Lillian Festvåg, PT, CandMag1,3, Anne-Kristine Schanke, CandPsychol, PhD1,2, Nils Erik Gilhus, MD, PhD4,5, Sigurd Aarrestad, MD6,7, Kari Lofthus, PT, CandMag8, Stein Johnsen3, Geir Strømsholm3, Steinar Øyhaugen3, Ragnhild Skovly Hartviksen3 and Johan Kvalvik Stanghelle, MD, PhD1,9
From the 1Sunnaas Rehabilitation Hospital HF, Nesoddtangen, 2Department of Psychology, University of Oslo, 3National Society of Polio Survivors, LFPS, 4Department of Clinical Medicine, University of Bergen, 5Department of Neurology, Haukeland University Hospital, Bergen, 6Department of Pulmonary Medicine, Oslo University Hospital Ullevål, 7Norwegian National Advisory Unit on Long Term Mechanical Ventilation, Haukeland University Hospital, Bergen, 8University Hospital of North Norway, Division of Neurosciences, Orthopedics and Rehabilitation Services and 9Institute of Clinical Medicine, Medical Faculty, University of Oslo, Oslo, Norway
OBJECTIVE: To explore the physical and social situation of the Norwegian polio population in 2014, and to compare the status of this population in 2014 with the results of a similar survey carried out 20 years previously, in 1994.
DESIGN: The study was based on a questionnaire covering demographics, polio history, and current medical, psychological and social conditions.
SUBJECTS: The questionnaire was prepared in cooperation with the National Society of Polio Survivors and others with known polio (n = 1,968). A total of 1,408 persons responded (72%), mean age 70 years (range 28–98 years).
RESULTS: The most frequent health problems reported were muscle and joint pain, cold intolerance and insomnia. New muscle weakness and loss of muscle volume were reported more frequently in 2014 than in the 1994 study. The use of orthopaedic aids, assistive devices, ventilators and other respiratory aids had increased significantly, but 83% reported that they still had no home care or nursing services support. The 2014 polio population reported only minor subjective worsening of health and well-being compared with the 1994 cohort.
CONCLUSION: The present study indicates that the elderly polio population are experiencing new muscle weakness and increasing health problems, but that the deterioration occurs slowly and with fewer consequences for the subjective experience of general health and well-being, indicating that the patients are adapting to their life situation. However, subgroups of the elderly polio population are in need of special care.
Key words: poliomyelitis; post-polio syndrome; rehabilitation; survey; neuromuscular disease.
J Rehabil Med 2016; 48: 00–00
Correspondence address: Lillian Festvåg, Sunnaas Rehabilitation Hospital, Bjørnemyrveien 11, NO-1450 Nesoddtangen, Norway. E-mail: Lillian.festvag@sunnaas.no
Accepted Apr 27, 2016; Epub ahead of print Aug 5, 2016
INTRODUCTION
The goal of eradicating poliomyelitis worldwide is close to being attained; new cases of poliomyelitis have decreased dramatically since the start of effective vaccination in 1956 (1). Since the majority of individuals living with the late effects of poliomyelitis in western countries are now middle-aged to elderly, a common misconception is that poliomyelitis has been conquered. However, although the vast majority of polio survivors are on disability pensions or retired, many are still of working age, especially if the younger polio population from developing countries are included. Worldwide, people who have recovered from polio infection will be affected for at least a generation (2).
Since the 1980s, increasing attention has been paid to the development of late-onset polio sequelae, or post-polio syndrome (PPS). However, less is known about how elderly polio survivors cope in the long-term.
The term PPS was introduced by Halstead & Grimby in 1985 and is characterized by a gradual or sudden onset of progressive or persistent new muscular weakness and abnormal muscle fatigue with or without generalized fatigue, muscle atrophy and muscle and joint pain (3).
The existence of PPS has been discussed, but it is now generally accepted as a clinical entity, and guidelines for diagnosis and management of PPS have been published in the international medical literature (4, 5).
