Roel De Ridder, PhD1, Tine Willems, PhD2, Jos Vanrenterghem, PhD3 and Philip Roosen, PhD1
From the 1Department of Rehabilitation Sciences and Physiotherapy, 2Department of Orthopedics and Physiotherapy, Ghent University, Ghent, Belgium, 3School of Sport and Exercise Sciences, Faculty of Science, Liverpool John Moores University, Liverpool, UK
OBJECTIVE: To evaluate the effect of balance surface type on muscle activity of ankle stabilizing muscles in subjects with chronic ankle instability.
DESIGN: Case-controlled, repeated-measures study design.
SUBJECTS: Twenty-eight subjects with chronic ankle instability and 28 healthy controls.
METHODS: Subjects performed a barefooted single-legged stance on uniaxial and multidirectional unstable surfaces. Muscle activity of the mm. peroneus longus/brevis, tibialis anterior, gastrocnemius medialis were registered using surface electromyography. Mixed model analysis was used to explore differences in muscle activity between subjects with chronic ankle instability and controls, and the effect of surface type on muscle activity levels within subjects with chronic ankle instability.
RESULTS: No differences were found between subjects with chronic ankle instability and healthy controls. Within subjects with chronic ankle instability, balancing along a frontal axis and on the Both Sides Up evoked overall highest muscle activity level, and the firm surface the least. Balancing on the firm surface showed the lowest tibialis anterior/peroneus longus muscle ratio, followed by balancing along a frontal axis and on the Airex pad.
CONCLUSION: Clinicians can use these findings to improve the focus of balance training programmes by gradually progressing in difficulty level based on muscle activation levels taking co-contraction ratios into account.
Key words: ankle joint; joint instability; postural balance; rehabilitation.
J Rehabil Med 2015; 47: 632–638
Correspondence address: Roel De Ridder, De Pintelaan 185, 3B3, BE- 9000 Ghent, Belgium. E-mail: Roel.DeRidder@ugent.be
Accepted Mar 3, 2015; Epub ahead of print Jun 1, 2015
INTRODUCTION
Balance training is by far the most commonly implemented component of a rehabilitation protocol for chronic ankle instability (CAI). This is based on the idea that subjects with CAI have impaired neuromuscular control (1), which in normal conditions can be defined as the subconscious activation of dynamic restraints occurring in preparation for, and in response to, joint motion and loading (2). This impaired neuromuscular control is believed to be a consequence of damage to the mechanoreceptors as a result of sustained ankle sprains, referred to as partial deafferentiation (3, 4). In addition to afferent input, changes in central processing and alpha motoneuron pool excitability (efferent output) also contribute to general neuromuscular impairment (5). This impairment is thought to lead, in turn, to repetitive episodes of giving way and even ankle sprains, and is, consequently, considered an important underlying mechanism for CAI.
The primary aim of balance training is regaining a normal functional level of neuromuscular control around the ankle joint. Balance training may influence afferent input, result in changes in the sensory cortex, and might augment motoneuron pool excitability (6, 7). Furthermore, balance training effectively reduces the risk of sustaining an ankle sprain (8, 9). However, not all balance training studies have demonstrated improvement in functional outcome parameters such as postural control in subjects with CAI (10). A possible explanation is the wide variety of balance training protocols and the fact that it is not known which exercises best serve the rehabilitation goals.
Current knowledge on the influence of commonly used balance equipment on muscle activity levels is based on studies including predominantly healthy subjects (11–14). Thus far, no studies have evaluated the effect of balance surface type on muscle activity levels in subjects with CAI. However, maximally stimulating muscle activity levels is expected to accelerate the rehabilitation process to pre-injury functional levels (12). In addition, most balance protocols use unstable devices without control over the direction in which the ankle is challenged. This reflects a functional situation, as one has to be able to stabilize the ankle joint independent of triggering direction. However, in a progressive treatment protocol, it may be desirable to focus specifically on resolving deficits of specific ankle stabilizing muscles, especially in the early stages of rehabilitation, e.g. targeting the peroneus longus muscle in subjects with CAI. To make a clear statement on how to progress during balance training, however, research is lacking on the effect of surface types on muscle activity in subjects with CAI.
