Melissa Selb, MSc1,2, Friedbert Kohler, MD3,4, Molly Meri Robinson Nicol, DC5, Marcelo Riberto, MD, PhD6, Gerold Stucki, MD, MS1,2,7, Cille Kennedy, PhD8 and Bedirhan Üstün, MD5
From the 1ICF Research Branch in cooperation with the WHO Collaborating Centre for the Family of International Classifications in Germany (at DIMDI), 2Swiss Paraplegic Research, Nottwil, Switzerland, 3Braeside Hospital, Wetherill Park, 4School of Public Health and Community Medicine, Faculty of Medicine, University of NSW, Sydney, Australia, 5World Health Organization, Classification, Terminology and Standards, Geneva, Switzerland, 6University of São Paulo, Ribeirão Medical School, São Paulo, Brazil, 7Department of Health Sciences and Health Policy, University of Lucerne, and at SPF, Nottwil, Switerzland and 8Office of the Assistant Secretary for Planning and Evaluation, US Department of Health and Human Services, Washington, USA
BACKGROUND: This is a follow-up of the special report Towards the joint use of ICD and ICF: A call for contribution, published by the Journal of Rehabilitation Medicine in 2012, which introduced an initiative of using the International Classification of Diseases (ICD) and the International Classification of Functioning, Disability and Health (ICF) in a complementary way in clinical practice. Recognizing the merits of using the ICD and ICF jointly, the World Health Organization (WHO) introduced so-called functioning properties in the ICD-11. The first step in this ICD-ICF joint use initiative revealed 103 rehabilitation-relevant health conditions for which functioning properties were to be identified. Afterwards experts were recruited to identify the functioning properties for the health conditions for which no ICF Core Sets were available and all the functioning properties were integrated in the beta-version of ICD-11.
OBJECTIVE: The objective of this special report is to present the outcome of the recruitment and training of the contributing experts, and to provide an update on the current status of identifying functioning properties and their integration in ICD-11.
Discussion: Having functioning properties in the ICD-11 achieves a milestone in depicting health information in an integrated and comprehensive manner. Explicitly identifying functioning properties for specific health conditions further reinforces the importance of acquiring a broader and more meaningful picture of a person’s health, and can guide clinical decision-making.
Key words: International Classification of Diseases; ICF; classification; functioning; ICD revision; rehabilitation.
J Rehabil Med 2015; 47: 2–8
Correspondence address: Melissa Selb, Coordinator of the ICF Research Branch, c/o Swiss Paraplegic Research, Guido-Zäch-Strasse 4, CH-6207 Nottwil, Switzerland. E-mail: melissa.selb@paraplegie.ch
Accepted Feb 7, 2014; Epub ahead of print Nov 24, 2014
INTRODUCTION
In the 2012 special report Towards the joint use of ICD and ICF: A call for contribution (1) and in the paper by Escorpizo et al. (2) on the importance and methods of linking disease and functioning, the authors encouraged the complementary use of the International Classification of Diseases (ICD) (3) and the International Classification of Functioning, Disability and Health (ICF) (4), both World Health Organization (WHO) classifications, in clinical practice. Recognizing the merits of jointly using ICD and ICF, WHO introduced so-called functioning properties (FP) in the 11th revision of the ICD (ICD-11) (5, 6). FP are ICF categories in the component of activities and participation (A&P) that are identified as being the most relevant for more fully describing the impact of a health condition on a person’s functioning for a particular health condition (1, 2).
To tackle the challenge of identifying or “populating” FPs for the thousands of health conditions in ICD-11 (5) WHO decided to start out with a selection of the most frequent health conditions encountered in rehabilitation, and called for contributors from the broad rehabilitation community. In line with the collaboration plan between the International Society of Physical and Rehabilitation Medicine (ISPRM) and WHO (7), ISPRM responded to the call. ISPRM’s response reflects its long-standing endeavour to facilitate the implementation of the ICF in rehabilitation practice. Together with WHO, and supported by the ICF Research Branch, a cooperation partner of the WHO Collaborating Centre of the WHO Family of International Classifications (WHO-FIC) in Germany, ISPRM commenced the ICD-ICF joint use initiative (name given to the task of populating FPs) with a workshop in February 2012, during which an international and multi-professional group of participants identified 103 rehabilitation-relevant health conditions for which FPs would be populated. To complete the task of populating FPs, experts who would be responsible for each of the 103 health conditions, had to be recruited and trained on the methodology for populating the FPs. This step turned out to be a challenge in itself.