Studies of PPS have focused mainly on new health problems and deteriorating neuromuscular function (6–10). In addition, attention has been paid to categorizing polio survivors into 2 groups; those with stable and unstable polio, respectively. Unstable post-polio is characterized by increasing loss of muscle strength over time (11, 12).
Fatigue, defined either as failure to sustain the force of muscle contraction (peripheral fatigue) or limited endurance of sustained physical and mental activities (central fatigue), is commonly reported among persons with late effects of poliomyelitis (13, 14), and has been confirmed in previous Norwegian studies (15, 16).
In addition, psychological distress and coping mechanisms are important for health and quality of life in the polio group. Polio survivors show high levels of emotional distress and fatigue at onset of the late effects of polio, as reported in 34–91% of cases (17, 18).
Several studies have considered perceived health and physical function from a longitudinal perspective (19–24), while few reports are based on epidemiological surveys (25, 26). A nationwide survey from Denmark in 1993 showed that the main new health problems in polio survivors were fatigue, muscle weakness, and pain, resulting in problems with activities of daily living (ADL), especially gait (27). These findings coincide with a population-based survey initiated by Lobben & Øyhaugen (28) and the National Society of Polio Survivors (LFPS) in Norway in 1994, which, in addition, showed a broad spectrum of health problems. The findings had great impact, both in generating comprehensive national rehabilitation programmes and in initiating further research on post-polio (28, 29). The present study is a follow-up, 20 years after the 1994 survey.
The main aim of the current survey was to explore the present situation of an ageing polio population with regards to their physical and social situation, and their needs for specialized healthcare. A further aim was to compare the status in 2014 with the findings 20 years earlier. Our hypothesis was that the current polio population would report more health problems due to their polio sequelae than in the 1994 study, and therefore challenge the healthcare system towards more and new therapeutic activities.
METHODS
Study design
The study is based on a postal questionnaire, comprising 87 questions with sub-items. The questionnaire was prepared in cooperation with the National Society of Polio Survivors, and to a great extent based on the survey from 1994. The questionnaire covered issues related to demographics, acute poliomyelitis, rehabilitation and stable phase, peak recovery, medical, psychological and social conditions. Resilience Scale for Adults (RSA-33), visual analogue scale (VAS), Fatigue Severity Scale (FSS) and Life Satisfaction Scale (Lisat-11) were included in the questionnaire.
The questionnaire was distributed in January 2014 to all registered members of LFPS (n = 1,998), and to all persons with a polio diagnosis registered by the South-Eastern Norway Health Authority, excluding members of LFPS (n = 152). At the same time the web-link was set up (www.tns-gallup.no/polio2014) and the survey was advertised on social media, resulting in 23 additional responders. One reminder was sent by post to non-responders.
Statistical analysis
The results are presented mainly as descriptive statistics, analysed using IBM SPSS Statistics version 21 (Armonk, NY, USA). Values are given as means and 95% confidence intervals (95% CI). Differences between the polio groups in 2014 and 1994 were studied by calculating the 95% CI for the 2 estimates compared, concluding that they are significantly different when they do not overlap. Significance was set at 0.05. Differences between sex were tested with χ2 for dichotomous variables. To adjust for sex differences in the response rate, the data were weighted in the reporting of results by the following values: women are given weight = 0.99342824451184, men are given weight = 1.10074172628988.