The main goal of this study was to evaluate the effect of 4 different surface types, i.e. a firm surface, a uniaxial wobble board with 2 different foot orientations, and 2 multidirectional unstable devices (Airex pad (Airex AG, Sins, Switzerland) and Both Sides Up (BOSU, Ashland, Ohio, USA)), on muscle activity levels of ankle stabilizing muscles during a single-legged balance protocol. The first objective was to investigate whether there were differences in muscle activity levels of ankle stabilizing muscles during the various conditions between subjects with CAI and healthy controls. The second objective was to assess the influence of surface type on these muscle activity levels in subjects with CAI.
METHODS
Subjects
A total of 56 subjects (28 subjects with CAI and 28 healthy matched controls) volunteered to perform a single-legged balance protocol. Population characteristics are shown in Table I. Subjects with CAI had to meet all of the following inclusion criteria: a history of a severe ankle sprain resulting in limitations in participation for at least 3 weeks; episodes of giving way; repetitive ankle sprains; feelings of instability and weakness around the ankle joint. Healthy control subjects reported no history of an ankle sprain in the past. Overall, subjects had to be recreationally active, defined by a minimum of 1.5 h of cardiovascular activity per week. Exclusion criteria were ankle fracture or surgery, lower limb complaints at the moment of testing (not related to CAI), and equilibrium disorders. For subjects with CAI, the unstable ankle was tested and, in case of bilateral instability, the most unstable ankle based on subject indication was included. The healthy controls were matched to the subjects with CAI based on age, height and body weight. Subsequently, leg dominance was taken into account, i.e. if the dominant leg of the subject with CAI was screened the dominant leg for the matched control was also tested, and vice versa. This study was approved by Ghent University Hospital ethics committee and all subjects provided informed consent.
Procedure
Anthropometric data and medical history were collected for all subjects (Table I). In addition, the Foot and Ankle Disability Index (FADI), its Sports Subscale (FADI-S), and the Cumberland Ankle Instability Tool (CAIT) were completed for group descriptive purposes. All subjects were tested unilaterally. Muscle activity of the mm. tibialis anterior, peroneus longus/brevis, and gastrocnemius medialis were registered using surface electromyography at 1,000 Hz (Myosystem 1400A, Noraxon USA Inc., Scottsdale, AZ, USA). In preparation, the skin was clean-shaven, scrubbed and degreased using ether to reduce skin impedance. Disposable bipolar Ag/AgCl surface electrodes, 2 cm diameter, with conducting gel were placed with an inter-electrode distance of 2 cm centre-to-centre and parallel to the muscle fibres according to Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscles (SENIAM) guidelines (www.seniam.org). Signal quality was checked and a baseline rest signal lower than 10 mV was required. Amplifiers were taped onto the lower leg and all wires were fixed by means of a circular gauze in order to reduce the possibility of motion artefacts. Subsequently, 3 maximal voluntary contractions for all registered muscles were recorded.