The objective of this special report is to present the outcome of the recruitment and training of rehabilitation experts, and to provide an update on the current status of populating FPs and their integration in ICD-11.
METHODS
Recruitment of experts
The multimodal approach to recruiting rehabilitation experts of varying disciplines started with the 2012 paper calling for contributions (1). This paper listed the 103 health conditions (3) for which FPs were to be identified. Since it was decided that these health conditions should be populated with the categories of the respective ICF Core Set, if available, experts were recruited only for those health conditions for which no Brief ICF Core Sets exist (1). A Brief ICF Core Set (8) is the shortest selection of ICF categories that are considered the most relevant for describing the functioning of a person with a specific health condition. While an ICF Core Set spans across all the components of the ICF, i.e. body functions and structures, A&P and environmental factors (4), FPs considers only the A&P categories of the respective Brief ICF Core Set.
In addition to the aforementioned paper calling for contribution, the ICD-ICF joint use initiative was introduced at various international and national scientific and professional society meetings, e.g. WHO-FIC Annual Meetings in 2012 and 2013, March 2012 American Academy of Orthotists and Prosthetists meeting, May 2012 Asia-Oceanian Conference of Physical and Rehabilitation Medicine, March 2013 annual meeting of the Physical and Rehabilitation Medicine Section of the European Union of Medical Specialists, and June 2013 ISPRM World Congress, personal invitations to identified experts to contribute, as well as “word of mouth” within the rehabilitation and scientific communities.
Populating functioning properties
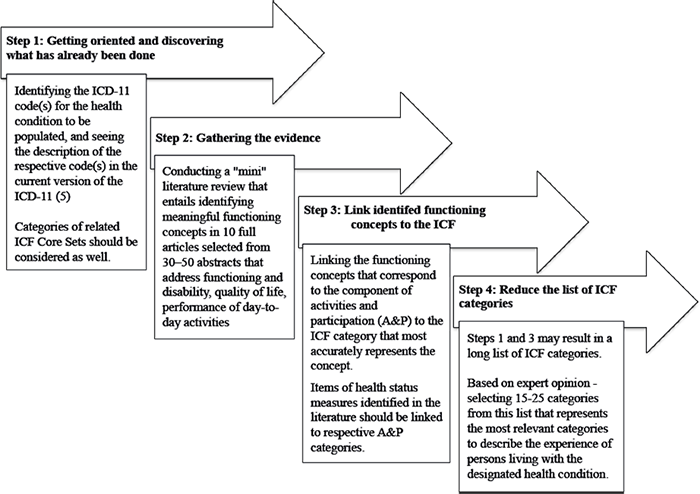
Experts who agreed to contribute to the initiative were provided with a guidance document and invited to participate in a live online tutorial (9) that detailed the content of the guidance document. The guidance document (http://www.ncbi.nlm.nih.gov/pubmed/?term=Selb+2012+Kohler) outlines the procedure for populating the FPs. Fig. 1 depicts the step-by-step instructions outlined in the guidance document. The 4-step procedure comprises: (i) becoming familiar with the ICD-11 description of the chosen health condition and categories of associated ICF Core Sets; (ii) conducting a literature review to identify functioning concepts; (iii) linking these concepts to the respective A&P categories that most reflects its meaning using established linking rules (10); and (iv) deciding on a selection of 15–25 categories that captures the experience of a person living with the health condition based the rehabilitation expert’s clinical know-how. If the literature review in step 2 reveals health status measures that are commonly used in assessments of persons living with the respective health condition, the items of the measure would also have to be linked to the ICF.