RESULTS
Inclusion
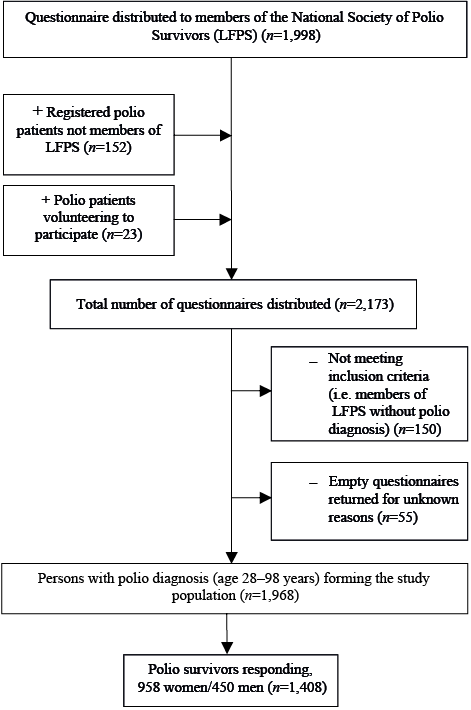
A total of 2,173 persons were invited to participate in this study (Fig. 1), of whom 1,968 fulfilled the inclusion criteria. A total of 1408 persons (958 women (68%) and 450 men (32%)) responded (response rate 72%). Reasons for exclusion were: not meeting the inclusion criteria, i.e. members of LFPS without a polio diagnosis (n = 150); and returned postal questionnaires not fully completed, for unknown reasons (n = 55) (Fig. 1).
Demographics
Mean response rate was 72%, compared with 61% in 1994. Due to patient anonymity, we do not know the number of patients who participated in both studies. Only 32% of the participants in 2014 remembered that they had participated in the 1994 study, whereas a further 24% were unsure. No official records of deaths among polio survivors were taken, but 177 members of LFPS were registered as dead during the 20-year period.
There were significant differences in most demographic data in 2014 vs 1994 (Table I). The mean age of the 2014 study population was 70 years, 20% were under 65 years of age, 51% were 65–74 years, 23% were 75–84 years, and 5% were over 84 years of age. The age distribution differs from the 1994 study population, which had a mean age of 57 years and a more even age distribution (27). The sum score of working status and relationship status is over 100%, as some participants ticked several options, e.g. part-time work and disability pension.
|
Table I. Demographics of subjects participating in 2014 and 1994 (27) |
||||||
|
|
2014 (n = 1,408) |
|
1994 (n = 1,444) |
p |
||
|
Mean (SD) [min–max] |
95% CI |
|
Mean (SD) [min–max] |
95% CI |
||
|
Response rate, years, % |
72 |
70–74 |
|
61 |
59–64 |
|
|
Age, mean (SD) (min–max) |
70 (9) [28–98] |
70–71 |
|
57 (10) [15–87] |
57–58 |
* |
|
Sex, women/men, % |
68/32 |
66–70/30–34 |
|
54/46 |
51–57/43–49 |
* |
|
Sex, women/men, n |
958/450 |
|
|
777/667 |
|
|
|
Working status, % |
|
|
|
|
|
|
|
Work (full-time) |
7 |
6–8 |
|
23 |
21–25 |
* |
|
Work (part-time) |
4 |
3–5 |
|
24 |
22–26 |
* |
|
Disability pension |
27 |
25–29 |
|
56 |
53–59 |
* |
|
Retirement |
60 |
57–63 |
|
20 |
18–22 |
* |
|
Relationship status, % |
|
|
|
|
|
|
|
Married/cohabitant |
63 |
61–66 |
|
71 |
69–73 |
* |
|
Divorced |
13 |
11–15 |
|
10 |
9–12 |
|
|
Single |
8 |
7–9 |
|
11 |
9–13 |
|
|
Widow/widower |
16 |
14–18 |
|
8 |
7–9 |
* |
|
Living conditions, % |
|
|
|
|
|
|
|
Villa/detached |
56 |
53–59 |
|
67 |
65–69 |
* |
|
Terraced, apartment block |
35 |
33–38 |
|
26 |
24–28 |
* |
|
Retirement home/sheltered housing |
4 |
3–5 |
|
7 |
6–8 |
* |
|
*Significance was set at 0.05 after calculating the 95% CI for the 2 estimates, concluding that they are significantly different when they do not overlap. CI: confidence interval; SD: standard deviation. |
||||||
Body characteristics
Mean body weight increased by 5 kg for the group as a whole, which led to a moderate increase in body mass index (BMI) (Table II). Some persons in 2014 had a very high body weight.