|
Table I. Population characteristics |
||
|
CAI (n = 28) |
Controls (n = 28) |
|
|
Age, years, mean (SD) |
20.3 (1.8) |
20.3 (1.8) |
|
Height, m, mean (SD) |
1.71 (0.7) |
1.72 (0.6) |
|
Weight, kg, mean (SD) |
63.4 (6.5) |
62.6 (7.5) |
|
BMI, mean (SD) |
21.6 (1.7) |
21.2 (2.3) |
|
FADI, mean (SD) |
90.6 (5.8) |
100.0 (0.2)* |
|
FADI-S, mean (SD) |
76.7 (12.7) |
99.6 (1.8)* |
|
CAIT, mean (SD) |
14.8 (3.8) |
29.7 (0.9)* |
|
Number of sprains, mean (SD) |
7.8 (6.4) |
N/A |
|
Time to last sprain, months, mean (SD) |
5.2 (6.3) |
N/A |
|
Orthotics (tape/brace) during sports, n |
19/28 |
0/28 |
|
Insoles, n |
12/28 |
7/28 |
|
*Significant group difference with p < 0.001. CAI: chronic ankle instability; BMI: body mass index; FADI: Foot and Ankle Disability Index; FADI-S: Foot and Ankle Disability Index – Sports Subscale; CAIT: Cumberland Ankle Instability Tool; SD: standard deviation. |
||
The balance protocol consisted of a barefooted single-legged stance on 4 different surfaces, including a flat surface, an Airex foam pad, a BOSU and a custom-made uniaxial balance board (Fig. 1). For the BOSU, the single-leg stance was performed standing on the soft side with the firm side on the ground. The wobble board surface was 40 × 40 cm with 2 identical segments of a circle underneath creating the axis of rotation (chord length = 28 cm, segment height = 8 cm, segment width = 4.5 cm). Two foot positions were marked on the uniaxial wobble board. The first foot orientation was aligned with the frontal axis of the foot (= WobF) inducing instability in the frontal plane (inversion/eversion). The second foot orientation was in alignment with a diagonal foot axis (= WobD), 45° externally rotated from the frontal axis and creating a plantarflexion/eversion and dorsiflexion/inversion motion. The wobble board was tested on subjects with CAI to make sure that it was possible to maintain balance for 5 s without touching the ground with the rim of the board. In general, subjects had to maintain a single-legged stance with the knee of the tested leg slightly flexed (knee above the toes, based on visual inspection by the researcher). Subjects had to assume the single-legged balance position with support of their hands on a chair and had to focus on a mark on the wall at eye height. Subsequently, they had to find balance, slowly release their hands from the chair and place them on their hips. If this was performed in a stable way, the measurement started. After a practice trial, the balance exercise was repeated until 3 successful balancing trials of 5 s were performed on each surface. A trial was discarded if subjects did not keep their hands on their hips, if the balancing foot shifted, if the contralateral foot touched the ground, or if both legs were pushed together for balance. A rest period of 30 s was foreseen between trials and of 1 min 30 s between surface types. The order of the surfaces was randomized and counterbalanced between groups.
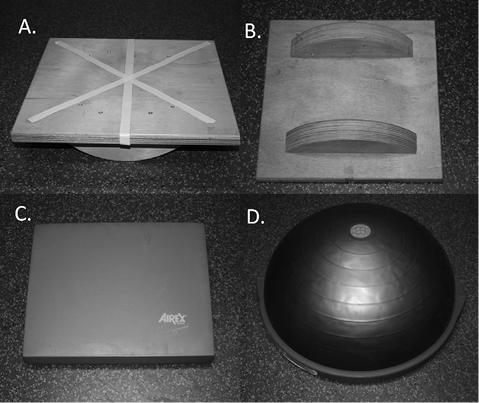
Fig. 1. Surface types: (A) top custom-made wobble board with lines indicating foot orientation; (B) bottom custom-made wobble board; (C) Airex pad; (D) Both Sides Up (BOSU).
Data processing and analysis
MyoResearch 3.4.5. Master Edition (Noraxon USA Inc., Scottsdale, AZ, USA) was used for the processing of the electromyography (EMG) data. The raw data of the EMG signals were full-wave rectified and smoothed using a root mean square with moving average window of 100 ms. The mean EMG value was determined over every 5 s balancing interval and, subsequently, the mean of the 3 trials on every individual surface type was calculated. For every muscle these values were then normalized to the respective highest maximal voluntary contraction value of the 3 trials. To illustrate the co-contraction between the invertor/evertor muscle activity, the mm. tibialis anterior/peroneus longus ratio (TA/PL ratio) was calculated by dividing the normalized activity values of these muscles.