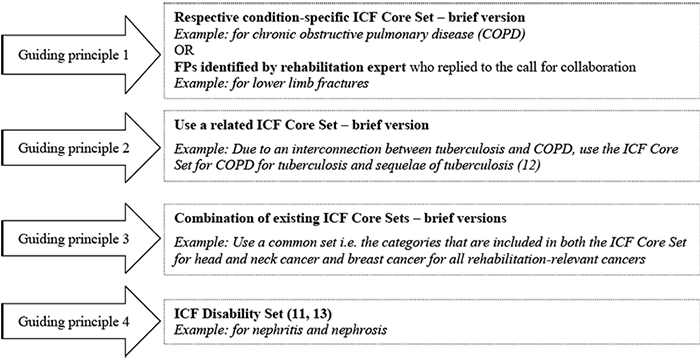
For the health conditions for which no ICF Core Sets were available nor populated by a contributing expert, a set of guiding principles was established to steer the decision as to which ICF categories should be employed as FPs for the respective health condition. Fig. 2 outlines this set of guiding principles (11–13). Guiding principle 1 reflects the starting point, i.e. the FPs should be populated with the A&P categories of the Brief ICF Core Set for the specified health condition, if it exists, or with categories established by an expert for the respective health condition. If guiding principle 1 is not possible, then guiding principle 2 should be followed. Likewise, if guiding principle 2 is not possible, then guiding principle 3 should be followed. This procedure continues until guiding principle 4 applies. Guiding principle 4 dictates that the ICF Disability Set should be used (11, 13). The ICF Disability Set is a set of 30 categories that was developed based on an extensive psychometric study and additional categories from the ICF Core Sets for acute, early-post acute, and geriatric settings, and are considered the most relevant for describing functioning across clinical populations along the continuum of care.
RESULTS
Based on a re-evaluation of the list of rehabilitation-relevant health conditions, 11 conditions were deleted from the original list of 103 health conditions. These conditions were either the cause of a health condition rather than a condition itself, e.g. Drownings, Fires, Falls, Poisonings, Road traffic accidents, Violence, War, interventions, e.g. Joint arthroplasty, or were not a specific health condition e.g. Other intentional injuries, Other unintentional injuries, Self-inflicted injuries (Table I).
|
Table I. Health conditions that were deleted from the original list of rehabilitation-relevant health conditions to populate |
||
|
Health condition (n = 10) |
ICD-10 code |
Reason for deleting |
|
Drownings |
T75.1 |
Not health condition |
|
Fires |
X00-09 |
Not health condition |
|
Falls |
W00-19 |
Not health condition |
|
Joint arthroplasty |
Z50.9 |
Intervention |
|
Other intentional injuries |
X83 |
Not health condition |
|
Other unintentional injuries |
V01-X59.9 |
Not health condition |
|
Poisonings |
T36-T50 |
Not health condition |
|
Road traffic accidents |
V01-V99 |
Not health condition |
|
Self-inflicted injuries |
X60-X84 |
Not health condition |
|
Violence |
R45.6, T74.0 |
Not health condition |
|
War |
Y36 |
Not health condition |
Seven conditions for which ICF Core Sets were available (Depression, Hand conditions, Inflammatory Bowel Disease, Obesity, Osteoporosis, Sleep disorders, Vertigo) and 1 condition that was populated by a WHO intern (Acute myocardial infarction) were added to the list (Table II), resulting in a list of 100 rehabilitation-relevant health conditions for which FPs required populating.
Recruitment efforts resulted in the agreement of 30 experts to contribute to the ICD-ICF joint use initiative. Twenty-six experts from all over the world (Belgium, Brazil, Canada, Croatia, France, Italy, Rwanda, Turkey, Slovenia, South Africa, USA) participated in the live online tutorials. However after the completion of the tutorials and some follow-up activities, only 4 health conditions were actually populated by contributing experts (Falls, Fracture of the femur, HIV/AIDS, Vertebral fractures). As previously mentioned, Falls was later deleted from the list of health conditions. The main reason indicated for not being able to contribute was limited resources and time constraints. For some, the online tutorial made the extensive requirements for completing the task more transparent; this seemed to deter some of the experts who initially agreed to contribute to the ICD-ICF joint use initiative from fully committing or following through with their commitment.