|
Table II. Body height, weight and body mass index (BMI) of subjects participating in 2014 and 1994 (27). Values are given in mean (standard deviation; SD) and minimum–maximum values |
||||||
|
|
2014 (n = 1,408) |
|
1994 (n = 1,444) |
p |
||
|
Mean (SD) [min–max] |
95% CI |
|
Mean (SD) [min–max[ |
95% CI |
||
|
Height, cm |
|
|
|
|
|
|
|
Women |
163 (13) [139–195] |
162–164 |
|
163 (6) [138–180] |
162–163 |
|
|
Men |
175 (8) [149–197] |
175–176 |
|
177 (8) [149–197] |
177–178 |
* |
|
Total |
168 (13) |
166–168 |
|
169 (9) |
169–170 |
* |
|
Weight, kg |
|
|
|
|
|
|
|
Women |
71 (14) [30–165] |
70–72 |
|
65 (11) [35–120] |
64–66 |
* |
|
Men |
82 (16)
|
81–83 |
|
76 (12)
|
75–77 |
* |
|
Total |
74 (16) |
73–75 |
|
70 (13) |
69–71 |
* |
|
BMI total |
27 (5) [11–65] |
27–27 |
|
25 (4) [15–44] |
25–25 |
* |
|
*Significance was set at 0.05 after calculating the 95% CI for the 2 estimates, concluding that they are significantly different when they do not overlap. CI: confidence interval; SD: standard deviation. |
||||||
Concomitant diseases
Major sex differences were found for age-related concomitant health problems (Table III), especially regarding osteoporosis and osteoarthritis, which were reported more frequently among women. Psychological problems requiring professional help were also more common among women, while sleep apnoea was a more dominant problem in the male polio population.
|
Table III. Prevalence (%) of concomitant health problems experienced by 1408 polio survivors in 2014 |
||||
|
|
Total (n = 1,408) |
Women (n = 957) |
Men (n = 451) |
p-value |
|
Osteoporosis (n = 1,193) |
18 |
25 |
4 |
< 0.001 |
|
Osteoarthritis (n = 1,193) |
45 |
53 |
28 |
< 0.001 |
|
Psychological problems (n = 1,195) |
18 |
20 |
12 |
< 0.001 |
|
Heart infarction (n = 1,215) |
16 |
6 |
14 |
< 0.001 |
|
Other cardiac diseases (n = 1,182) |
15 |
18 |
14 |
0.042 |
|
Asthma (n = 1,191) |
15 |
11 |
17 |
0.001 |
|
Chronic bronchitis, emphysema, COPD (n = 1,186) |
9 |
8 |
10 |
0.215 |
|
Cancer (n = 1,200) |
16 |
14 |
17 |
0.068 |
|
Sleep apnoea (OSA) (n = 1,157) |
20 |
17 |
26 |
< 0.001 |
|
Diabetes (n = 1,192) |
10 |
9 |
13 |
0.022 |
|
Rheumatoid arthritis (n = 1,175) |
7 |
8 |
5 |
0.010 |
|
Renal disorders (n = 1,186) |
6 |
6 |
4 |
0.045 |
|
COPD: chronic obstructive pulmonary disease; OSA: obstructive sleep apnoea. |
||||
Muscle weakness
In the acute phase, 90% of participants reported that they had varying degrees of paresis in the leg and hip muscles, and 61% reported paresis in the arms and shoulders (Table IV). Half of the group reported paralysis in the spinal or abdominal muscles, and one-third reported paresis in pharyngeal or respiratory muscles. These reports confirm that the group was severely affected in the acute phase.