Statistical analysis was performed with SPSS 22 (SPSS Inc., Chicago, IL, USA). For the first research question, differences in muscle activity levels by muscle on the various surfaces between study groups were evaluated using mixed model analyses to analyse interaction effect, i.e. surface*group. In case of a significant interaction effect, multiple pairwise comparisons with a Holm-Bonferroni correction were performed. Secondly, within the CAI group, mixed model analysis was performed for each individual muscle and the TA/PL ratio to assess the effect of surface on muscle activity levels. Post-hoc multiple pairwise comparisons were performed with a Holm-Bonferroni correction. Significance levels were set at p < 0.05.
RESULTS
Subjects with chronic ankle instability vs matched controls
Only for the medial gastrocnemius a significant interaction effect was found between surface and group (p = 0.007). However, post-hoc pairwise comparisons indicated no significant difference in muscle activity levels for the different surfaces between subjects with CAI and matched controls. Mean muscle activity levels are presented in Table II.
|
Table II. Normalized muscle activity (%) on different surface types for subjects with chronic ankle instability and healthy controls |
|||||||||||
|
MG |
TA |
PL |
PB |
||||||||
|
CAI Mean (SD) |
CON Mean (SD) |
CAI Mean (SD) |
CON Mean (SD) |
CAI Mean (SD) |
CON Mean (SD) |
CAI Mean (SD) |
CON Mean (SD) |
||||
|
Firm |
20.2 (11.8) |
21.5 (12.3) |
15.3 (10.5) |
19.2 (13.1) |
33.1 (13.8) |
34.4 (19.2) |
27.0 (11.8) |
27.7 (14.8) |
|||
|
Airex |
29.1 (16.6) |
31.9 (17.1) |
28.9 (13.7) |
39.5 (27.1) |
44.8 (14.3) |
50.7 (23.9) |
45.7 (17.8) |
51.6 (25.2) |
|||
|
BOSU |
43.8 (22.6) |
36.4 (16.7) |
46.5 (26.5) |
53.6 (24.4) |
59.8 (25.0) |
66.3 (29.4) |
66.4 (18.3) |
70.0 (31.6) |
|||
|
WobF |
38.9 (21.9) |
29.4 (13.5) |
43.0 (22.9) |
44.8 (23.0) |
66.0 (29.8) |
64.9 (30.5) |
68.2 (20.6) |
64.2 (26.5) |
|||
|
WobD |
41.1 (26.7) |
35.4 (12.2) |
41.2 (32.2) |
43.4 (22.4) |
44.6 (17.6) |
48.8 (14.3) |
45.5 (17.9) |
50.2 (22.0) |
|||
|
MG: medial gastrocnemius; TA: m. tibialis anterior; PL: m. peroneus longus; PB: m. peroneus brevis; CAI: subjects with chronic ankle instability; CON: healthy controls; BOSU: Both Sides Up; WobF: Wobble board along the frontal axis; WobD: Wobble board along the diagonal axis. |
|||||||||||
Effect of surface type within subjects with chronic ankle instability
Mixed model analysis showed significant differences in muscle activation according to the surface for all muscles tested (p < 0.001). The pairwise comparison results, with mean differences and confidence intervals, are presented in Table III. Overall, the single-legged stance on a firm surface evoked significantly lower muscle activity levels for all muscles (medial gastrocnemius, firm vs Airex: p = 0.006; for all other muscles: p < 0.001) and had a significantly lower TA/PL ratio compared with the other surface types (p < 0.001). The results of the influence of surface type on muscle activity levels are described below without further reference to the firm surface results. A comprehensive visual overview of the impact of surface on activity levels of all tested muscles is given in Fig. 2.