The FPs for Acute myocardial infarction, Asthma and Epilepsy were populated by interns at WHO (Table II).
|
Table II. Rehabilitation-relevant health conditions that have been populated with functioning properties (FP) |
|
|
Health condition (n = 100) |
ICF set used to populate FPs |
|
Acute myocardial infarction |
FP identified by WHO |
|
Alzheimer and other dementias |
Disability Set |
|
Amputation (traumatic amputations involving multiple body regions) |
Disability Set |
|
Amyotrophic diseases (amyotrophic lateral sclerosis) |
ICF Core Set for neurological conditions post-acute |
|
Ankylosing spondylitis and other spondylopathies |
Use ICF Core Set for ankylosing spondylitis |
|
Asthma |
FP identified by WHO |
|
Benign prostatic hypertrophy |
Disability Set |
|
Bipolar affective disorder |
ICF Core Set for bipolar disorders |
|
Birth asphyxia and birth trauma |
Adapted ICF Core Set for cerebral palsy |
|
Bladder cancer |
Adapted common set of ICF Core Sets for breast cancer and head/neck cancer |
|
Brain injury (traumatic brain injury or acquired brain injury) |
ICF Core Set for traumatic brain injury |
|
Breast cancer |
ICF Core Set for breast cancer |
|
Cerebral palsy |
Adapted ICF Core Set for cerebral palsy |
|
Cerebrovascular disease including stroke |
ICF Core Set for stroke |
|
Cervix uteri cancer |
Adapted common set of ICF Core Sets for breast cancer and head/neck cancer |
|
Chagas disease |
Disability Set |
|
Chronic obstructive pulmonary disease |
ICF Core Set for COPD |
|
Cleft lip |
Disability Set |
|
Cleft palate |
Disability Set |
|
Colon and rectum cancers |
Adapted common set of ICF Core Sets for breast cancer and head/neck cancer |
|
Complex regional pain syndrome |
ICF Core Set for chronic widespread pain |
|
Congenital heart anomalies |
ICF Core Set for cardiopulmonary conditions |
|
Corpus uteri cancer |
Adapted common set of ICF Core Sets for breast cancer and head/neck cancer |
|
Depression |
ICF Core Set for depression |
|
Diabetes mellitus |
ICF Core Set for diabetes mellitus |
|
Down syndrome |
Disability Set |
|
Drug use disorders |
Disability Set |
|
Endocrine disorders |
Disability Set |
|
Epilepsy |
FP identified by WHO |
|
Fracture of femur |
FP identified by expert |
|
Fracture of lower leg, including ankle |
FP for fracture of femur |
|
Fracture of lumbar spine and pelvis |
Disability Set |
|
Gout |
ICF Core Set for musculoskeletal conditions |
|
Haemophilia |
Disability Set |
|
Hand conditions |
ICF Core Set for hand conditions |
|
Hearing loss, adult onset |
ICF Core Set for hearing loss |
|
Heart failure |
ICF Core Set for cardiopulmonary conditions |
|
HIV/AIDS |
FP identified by expert |
|
Hypertensive heart disease |
ICF Core Set for cardiopulmonary conditions |
|
Impingement syndrome |
ICF Core Set for chronic widespread pain |
|
Inflammatory bowel disease |
ICF Core Set for IBD |
|
Ischaemic heart diseases |
ICF Core Set for chronic ischaemic heart disease |
|
Japanese encephalitis |
Disability Set |
|
Leishmaniasis |
Disability Set |
|
Leprosy and sequelae of leprosy |
Disability Set |
|
Leukaemia |
Adapted common set of ICF Core Sets for breast cancer and head/neck cancer |
|
Liver cancer |
Adapted common set of ICF Core Sets for breast cancer and head/neck cancer |
|
Low back pain (dorsalgia) |
ICF Core Set for low back pain |
|
Low birth weight |
Adapted ICF Core Set for cerebral palsy |
|
Lower limbs fractures |
FP for fracture of femur |
|
Lower respiratory infections |
ICF Core Set for COPD |
|
Lymphatic filariasis |
Disability Set |
|
Lymphomas and multiple myeloma |
Adapted common set of ICF Core Sets for breast cancer and head/neck cancer |
|
Macular degeneration and other sense disorders |
Disability Set |
|
Malaria |
Disability Set |
|
Melanoma and other skin cancers |