|
Table IV. Prevalence (%) of persons experiencing some degree of paresis in the extremities, spinal, abdominal, respiratory and pharyngeal muscles in the acute phase of poliomyelitis |
||||
|
Body parts affected by polio in the acute phase* |
Total (n = 1408) |
Women (n = 957) |
Men (n = 451) |
p-value |
|
Legs (1 or both) (n = 1,252) |
90 |
90 |
90 |
0.056 |
|
Arms (1 or both) (n = 953) |
61 |
61 |
62 |
0.006 |
|
Spine/back (n = 900) |
53 |
53 |
52 |
0.164 |
|
Abdomen/chest (n = 838) |
43 |
42 |
45 |
0.246 |
|
Respiratory muscles (n = 800) |
21 |
19 |
23 |
0.067 |
|
Pharyngeal (n = 770) |
10 |
9 |
13 |
0.063 |
|
*Some, moderate, complete paresis. |
||||
Table V shows the answers to the question: “Have you experienced unexpected new muscle weakness or experienced unexpected loss of muscle size or volume?” The response in 2014 was compared with the response to the same question in 1994. There was a significant increase in reported new muscle weakness and loss of muscle size and volume, both in extremities previously known to be affected by polio and in muscles previously not known to be affected by polio. Men and women reported increased muscular weakness and loss of muscle volume to the same degree.
|
Table V. Prevalence of new muscle weakness and loss of muscle volume in the extremities reported in 1994 and 2014. Age when new muscle weakness occurred is given in mean years (standard deviation; SD) |
||||
|
|
2014 (n = 1,408) Mean (95% CI) |
1994 (n = 1,444) Mean (95% CI) |
Age at new weakness |
p |
|
New muscle weakness, % |
|
|
|
|
|
Extremities previously affected by polio |
95 (94–96) |
85 (83–87) |
46 (14) |
* |
|
Extremities previously not affected by polio |
67 (65–70) |
58 (56–61) |
50 (14) |
* |
|
Loss of muscle size or volume, % |
|
|
|
|
|
Extremities previously affected by polio |
63 (61–66) |
49 (46–52) |
46 (15) |
* |
|
Extremities previously not affected by polio |
38 (36–41) |
24 (22–26) |
51 (12) |
* |
|
*Significance was set at 0.05 after calculating the 95% CI for the 2 estimates, concluding that they are significantly different when they do not overlap. CI: confidence interval; SD: standard deviation. |
||||
Activities of daily living
The polio population needed help from others for several activities (Table VI). Climbing stairs was difficult, and was markedly worse in 2014 than in 1994. Also, walking had a higher percentage of persons in need of help in 2014. There was no change regarding assistance for personal hygiene. In total, 83% reported that they had no support from the public sector for home care or nursing services.
|
Table VI. Polio patients (%) in need of personal assistance for activities of daily living (ADL) in 2014 and 1994 |
|||
|
|
2014 (n = 1,408) Mean (95% CI) |
1994 (n = 1,444) Mean (95% CI) |
p |
|
Climbing stairs |
56 (53–59) |
23 (21–25) |
* |
|
Carry objects |
43 (40–46) |
43 (41–46) |
* |
|
Walking |
21 (19–23) |
16 (14–18) |
* |
|
Household tasks |
17 (15–19) |
31 (29–33) |
* |
|
Dressing |
9 (8–11) |
11 (9–13) |
|
|
Personal hygiene |
9 (8–11)) |
10 (9–12) |
|
|
Go to bed/get up |
7 (6–8) |
8 (7–9) |
|
|
Toileting |
10 (8–12) |
10 (9–12) |
|
|
Eating/swallowinga |
2 |
|
|
|
Cookinga |
12 |
|
|
|
*Significance was set at 0.05 after calculating the 95% confidence interval (CI) for the 2 estimates, concluding that they are significantly different when they do not overlap. aData from eating/swallowing and cooking not available for 1994. |
|||
The use of ambulatory aid devices had increased significantly from 1994 to 2014, especially the use of walkers and powered wheelchairs (Table VII). Assistive aids for hands and arms were used more often. In 2014 14% of people were using a ventilator or other respiratory aid, compared with only 2% in 1994.