|
Table III. Post-hoc multiple pairwise comparisons with Holm-Bonferroni correction of the muscle activity levels (% normalized to MVC) according to the different surface types within each muscle |
||||||||||||||
|
Surface |
Medial gastrocnemius |
Tibialis anterior |
Peroneus longus |
Peroneus brevis |
TA/PL ratio |
|||||||||
|
Mean Diff [95% CI] |
p-value |
Mean Diff [95% CI] |
p-value |
Mean Diff [95% CI] |
p-value |
Mean Diff [95% CI] |
p-value |
Mean Diff [95% CI] |
p-value |
|||||
|
Firm-AIR |
–8.9 [–13.8, –3.9] |
0.006* |
–13.6 [–17.8, –9.3] |
< 0.001* |
–11.8 [–15.4, –8.2] |
< 0.001* |
–18.7 [–23.9, –13.5] |
< 0.001* |
–18.8 [–28.1, –21.2] |
< 0.001* |
||||
|
Firm- BOSU |
–23.6 [–30.0, –17.1] |
< 0.001* |
–31.2 [–39.2, –23.2] |
< 0.001* |
–26.7 [–34.3, –19.2] |
< 0.001* |
–39.4 [–44.9, –34.0] |
< 0.001* |
–32.8 [–44.6, –14.9] |
< 0.001* |
||||
|
Firm-WobF |
–18.6 [–25.4, –11.9] |
< 0.001* |
–27.7 [–34.9, –20.4] |
< 0.001* |
–32.9 [–42.1, –23.7] |
< 0.001* |
–41.2 [–48.3, –34.1] |
< 0.001* |
–18.8 [–27.2, –10.4] |
< 0.001* |
||||
|
Firm-WobD |
–20.9 [–28.6, –13.1] |
< 0.001* |
–25.9 [–35.7, –16.0] |
< 0.001* |
–11.5 [–14.8, –8.2] |
< 0.001* |
–18.5 [–23.9, –13.1] |
< 0.001* |
–45.8 [–63.0, –28.9] |
< 0.001* |
||||
|
AIR-BOSU |
–14.7 [–20.1, –9.3] |
< 0.001* |
–17.7 [–26.1, –9.2] |
< 0.001* |
–14.9 [–23.0, –6.9] |
0.003* |
–20.7 [–27.2, –14.2] |
< 0.001* |
–14.1 [–25.6, –2.6] |
0.054 |
||||
|
AIR-WobF |
–9.8 [–15.5, –4.0] |
0.010* |
–14.1 [–20.8, –6.4] |
0.005* |
–21.1 [–30.5, –11.7] |
< 0.001* |
–22.5 [–30.4, –14.6] |
< 0.001* |
0.1 [–8.1, 8.1] |
1.000 |
||||
|
AIR-WobD |
–12,0 [–19.0, –5.0] |
0.010* |
–12.3 [–22.5, –2.2] |
0.076 |
0.3 [–4.1, 4.6] |
0.906 |
0.2 [–6.1, 6.6] |
1.000 |
–27.0 [–44.1, –10.2] |
0.015* |
||||
|
BOSU-WobF |
5.0 [–2.1, 12.1] |
0.498 |
3.5 [–6.6, 13.7] |
1.000 |
–6.2 [–17.7, 5.3] |
0.566 |
–1.8 [–9.9, 6.3] |
1.000 |
14.1 [3.3, 24.9] |
0.048* |
||||
|
BOSU-WobD |
2.7 [–5.4, 10.8] |
1.000 |
5.4 [–6.7, 17.4] |
1.000 |
15.2 [7.3, 23.1] |
< 0.001* |
20.9 [14.3, 27.6] |
< 0.001* |
–13.0 [–31.3, 5.2] |
0.314 |
||||
|
WobF-WobD |
–2.3 [–10.6, 6.0] |
1.000 |
1.8 [–9.8, 13.4] |
1.000 |
21.4 [11.9, 30.9] |
< 0.001* |
22.7 [14.7, 30.7] |
< 0.001* |
–27.1 [–43.6, –10.6] |
0.012* |
||||
|
AIR: Airex; WobF: Wobble board along the frontal axis; WobD: Wobble board along the diagonal axis; MVC: maximal voluntary contraction; TA/PL ratio: mm. tibialis anterior/peroneus longus ratio; BOSU: Both Sides Up; 95% CI: 95% confidence interval. |
||||||||||||||
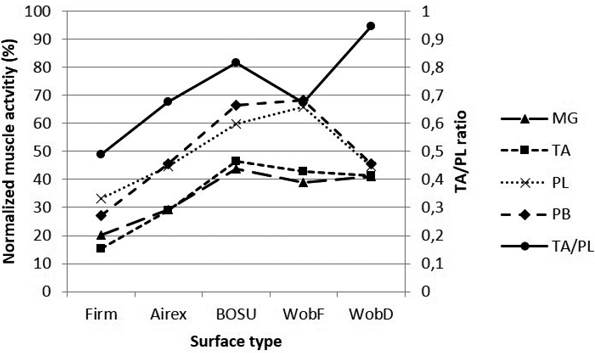
Fig. 2. Normalized muscle activity levels and mm. tibialis anterior/peroneus longus (TA/PL) ratio on the various surfaces. MG: m. medial gastrocnemius; TA: m. tibialis anterior; PL: m. peroneus longus; PB: m. peroneus brevis; WobF: wobble board along frontal axis; WobD: wobble board along diagonal axis; BOSU: Both Sides Up.