Adapted common set of ICF Core Sets for breast cancer and head/neck cancer |
|
Meningitis |
Disability Set |
|
Mental and behavioural disorders due to use of alcohol |
Disability Set |
|
Mild mental retardation attributable to lead exposure (unspecified mental retardation) |
Disability Set |
|
Mouth and oropharynx cancers |
ICF Core Set for head/neck cancer |
|
Movement disorders (e.g. ataxia, hemiplegia, dysdiadochokinesia) |
ICF Core Set for neurological conditions post-acute |

|
Table II. Contd. |
|
|
Health condition (n = 100) |
ICF set used to populate FPs |
|
Multiple sclerosis |
ICF Core Set for multiple sclerosis |
|
Muscle dystrophy |
ICF Core Set for neurological conditions post-acute |
|
Musculoskeletal pain syndrome (fibromyalgia, entrapment/ mononeuropathies) |
ICF Core Set for chronic widespread pain |
|
Myopathies |
ICF Core Set for neurological conditions post-acute |
|
Nephritis and nephrosis |
Disability Set |
|
Neuropathies |
ICF Core Set for neurological conditions post-acute |
|
Obesity |
ICF Core Set for obesity |
|
Oesophageal atresia |
Disability Set |
|
Oesophagus cancer |
ICF Core Set for head/neck cancer |
|
Onchocerciasis |
Disability Set |
|
Osteoarthritis |
ICF Core Set for osteoarthritis |
|
Osteoporosis |
ICF Core Set for osteoporosis |
|
Other joint disorder, not elsewhere classified |
ICF Core Set for musculoskeletal conditions |
|
Other neurotic conditions |
Disability Set |
|
Ovary cancer |
Adapted common set of ICF Core Sets for breast cancer and head/neck cancer |
|
Pancreas cancer |
Adapted common set of ICF Core Sets for breast cancer and head/neck cancer |
|
Parkinson disease |
ICF Core Set for neurological conditions post-acute |
|
Poliomyelitis and sequelae of poliomyelitis |
Disability Set |
|
Post-traumatic stress disorder |
Disability Set |
|
Prostate cancer |
Adapted common set of ICF Core Sets for breast cancer and head/neck cancer |
|
Protein-energy malnutrition |
Disability Set |
|
Pulmonary hypertension |
ICF Core Set for cardiopulmonary conditions |
|
Renal failure |
Disability Set |
|
Rheumatic heart disease |
ICF Core Set for cardiopulmonary conditions |
|
Rheumatoid arthritis |
ICF Core Set for rheumatoid arthritis |
|
Schizophrenia |
Disability Set |
|
Scleroderma, dermatomyositis |
Disability Set |
|
Skin diseases, e.g. psoriasis, decubitus ulcer and pressure area, other disorders of skin and subcutaneous tissue not elsewhere classified |
Disability Set |
|
Sleep disorders (obstructive sleep apnoea, narcolepsy, insomnia, circadian rhythm sleep-wake disorder, restless legs) |
ICF Core Set for sleep disorders |
|
Spina bifida |
ICF Core Set for spinal cord injury |
|
Spinal cord injury |
ICF Core Set spinal cord injury |
|
Stomach cancer |
Adapted common set of ICF Core Sets for breast cancer and head/neck cancer |
|
Syphilis |
Disability Set |
|
Tetanus |
Disability Set |
|
Trachea, bronchus and lung cancers |
ICF Core Set for head/neck cancer |
|
Tuberculosis and sequelae of tuberculosis |
ICF Core Set for COPD |
|
Upper limbs fractures |
ICF Core Set for musculoskeletal conditions |
|
Vertebral fractures |
FP identified by expert |
|
Vertigo |
ICF Core Set for vertigo |
|
COPD: chronic obstructive pulmonary disease; IBD: inflammatory bowel disease; WHO: World Health Organization; ICF: International Classification of Functioning, Disability and Health. |
|
Table II shows that, from 10 health conditions 34 conditions were populated with guiding principle 1 considerations, i.e. using existing ICF Core Set categories (n = 27) or with FPs identified by a contributing expert (n = 7), 19 conditions with guiding principle 2, i.e. with related ICF Core Sets, 15 conditions with guiding principle 3, i.e. with adaptations of existing ICF Core Sets, and 33 conditions with guiding principle 4 or with the ICF Disability Set.
