Guy Vanderstraeten, MD1, Thierry Lejeune, MD2, Hubert Piessevaux, MD3, Dirk De Bacquer, PhD4, Chris Walker, PhD5 and Birgit De Beleyr, MPharm6
From the 1Department of Rehabilitation Sciences and Physical Therapy, Faculty of Medicine and Health Sciences, Ghent University Hospital, Ghent, 2Université Catholique de Louvain, Cliniques Universitaires Saint-Luc, Physical Medicine and Rehabilitation Department, Brussels, 3Hepato-Gastroenterology Department, Cliniques Universitaires Saint-Luc, Université Catholique de Louvain, Brussels, 4Department of Public Health, University of Ghent, Belgium, 5Pfizer, Walton Oaks, UK and 6Pfizer, Brussels, Belgium
OBJECTIVE: To evaluate gastrointestinal risk profiles in patients with osteoarthritis who are currently being treated, or who are candidates for treatment, with a non-steroidal anti-inflammatory drug.
METHODS: Patients with osteoarthritis treated by primary care physicians or physical and rehabilitation medicine (PRM) specialists in Belgium and Luxembourg were scored for gastrointestinal risk profile, low, moderate or high, based on the presence of gastrointestinal risk factors. These included advanced age, gastrointestinal history, comorbidities, medication use, smoking, and alcohol consumption. Use of gastro-protective agents (proton pump inhibitors) was also assessed.
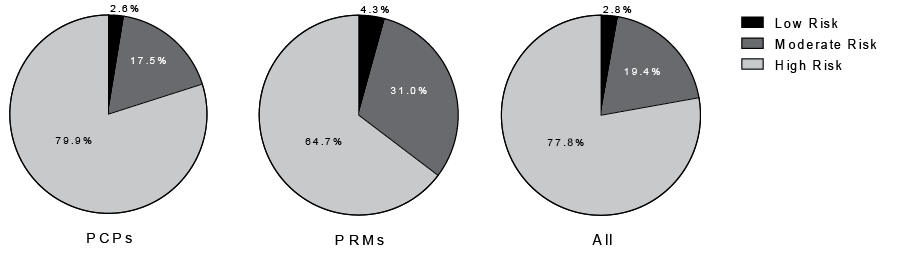
RESULTS: A total of 190 primary care physicians and PRM specialists provided data on 885 patients. A large majority of patients were rated high-risk gastrointestinal (77.8%), with fewer moderate (19.4%) or low (2.8%) risk. The proportion of high-risk patients treated by PRM specialists was significantly lower than that treated by primary care physicians (64.7% vs 79.9%; p < 0.0001). Only 37.0% of high-risk patients received proton pump inhibitors co-prescription with a non-steroidal anti-inflammatory drug.
CONCLUSION: A high prevalence of elevated gastrointestinal risk was found in this survey of patients with osteoarthritis who were current or candidate users of non-steroidal anti-inflammatory drugs. This appears to be insufficiently recognized, as preventative gastro-protective co-treatment was infrequently prescribed. Careful assessment of gastrointestinal risk factors should be made before prescribing non-steroidal anti-inflammatory drugs, with treatment tailored to the patient’s gastrointestinal risk profile.
Key words: gastrointestinal risk; non-steroidal anti-inflammatory drug; osteoarthritis; primary care.
J Rehabil Med 2016; 00: 00–00
Correspondence address: Guy Vanderstraeten, Department of Rehabilitation Sciences and Physical Therapy, Faculty of Medicine and Health Sciences, Ghent University Hospital, De Pintelaan 185, BE-9000, Ghent, Belgium. E-mail: Guy.Vanderstraeten@UGent.be
Accepted May 17, 2016; Epub ahead of print Jun 30, 2016
INTRODUCTION
Osteoarthritis (OA) is among the top 10 causes of disability globally (1) and is the most frequent cause of disability in older age groups (2). There are approximately 135 million individuals with OA worldwide and, as the population ages in most western societies, the condition is becoming more common (3). OA is characterized by pain, stiffness and weakness in the affected joint. Therapeutic intervention is focused on alleviating pain and reducing physical disability via both pharmacological and non-pharmacological approaches (4). Non-steroidal anti-inflammatory drugs (NSAIDs) are widely prescribed for long-term pain relief and inflammation, with guidelines for OA recommending their use after failure of treatment with paracetamol (4–6).
While NSAIDs offer important clinical benefits, adverse events are common and they have been associated with an increased risk of gastrointestinal (GI) complications (in both the upper and lower GI tract) (7, 8), kidney toxicity (9, 10) and an increased risk of cardiovascular outcomes (11). The most frequent toxicities are GI related. These can range from mild dyspepsia, to potentially fatal perforations or haemorrhages in the upper and lower GI tract (12, 13). As mild symptoms provide insufficient warning for serious GI complications (14), it is important to identify factors that are associated with an increased risk of GI events in NSAID users.