Effect of surface type on individual muscle activity. Results for peroneus longus and brevis muscles were similar. Both muscles displayed significantly higher activation levels when balancing on the WobF and the BOSU compared with balancing on the WobD (p < 0.001) and the Airex pad (m. peroneus longus: respectively p < 0.001 and p = 0.003; m. peroneus brevis: p < 0.001 for both). There was no significant difference in muscle activity between the WobF and the BOSU (m. peroneus longus: p = 0.566; m. peroneus brevis: p = 1.000), and between the WobD and the Airex pad (m. peroneus longus: p = 0.906; m. peroneus brevis: p = 1.000).
Muscle activation levels of the tibialis anterior muscle were significantly higher when balancing on the BOSU and the WobF compared with balancing on the Airex pad (respectively p < 0.001 and p = 0.005). There was no significant difference in muscle activation levels between the BOSU, WobF and WobD (p = 1.000 for all), and between the WobD and the Airex pad (p = 0.076).
Table II shows significantly higher muscle activation levels in the medial gastrocnemius when balancing on the BOSU, WobD and WobF compared with balancing on the Airex pad (respectively p < 0.001, p = 0.010, p = 0.010). There was no significant difference in muscle activation levels between the BOSU, WobF and WobD (respectively p = 0.498, p = 1.000, p = 1.000).
Effect of surface type on mm. tibialis anterior/peroneus longus ratio
The TA/PL ratio was significantly lower when balancing on the WobF and the Airex pad compared with the WobD (respectively p = 0.012 and p = 0.015). Balancing on the WobF and the Airex pad also displayed a lower TA/PL ratio compared with the BOSU, although the corrected p-value barely exceeded significance level for the Airex pad comparison (respectively p = 0.046 and p = 0.054). There was no significant difference between the WobF and the Airex pad (p = 1.000) or between the BOSU and the WobD (p = 0.314).
DISCUSSION
Balance training protocols incorporating different surface types are used in daily practice for the treatment of CAI even though the effect of surface type on muscle activation levels and TA/PL ratio is unknown. The results of our study indicated that the effect of surface type on muscle activity levels of the mm. peroneus longus/brevis, tibialis anterior and gastrocnemius medialis is not different between a healthy control group and subjects with CAI. Furthermore, within the CAI group, the BOSU and the WobF evoked overall largest muscle activity levels. In addition, the WobF generated a lower TA/PL ratio. These insights may be helpful in designing balance training programmes for subjects with CAI.