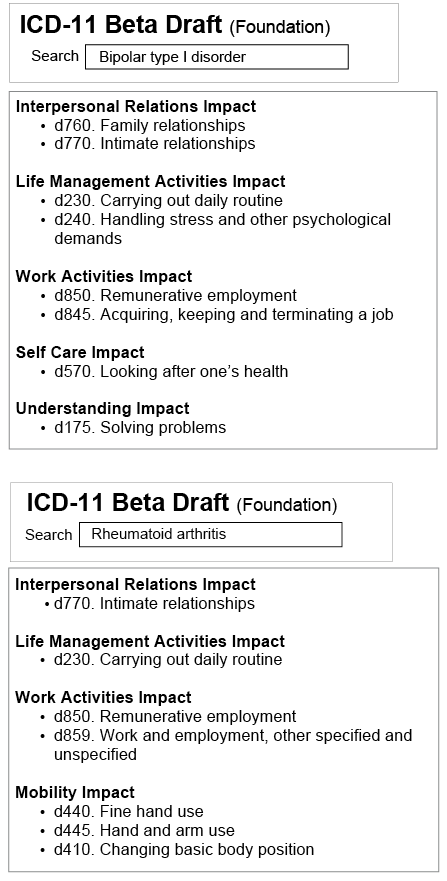
The FPs for the 100 health conditions can now be viewed in the online beta-version of the ICD-11 (5). FPs are presented as ICF categories and listed under the headings that represent the areas of functioning that are impacted by the specific health condition: Community Impact, Interpersonal Relations Impact, Household Activities Impact, Life Management Activities Impact, School Activities Impact, Work Activities Impact, Mobility Impact, Self Care Impact, Social Participation Impact, Understanding Impact and Children and Youth Impact (6). Fig. 3 illustrates 2 examples, i.e. for Bipolar type 1 disorder and for Rheumatoid arthritis, of how FPs are depicted in the ICD-11 beta-browser.
DISCUSSION
The difficulty in recruiting experts to assist in this project was disappointing, although not totally unexpected. Although the ICF is well-established the use in routine clinical practice has had a relatively slow uptake (14). Subsequently the pool of available clinicians who are both experts in particular conditions as well as having sufficient expertise with the ICF in order to develop a list of FPs for the health conditions is limited. Some of the clinicians who had such expertise could not contribute to this process in view of their other commitments. It would be expected that given further time and exposure to the ICF the pool of clinicians familiar with both the clinical conditions and the ICF will continue to increase. Refinements to the selected health condition-relevant FPs can then be considered.
Some clinicians indicate that the large number of ICF categories is an impediment to the take-up of the ICF into their clinical practice. It is difficult to draw a clear conclusion if this is a major contributor to the limited pool of clinicians who have both condition-specific and ICF-specific expertise. If this is the case then there is reason to be optimistic – the ICF Core Sets, the Generic or Disability (11) will facilitate an increased uptake of the ICF in clinical settings.