A number of these factors have already been identified. The most important of these are: prior history of ulcer complications or symptomatic ulcers (8), and advanced patient age (either ≥ 65 years (13, 15) or ≥ 60 years (16, 17)). Concomitant use of NSAIDs with anti-platelet agents (18), anticoagulants (19), corticosteroids (19) or selective serotonin reuptake inhibitors (SSRIs) (20) has also been associated with an increased risk of GI events. In addition, a number of disease states are associated with increased GI risk in NSAID users, including Helicobacter pylori infection with peptic ulcers (21), and severe rheumatoid arthritis (ACR classification 4) (22) and cardiovascular disease (13). In contrast, a history of dyspepsia has only a modest association with all clinical upper GI events and no association with complicated upper GI events (13). There are also demographic and lifestyle factors, independent of the use of NSAIDs, that could contribute to GI risk, namely male sex, excessive alcohol consumption and smoking (15).
This non-interventional, real-life study aimed to measure all these factors in order to evaluate the GI risk profiles in patients with OA who were either currently being treated with an NSAID or were candidates for NSAID treatment, in Belgium or Luxembourg. Patients were referred by either primary care physicians (PCPs) or secondary care physicians (physical and rehabilitation medicine specialists (PRMs)).
METHODS
Study population and design
This was a non-interventional cross-sectional study including men and women aged ≥ 18 years with a clinical diagnosis of OA who were currently treated with an NSAID or who were a candidate for NSAID therapy. Candidates for NSAID therapy were determined by the investigator. Patients were currently being treated in everyday practice by a PCP or PRMs in Belgium or Luxembourg. The only exclusion criteria were pregnancy or breast-feeding.
Patient information was collected between September 2011 and August 2012. A total of 160 PCPs and 30 PRMs from Belgium and Luxembourg provided data on 885 eligible patients. Patients were from both the Dutch- and French-speaking parts of Belgium, and from Luxembourg. The first OA patient of each working day was enrolled by each physician. Patient demographic and clinical information were collected at the time of the single study visit. Patient information included age, smoking status, alcohol consumption, comorbidities, GI history and current medication use.
All patients provided written informed consent, and the study was conducted in accordance with the International Society for Pharmacoepidemiology and International Society for Pharmacoeconomics and Outcomes Research guidelines. Ethics approval was obtained from the relevant Institutional Review Board or Independent Ethics Committee by each investigator.
Outcome measures and gastrointestinal risk classification
The primary objective of the study was to evaluate the GI risk profiles (8, 13) of patients and to stratify them into low, moderate and high risk. Assessment of the GI risk profile of each patient was conducted by populating the study case report form and assigning the GI risk profile based on predefined criteria (Table I). Patients were designated as: GI “low risk” if ≤ 1 Level A risk factor was present; GI “moderate risk” if 1 or 2 Level B risk factors, or 2 Level A risk factors were present; and GI “high risk” if ≥ 1 Level C risk factor, or ≥ 3 Level A or Level B risk factors were present.
Secondary objectives of the study were to assess: the prevalence of GI risk factors in patients; the difference in GI risk profiles in patients being treated by a PCP compared with those treated by a PRM; and the proportion of patients being concomitantly treated with an NSAID and a proton pump inhibitor (PPI) and if this positively correlates with the level of GI risk
|
Table I. Definition of gastrointestinal risk profiles |
|
|
Level A risk factors History of dyspepsia Male sex Presence of Helicobacter pylori infection Excessive alcohol use |
Low risk ≤ 1 Level A factor present |
|
Level B risk factors History of symptomatic GI ulcer Age > 60 years Co-morbidities (rheumatoid arthritis, cardiovascular disease, diabetes mellitus, cerebrovascular disease) Smoker Use of NSAID (including high-dose aspirin or combination of multiple NSAIDs) Use of corticosteroids Use of SSRI Use of oral bisphosphonates |
Moderate risk 1 or 2 Level B risk factors present or, 2 Level A risk factors present |
|
Level C risk factors History of complicated GI ulcer Use of concurrent anticoagulants/antiplatelet (or low-dose aspirin) therapy and NSAIDs |
High risk ≥ 1 Level C risk factor present or, ≥ 3 Level A or Level B risk factors present |
|
NSAID: non-steroidal anti-inflammatory drug; SSRI: selective serotonin re-uptake inhibitor; GI: gastrointestinal. |
|
Statistical analysis
Sample size calculations revealed that recruitment of 800 patients from Belgian PCPs and 400 patients from Belgian PRMs were needed to estimate the distribution of GI profiles with a precision of at least 5% and a confidence interval of 95%. These numbers would allow a comparison of GI risk profiles between primary care and specialist practices with 80% statistical power. In addition, a further 100 patients were to be recruited from PCPs from Luxembourg. Following changes to legislation governing clinical studies in Belgium, which limited the recruitment of patients in that country, the recruitment goal was increased to 200 patients from Luxembourg. The final sample size was also reduced as recruited patients who did not meet the inclusion criteria were excluded from the data-set.
Differences in the distribution of GI risk profiles were assessed for statistical significance by 2-sided Fisher’s exact test.
