) (28). Our results partially disagree with two studies (8, 29), that have reported greater improvements in VO2 at VT in patients with CAD and CHF who followed HIT training (32% and 41%, respectively) compared to patients in CAT (9.5 and 26.2% increases). The interventions in the aforementioned studies were designed to be isocaloric with an estimated (from information available in the literature) EE/week for the HIT prescription (walking at 80–90% VO2peak) of ~1,002 kcal vs 942 kcal for the CAT (50–60% VO2peak) programme. In contrast, our training regimens were not designed to be isocaloric, so our HIT prescription, elicited a significantly lower volume of exercise compared to CAT (Table III). Our weekly cycling EE progressed from 436 kcal/week at baseline to 704.7 kcal/week by 12 weeks for CAT vs 531 to 588 kcal/week for HIT, inducing statistically similar increases in VO2-VT (CAT: 23.9% vs HIT:16.8%) (Fig. 2). These observations may indicate that there is a critical threshold of total volume of work (EE) that needs to be achieved before training stimuli become optimally effective in modifying metabolic and CV efficiency at moderate levels of exercise. In all other studies that have used similar isocaloric HIT and CAT training protocols (8, 9, 13, 22–26), achievement of higher EE was perhaps easier, as the exercise prescriptions combined high (80–95% VO2peak or HR max) and moderate intensity (60–70% of HR max or VO2peak) longer exercise phases (2–4 min) of weight bearing physical activities. It may be unrealistic to expect this level of EE, during cycling in particular, in typical cardiac rehabilitation programmes. Nevertheless, our lower volume HIT protocol was not worse than CAT in eliciting favourable adaptations.
To our knowledge, only one other study that has examined the effectiveness of a HIT protocol vs usual care in people with CHF, has reported functional capacity outcomes (9). Functional capacity outcomes are important, as they can represent outcomes more meaningful to patients and can ultimately translate into enhanced physical independence and QoL. Nilsson et al. (9) reported that a high-intensity dance circuit programme significantly improved distance walked over 6 min, by 58 m. In our study, gait speed improved in both groups by about 18.3% (SD 14) in CAT and by 13.4% (SD 24) in HIT, despite the mode of training being cycling. We also observed significant improvements over time in both groups, for tasks primarily reflecting leg muscular power and fatigue tolerance (STS-5: CAT: 11 (SD 10%) vs HIT: 18 (SD 8.6%) and STS-60: CAT:11 (SD 12%) vs HIT: 26 (SD 37.7%). Our results are encouraging as they indicate that whole body integrated physiological adaptations translated into similar levels of improvement in the ability to perform common activities of daily living. In contrast, our patients’ perception of overall QoL did not substantially change in any group (Table VI). Surprisingly, the improvements noted in objectively measured functional capacity were not reflected in the relevant physical function sub-components of the questionnaires used (data not shown). In the study by Nilsson et al. (9), the significant improvement in walking capacity was accompanied by significant improvements in the MLWHF score in the exercise group. However, the exercise group started from a significantly higher baseline value (30) compared to the usual care group (23) and thus at the end both groups had very similar scores. Recent meta-analyses have suggested that QoL changes in patients with CHF, do not always parallel changes in physical function outcomes following exercise rehabilitation, with small or no changes reported for a variety of HRQoL measures (15, 16). Our patients had baseline scores similar to those reported elsewhere (9, 31, 32) using the same assessment outcome and thus our data are within the expected range.
Reduced HRV is considered a significant prognostic indicator of mortality in CHF (14). Aerobic exercise training of moderate intensity has been shown to have sympathoinhibitory effects in addition to pharmacotherapy (30, 32–38). Resistance based exercise training has also been reported to produce some favourable modification in indices of exercise performance but with no associated modulation of autonomic function (30, 34). Our results indicate that none of our exercise stimuli were effective in altering cardiac autonomic regulation. Data from our patients indicate an increased level of sympathetic activation that persisted even at times during which a predominance of parasympathetic modulation would be expected (39) (see Table VI, LF/HF night vs LF/HF day). It is also worth noting a declining trend in total P24, in the HIT group, which is an index of total amount of variability in the regulation of HR over a 24-h period (39). These observations may reflect worsening of underlying medical conditions and the general health status over time, as many patients experienced several health challenges that resulted in substantial pauses of the exercise training programme on occasions. It is also possible that the overall volume of work was not sufficient to provoke changes to, or override the medication effects on, these indices of cardiac autonomic regulation. Meyer et al. (5), whose training protocol we have reproduced here, observed no changes in resting epinephrine and norepinephrine levels following a 3 week training period in patients with CAD. On the other hand, Munk et al. (13) observed significant improvements in HRV indices in patients with CAD, following a 6 month high volume HIT training (> 900 kcal/week). Future studies should aim to evaluate different volumes of HIT training to establish a threshold of consistent effect on HRV outcomes in CHF.
Study limitations
One could argue that a greater number of participants were required to increase confidence in the observations made. Although the low completion numbers were disappointing, they reflected the high comorbidity burden of these patients that ultimately precipitated withdrawal from the study or delayed progression and adherence to the exercise protocols. In cases of pauses > 2 weeks in the training plan, we compensated by offering more training sessions, so that every patient had accumulated at least 85% of planned sessions. These drawbacks may of course have diluted the magnitude of potential improvements. Moreover, due to funding limitations, travel reimbursement and blinding of the investigators to the interventions and assessments was not possible. Unblinded outcome assessment can potentially introduce bias in the reported data, although every effort was made to collect and analyse the data as objectively as possible. We feel however, that our investigative approach was acceptable, given that this was a pragmatic feasibility study and these are common experiences and occurrences within such patient groups in real-life clinical rehabilitation settings.
In conclusion, our study shows favourable training adaptations in people with CHF following low-volume HIT training. Compared to CAT exercise and functional capacity adaptations were achieved against a background of significantly reduced training time and total volume of work, with similar levels of perceived exertion and haemodynamic stress. These are important observations that may allay some of the concerns regarding the use of HIT for people with pathophysiologically reduced exercise tolerance. Moreover, the potential value of our HIT approach may be in its utility for severely deconditioned and cachectic CHF patients where improvements in physical function are desired in the context of energy preservation and time efficiency.
Acknowledgements
This work was funded, in part, by a research grant from West Midlands R&D (LORS), UK with registration number 895WRD/38/032. We would also like to thank Ms Julie Machin and Ms Angela Mason, research and heart failure nurses, for their invaluable assistance with patient liaison, recruitment, exercise supervison and overall patient care.
The study was conducted at North Staffordshire University Hospital, Department of Cardiology in collaboration with the Department of Exercise and Sport Science, Manchester Metropolitan University.
REFERENCES
1. Piepoli MF, Corrá U, Benzer W, Bjarnason-Wehrens B, Dendale P, Gaita D, et al. Secondary prevention through cardiac rehabilitation: from knowledge to implementation. A position paper from the cardiac rehabilitation section of the European association of cardiovascular prevention and rehabilitation. Eur J Cardiov Prev Rehab 2010; 17: 1–17.