Being able to see the language of functioning as part of the description of a specific health condition achieves a milestone in depicting health information in an integrated and comprehensive manner. Not only are FPs visible in the ICD-11, they are also listed alongside other properties of the health condition, such as the definition, the body site and body system that are affected by the health condition, signs and symptoms, etc., all of which are intended to guide the ICD-11 user in terms of what to consider when deciding on diagnosis and treatment. Rehabilitation clinicians and other ICD-11 users may already be familiar with the associations between functioning and health conditions. However, explicitly identifying FPs for specific health conditions further reinforces the importance of acquiring a broader and more meaningful picture of the health of persons and populations.
WHO and the functioning Topic Advisory Group (fTAG), a group of ICF experts established by WHO to advise WHO and the ICD-11 Revision Steering Group on optimally capturing the impact of disease on functioning in the ICD-11 (1, 2), are currently working to optimize the visualization of FPs in ICD-11 by its expected launch in 2017 (15). Considering that the final ICD-11 “will be ready to use with electronic health records and information systems”(15) providing a hyperlink to the ICF description of the respective FP in the ICF browser (16) may further encourage the clinician to consider functioning information in their diagnostic and treatment decision-making.
In a possible expansion of their clinical utility, the ICD and ICF can also be used complimentarily with other classifications such as the ISO-9999, an international classification of assistive products for persons with disability. In the WHO’s Priority Medical Devices project background paper on Global Burden of Disease, ICF and ISO-9999, the authors propose using ICF Core Sets and functioning profiles to build “bridges between diseases, disabilities and assistive devices” (17, 18). The paper provides an overview of 15 high burden diseases and their associated ISO-9999 assistive product classes and ICF Core Set or functioning profile.
Concrete implementation of joint use of ICD, ICF and other classifications in real-life clinical settings will require further conceptualization and planning in consideration of regional and local health systems. There are, however, ICF-based tools available, e.g. categorical profile related to the Rehab-Cycle that may facilitate the complementary use of ICD and ICF in clinical settings (19, 20). These tools can promote effective communication within a multidisciplinary rehabilitation team and guide goal-setting and intervention planning across disciplines.
Beyond the clinical setting, other areas of application in which joint use of ICD and ICF may find utility include casemix modelling (21), home care (22), and comprehensive and transparent reporting in medical evaluations of work capacity (23).
In conclusion, capturing the impact of disease on functioning as depicted by FP in the (beta-version) ICD-11 reflects the potential expressed in the words of the WHO-FIC: “joint use of (the ICD, ICF and other) classifications renders better health information, identifying associations between diseases, disability and interventions. In this way knowledge could be distilled about the impact of the diseases and various interventions” (21, 24). It also holds promise in fulfilling the rehabilitation community’s long-standing endeavour to facilitate the implementation of the ICF in rehabilitation practice.
Acknowledgements
The authors would like to thank Associate Professor Aydan Oral, Istanbul University Faculty of Medicine (Turkey), Professor Peter Takac and Dr Anna Kubincova, both from the Pavol Jozef Safarik University Faculty of Medicine (Slovak Republic) and Associate Professor Hellen Myezwa, University of the Witwatersrand (South Africa) for their valuable work in populating FPs for selected health conditions, as well as to Anni Preisler, former WHO Fellow, for providing essential technical support. We would also like to express our gratitude to Christoph Gutenbrunner Professor at Hannover Medical School (Germany) and International Society of Physical and Rehabilitation Medicine (ISPRM) Liaison Officer to the WHO, Nenad Konstanjsek, Classification, Terminology and Standards – World Health Organization (Switzerland) and Assistant Professor Reuben Escorpizo, University of Vermont (USA), who have been instrumental in laying down the foundation for the ICD-ICF joint use initiative.
Any views expressed by the authors in this paper do not necessarily reflect the official views of the Office of the Assistant Secretary for Planning and Evaluation, Department of Health and Human Services, USA.
References