|
Table VII. Polio patients (%) in need of technical aids in 2014 and 1994 |
|||
|
|
2014 (n = 1,408) Mean (95% CI) |
1994 (n = 1,444) Mean (95% CI) |
p |
|
Orthopaedic aids |
68 (66–70) |
63 (61–65) |
* |
|
Walker |
58 (55–61) |
4 (3–5) |
* |
|
Electric wheelchair |
32 (30–34) |
11 (9–13) |
* |
|
Manual wheelchair |
29 (27–31) |
20 (18–22) |
* |
|
Assistive aids for hands/arms |
17 (15–19) |
8 (7–9) |
* |
|
Ventilator or other respiratory aid |
14 (12–16) |
2 (1–3) |
* |
|
*Significance was set at 0.05 after calculating the 95% confidence interval (CI) for the 2 estimates, concluding that they are significantly different when they do not overlap. |
|||
Other health problems
Muscle and joint pain and cold intolerance were the most frequently reported health problems in the polio population, both in 2014 and 1994, with a marked increase during the 20-year period (Table VIII). Insomnia also increased, while daytime sleepiness, although frequent, did not change. Concentration problems and headache did not increase, while general exhaustion showed a marked reduction in the 20-year period. In 2014 the subjective reported that the level of experienced fatigue, measured by Fatigue Severity Scale (FSS), was median 4,9 (SD 1.5) with an interquartile range of 2.2 (mean 4.8 (SD 1.5)), and a non-significant difference between sex.
|
Table VIII. Frequency (%) of health problems reported by polio survivors in 2014 and 1994 |
|||
|
|
2014 (n = 1,408) Mean (95% CI) |
1994 (n = 1,444) Mean (95% CI) |
p |
|
Muscle and joint pain |
85 (83–87) |
73 (71–75) |
* |
|
Cold intolerance |
74 (72–76) |
62 (60–65) |
* |
|
Insomnia |
64 (62–67) |
38 (36–41) |
* |
|
Swelling of legs and feet |
50 (47–53) |
43 (41–46) |
* |
|
Breathing problems |
|
|
|
|
After physical exertion |
40 (37–43) |
41 (38–43) |
|
|
At rest |
14 (12–16) |
16 (14–18) |
|
|
Daytime sleepiness |
42 (39–45) |
41(39–44) |
|
|
Self-reported general exhaustion |
42 (39–45) |
59 (57–62) |
* |
|
Concentration problems |
36 (34–39) |
39 (37–42) |
|
|
Headache |
30 (28–32) |
33 (31–35) |
|
|
Fasciculation/muscle cramps |
60 |
|
|
|
Voice change |
21 (19–23) |
15 (19–23) |
|
|
Swallowing problems |
15 (13–19) |
5 (4–6) |
|
|
*Significance was set at 0.05 after calculating the 95% confidence interval (CI) for the 2 estimates, concluding that they are significantly different when they do not overlap. |
|||
Nearly one-third of the polio population (28%) reported that they seldom or never exercised, while half reported performing physical activity for more than 30 min at least 3 times a week. Only 12% were daily smokers in 2014, compared with 27% in 1994.
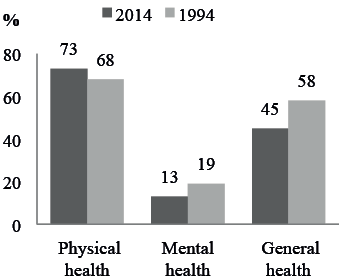
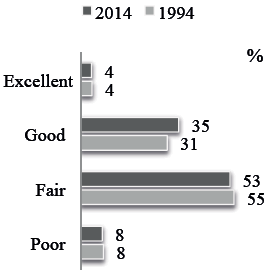
The rating of experienced deterioration of physical, mental and general health condition during recent years in 2014 and 1994 is illustrated in Fig. 2, whereas Fig. 3 shows the self-reported general health condition. The results were remarkably similar in 1994 and 2014, with no obvious deterioration.