No differences were found between the matched controls and subjects with CAI regarding muscle activity levels evoked by the different surface types. This was somewhat unexpected in view of the reported neuromuscular dysfunctions related to CAI, indicating a decreased activity of the peroneus longus muscle during various tasks (15–18) and increased activity of the tibialis anterior muscle during hopping tasks (19, 20). These findings, however, are not reflected in the muscle activity levels in our study. A possible explanation might be that our results are not based on functional activities, as described above and, moreover, most of the described differences in muscle activity were observed in the preparatory phase before contact reflecting the feed-forward muscle activation patterns. This was not considered in the current study, in which only static single-legged stance exercises were assessed. When assuming that there is no difference between subjects with CAI and healthy controls in evoked muscle activity levels during static balance training independent of surface type, the results of studies on healthy subjects (11–14, 21, 22) might be extrapolated to subjects with CAI. Caution is warranted, as further research is needed on different surfaces to confirm this hypothesis.
Surface type clearly had an impact on evoked muscle activity levels within the CAI group. For all included muscles, single-leg balance on a flat surface produced least muscle activation levels. Both the mm. peroneus longus and brevis displayed higher muscle activation levels on the WobF and the BOSU compared with the WobD and the Airex pad. The higher activation on the WobF is to be expected based on the orientation of the axis of the balance board creating an inversion/eversion motion (23), which corresponds with the eversion function of the mm. peroneus longus and brevis (24). The higher muscle activity levels on the BOSU might be explained by a relatively high overall instability level of this multidirectional unstable device, represented by a higher centre of pressure area and mean sway velocity compared with, for example, an Airex pad (25). Also, for the tibial anterior muscle, the BOSU, together with the WobF, evoked highest muscle activation levels. We expected higher tibialis anterior muscle activation levels on the WobD (23); however, no significant differences in activation levels were found between the WobD and all other devices. The design of the custom-made balance board might explain these results, as it was less provocative to ensure subjects with CAI could balance for the requested period of time. Finally, for the medial gastrocnemius, highest muscle activity levels were also found on the BOSU, with no difference between the WobD and the WobF. Based on anatomical function (26), we expected lower muscle activity levels on the WobF (23). However, these results were not confirmed using our custom-made balance board. Exercising on the Airex pad produced lower muscle activity levels, possibly based on the lower sway velocity and centre of pressure area, as discussed above (25).
One of the main challenges of outlining such a balance training programme is to establish a progressive increase in difficulty level by selecting suitable exercises depending on pathology. Several studies have been carried out comparing the activity levels of lower limb muscles using different types of exercises, surfaces, playing with visual control, etc. (11–14, 21, 22). As CAI has been associated with a decreased function of the peroneus longus muscle (15–17, 27–30), rehabilitation exercises should target, in the first place, activation of this ankle-stabilizing muscle. Blackburn et al. (13) emphasized considering agonist-antagonist co-activation because of the risk of establishing disproportionate muscle activity gains, since increased muscle activity may not be a positive outcome for every injury scenario. For example, increased ankle-invertor strength without concomitant increases in evertor strength may predispose the ankle joint to inversion injury after invertor/evertor coactivation. Therefore, we also calculated the TA/PL ratio in addition to individual muscle activity levels. A lower ratio would indicate a invertor/evertor co-contraction in favour of the evertors. Based on our results, the following progressive scheme could be advised for treatment of subjects with CAI. To start, single-legged stance on a firm surface evokes overall lowest muscle activity levels and the lowest TA/PL ratio. Subsequently, single-legged stance on the Airex pad evokes overall low muscle activity levels and has, together with the WobF, a low TA/PL ratio. Based on muscle activity levels alone of the m. peroneus longus, exercising on the WobD is equal to exercising on an Airex pad. However, single-legged stance on the WobD generates the highest TA/PL ratio (TA 26% vs PL 12% muscle activity increase relative to single-legged stance on a firm surface) and is therefore not immediately an exercise of choice. Highest muscle activity levels for the m. peroneus longus are generated when exercising on the BOSU and the WobF. These exercises can be used to maximally target this ankle stabilizing muscle, based on the surface types compared in this study. When also considering the TA/PL ratio, single-legged stance on the WobF can be considered the best exercise to target the m. peroneus longus without possibly establishing disproportionate agonist-antagonist co-activation.