DISCUSSION
The surprising finding from the present study was that the 2014 polio population reported only minor subjective worsening of their health situation compared with the 1994 polio cohort, even though the mean age had increased from 57 to 70 years. However, over 90% of both men and women reported distinct new muscular weakness, appearing many years after the acute polio, especially in muscles previously known to be affected by polio, but also in muscles previously thought to be unaffected. This is an even higher frequency of new weakness than reported previously (3, 23–25). Furthermore, half of the patients reported loss of muscle size or volume in 2014, a 15% increase since 1994, with no sex difference. The mean age for onset of new atrophy and paresis was between 46 and 51 years, i.e. more than 20 years earlier.
Since it has not been common to examine clinically unaffected muscles with neuromuscular methods, such as electromyography (EMG), neither patient nor physicians were able to determine if a muscle was, in fact, unaffected. Therefore, new muscular weakness in muscles previously thought to be unaffected might be an anticipated deterioration.
Our study indicates that, although post-polio represents an ongoing process in most patients, the deterioration occurs slowly and with less consequence for general health and ADL than previously thought.
The subjects’ perceived health condition was almost identical in 2014 and 1994. However, the 2014 study population reported more respiratory aids, insomnia, swelling of legs and feet, cold intolerance, and swallowing problems, than those participating in 1994, illustrating the ongoing loss of motor neurones in post-polio. The use of ventilators or other respiratory aids had increased in 2014, reflecting an increase in breathing problems, and probably also increased awareness of/and recent technical developments, especially regarding non-invasive ventilation (30).
The reported use of aid devices, especially ambulatory devices, reflects the severity of impairment and disability (31). The use of orthopaedic aids and assistive devices increased significantly from 1994 to 2014, particularly the use of walkers and powered wheelchairs, confirming previous findings (22). The increase in use of walkers might reflect a shift in attitude towards aid devices, and less use of canes and crutches. The same might be true for wheelchairs, especially electrical, and el-scooters, which are used as effective energy-saving devices by many polio patients. Climbing stairs was the most difficult ADL, and the need for assistance doubled from 1994 to 2014, illustrating the deterioration in muscular weakness.
Surprisingly, there was no change in the need for personal assistance to manage personal hygiene or other ADL over the 20-year period. Such tasks probably depend less on pure muscle strength. In fact, fewer people reported a need for assistance with household chores in 2014, in accordance with recent studies, which found only minor changes in disability and no increase in ADL dependency over a 4-year period (31, 32).
Our results indicate that the elderly polio population had adapted better to their life situation at the mean age of 70 years, than at 57 years. It is known from the literature that older people are more satisfied than younger people with certain aspects of life. However, the difference is striking, and we believe that the main reason is that polio survivors have made lifestyle changes and adapted to the late effects, for the majority occurring more than 20 years earlier. This is also reflected in the fact that in 1994 67% lived in detached houses or villas, while this was reduced to 56% in 2014, and that the vast majority now are on disability pensions or retired.
The survey revealed that there is most likely underuse of technical aids and support from the healthcare system in the elderly polio population. More than half lived in homes without special arrangements for disability. Even if the number using assistive aids for hands and arms increased from 8% to 17% over the 20-year period, this seems inadequate, bearing in mind that 61% experienced weakness in the arms and hands. Similarly, despite an increase in the need for personal assistance with activities such as climbing stairs, and in the use of assistive devices, 83% of respondents reported that they had no support with home care or nursing services.
The current study showed increasing pain in the polio group, especially muscle and joint pain, and the majority of respondents reported that pain hampered them in their everyday life. Pain was similar across all age cohorts of polio subjects and thus should not be attributed to the process of ageing (33, 34). Self-reported pain intensity and distribution have been shown to correlate with perceived general muscle strength and function (35).