The use of a uniaxial balance board showed that, based on foot orientation, the agonist-antagonist co-activation can be somewhat controlled. Although the WobD did not evoke higher muscle activity levels of the m. tibialis anterior, as expected (23), the higher TA/PL ratio clearly showed that the tibialis anterior muscle is more targeted than the peroneus longus muscle. Similar findings were noted for the WobF, which evoked high muscle activity levels of the peroneus longus muscle, as expected (23), together with the BOSU. In addition, the WobF clearly showed a lower TA/PL ratio, indicating a higher focus on the peroneus longus muscle than on the tibialis anterior muscle compared with the BOSU. In rehabilitation of CAI, this exercise seems to better address the needs of this pathology. Therefore, in clinical practice, initially exercising on a uniaxial balance board should be considered before using high-level multidirectional unstable devices to focus on the intended muscles. Research on the functional outcome parameters of these exercises is required in order to assess their efficacy. An earlier study by Eisen et al. attempted to evaluate the effect of 4 weeks’ multidirectional or uniaxial balance training on the Star Excursion Balance Test (SEBT) in a small sample of healthy college athletes (31). They found no improvement in SEBT of the individual interventions, probably due to low statistical power. Further research in patient populations with CAI is necessary to evaluate the possible added value of uniaxial balance training.
This study has some limitations. The interpretation of the difficulty level of the included exercises is based solely on the evoked muscle activation levels. To assess the instability level and the direction of the instability, it would be interesting to see the effect of surface type, i.e. uniaxial vs different multidirectional devices, on COP displacement and sway velocity (25). We also used a custom-made balance board to ensure subjects with CAI were able to maintain their balance effectively. More research on similar devices is necessary to be able to extrapolate results. As no intervention was performed in the current study, the true effect on neuromuscular control of a balance training protocol using these recommendations is not yet known. Furthermore, not only static exercises are included in balance training programmes, as progression is typically made towards more dynamic and functional movements (32). The effect of surface types during these more dynamic and functional exercises have not yet been assessed in CAI. A recent study by Feger et al. found lower limb muscle activity levels in subjects with CAI compared with controls during several functional exercises, such as forward lunges and lateral hops, advocating the implementation of functional exercises into a rehabilitation programme (33). Further research is needed into the effect of surface type on muscle activity levels in subjects with CAI.
In conclusion, this study found no significant differences between subjects with CAI and matched controls during static balance exercises on various surfaces. For subjects with CAI, based on muscle activity levels and agonist-antagonist co-activation, a gradual progression in difficulty level can be made depending on surface type. Balancing on a firm surface evoked overall lowest muscle activation levels and a low TA/PL co-contraction, followed by balancing on an Airex pad. In order to maximally focus on the peroneus longus muscle with a low TA/PL ratio, balancing on a uniaxial wobble board with the axis orientated parallel underneath the foot can be advised. Balancing on the BOSU and the wobble board along the diagonal axis evoked the highest TA/PL ratio and may be less favourable at the beginning of a balance training programme. In order to develop evidence-based progressive balance training programmes further research is needed into the effect of surface type on muscle activity levels in subjects with CAI.
ACKNOWLEDGEMENTS
The authors would like to thank Joyce Sinnaeve and Marlien De Jans for their help in data collection for this study.
The authors declare no conflicts of interest.
REFERENCES