Female sex has been suggested as a risk factor for developing post-polio (36), and in our study more women than men experienced new weakness in polio muscles. In addition, 1 of the major health problems in the polio population, osteoarthritis, showed a marked sex difference; nearly twice as many women as men reported osteoarthritis. Osteoporosis and fibromyalgia, similarly, were more common in females. Sex should be considered when evaluating health problems in the polio population.
Regarding fatigue, a mean score of 4.8 was found in the study group. Compared with other Norwegian samples, the scores have decreased, with mean scores for fatique decreasing from 5.6 in a 1997 sample, to 5.2 in a 2001 sample (15, 16). According to Lerdal et al. (37) the cut-off score of clinically significant fatigue in the general population should be above 5, as 46.7% of the Norwegian population scored > 4.0.
Nearly one-third of the polio population reported that they seldom or never exercised, while another third reported performing regular activity for more than 30 min 3 times a week, and 15% reported such activities more than 3 times a week. Physical function and activity has been shown to correlate with quality of life for polio subjects (38). Despite progressive physical disability, most people with late effects of polio are physically active and much of this activity is performed as part of occupational or household tasks and not as traditional exercise (39). The level of physical activity among polio subjects must be evaluated as satisfactory compared with the level among healthy elderly people.
Study limitations
The current study is based on a questionnaire, and the results are based on self-reporting. Comparisons with the situation 20 years ago are virtually impossible for individual patients, especially regarding muscle strength and volume. Even if questionnaire-based studies have limitations, they usually show high validity for the type of questions used in our study. Also, we have the advantage of quantifying the answers from a large group of polio survivors and comparing them with similar questions in a previous study. We are aware that these groups are only partially overlapping, since we have no data on the number of patients participating in both the 1994 and the 2014 studies, and that one should take this into consideration when calculating significance. However, we find the results interesting, and believe our relatively cautious conclusions are justified.
The questionnaire was sent to members of the Norwegian Polio Association (LFPS) on both occasions, but only 32% positively remembered having participated in 1994. However, the correct number of participants on both occasions was probably much higher. One of the reasons for a low participation in both studies could be change in membership. However, it is not possible to establish the reason for this, since LFPS does not keep records of reasons for not renewing membership. Furthermore, it seems fair to estimate that another reason is death, as 177 members (13%) of LFPS were reported to have died in the period. A recent Swedish follow-up study from 1995 and 2012 of 270 polio-patients showed that only 116 persons (40%) were still alive after 17 years. The patients who had died in the period had a mean age of 70 years in 1995 (40).
Strengths of our study are the high number of participants and the 72% response rate, supporting the representativeness of the study. Adding another 175 polio patients from advertising and via the South-Eastern Norway Health Authority should increase representativeness, as these patients were somewhat younger, but otherwise similar to the main group.
The 1994 cohort was found to be representative, as the distribution of year of polio onset was the same in this cohort as in the total Norwegian polio population (27). On the other hand, the prevalence of polio survivors in Norway is estimated to be between 8,000 and 10,000 persons (26, 27). Hence, the representativeness of the approximately 2,000 members of the National Society of Polio Survivors might be contested.
Conclusion
The present study illustrates that the polio population today have more health problems and have an increased need for assistive devices compared with 20 years ago. These findings demonstrate a need for specialized healthcare for polio patients as they age, and the importance of identifying specific subgroups with unmet healthcare needs. However, today’s elderly polio population still report surprisingly high general wellbeing, reflecting adaptation to their disability.
Polio survivors live with a lifelong disability, which may often have complicating factors that can be life-threatening with misdiagnosis or incorrect treatment. They need regular evaluation and treatment to maintain function and ensure necessary healthcare. We recommend that polio survivors are referred to regional centres for specialized examination and treatment in older age.
ACKNOWLEDGEMENTS
The authors would like to thank TNS Gallup, Jonny Nordøy and Audun Fladmoe. Also, the members of the National Society of Polio Survivors, and especially the Pilot group, who have contributed crucially in all phases of this survey.
The authors declare no conflicts of interest.
REFERENCES