RESULTS
Patient population and characteristics
A total of 160 PCPs and 30 PRMs provided data on 754 and 131 eligible patients, respectively. Patients were equally distributed by healthcare provider from Dutch-speaking (429 from PCPs; 93 from PRMs) and French-speaking (175 from PCPs; 38 from PRMs) parts of Belgium. Patients from Luxembourg were all from PCPs (n = 150). The demographic characteristics of the patient population are shown in Table II, with patients attending PRMs being of younger mean age than those attending PCPs (61.7 vs 66.9 years).
|
Table II. Patient demographics by healthcare provider |
|||
|
|
PCPs |
PRMs |
All |
|
Sex, % (n/N) |
|||
|
Female |
62.4 (470/753) |
69.5 (91/131) |
63.5 (561/884) |
|
Male |
37.6 (283/753) |
30.5 (40/131) |
36.5 (323/884) |
|
Age (years)a |
|
|
|
|
< 40, % (n/N) |
2.5 (19/748) |
7.0 (9/129) |
3.2 (28/877) |
|
40–49, % (n/N) |
7.6 (57/748) |
11.6 (15/129) |
8.2 (72/887) |
|
50–59, % (n/N) |
15.2 (114/748) |
27.1 (35/129) |
17.0 (149/887) |
|
60–69, % (n/N) |
27.8 (208/748) |
18.6 (24/129) |
26.4 (232/887) |
|
70–79, % (n/N) |
30.2 (226/748) |
25.6 (33/129) |
29.5 (259/887) |
|
≥ 80, % (n/N) |
16.6 (124/748) |
10.1 (13/129) |
15.6 (137/887) |
|
Mean (SD) |
66.9 (12.7) |
61.7 (13.8) |
66.1 (13.0) |
|
Smoking status, % (n/N) |
|||
|
Smoker |
19.9 (149/748) |
18.9 (24/127) |
19.8 (173/875) |
|
Ex-smoker |
18.7 (140/748) |
22.0 (28/127) |
19.2 (168/875) |
|
Non-smoker |
61.4 (459/748) |
59.1 (75/127) |
61.0 (534/875) |
|
Excessive alcohol useb, % (n/N) |
20.9 (148/708) |
11.0 (14/127) |
19.4 (162/835) |
|
aAge at time of inclusion in the study. b> 2 units/day for females and > 3 units/day for males. PCPs: primary care providers; PRMs: physical and rehabilitation medicine specialists. |
|||
The most common co-morbidities in patients were hypertension and cardiovascular disease, with patients treated by PRMs tending be less likely to have many comorbidities (Table III). While Helicobacter pylori infection was known to be present in 9.3% of patients, this information was missing in a large proportion (56.4%) of patients. The majority of patients (71.0%) were currently receiving NSAIDs; more than half (50.6%) for ≥ 30 days. A notably high proportion of patients (21.0%) used an over-the-counter (OTC) medication for their OA. Patients treated by PRMs were less likely to be currently receiving NSAIDs, but more likely to be receiving corticosteroids or an SSRI (Table III).
|
Table III. Patient clinical characteristics and medication use by healthcare provider |
|||
|
|
PCPs % (n/N) |
PRMs % (n/N) |
All % (n/N) |
|
Comorbidities |
|
|
|
|
Rheumatoid arthritis |
5.5 (41/749) |
0.8 (1/129) |
4.8 (42/878) |
|
Diabetes mellitus |
16.8 (126/749) |
10.8 (14/129) |
16.0 (140/878) |
|
Cardiovascular disease |
26.7 (200/749) |
10.1 (13/129) |
24.3 (213/878) |
|
Cerebrovascular disease |
6.3 (47/749) |
3.1 (4/129) |
5.8 (51/878) |
|
Hypertensiona |
66.8 (482/722) |
61.5 (75/122) |
66.0 (557/844) |
|
Other |
15.2 (114/749) |
15.5 (20/129) |
15.3 (134/878) |
|
Gastrointestinal history |
|
|
|
|
Symptomatic GI ulcer |
18.3 (136/745) |
17.2 (22/128) |
18.1 (158/873) |
|
Complicated GI ulcer |
3.2 (24/746) |
2.3 (3/128) |
3.1 (27/874) |
|
Dyspepsia |
52.6 (390/742) |
41.2 (54/131) |
50.9 (444/873) |
|
Helicobacter pylori infection |
9.0 (30/332) |
11.1 (6/54) |
9.3 (36/386) |
|
Medication use |
|
|
|
|
Current NSAID |
72.1 (520/721) |
64.2 (79/123) |
71.0 (599/844) |
|
Combination of NSAIDs |
4.7 (35/744) |
3.8 (5/131) |
4.6 (40/875) |
|
NSAID ≥ 30 days |
52.6 (388/737) |
39.2 (51/130) |
50.6 (439/867) |
|
Corticosteroids (systemic) |
5.7 (43/750) |
9.9 (13/131) |
6.4 (56/881) |
|
SSRI |
16.4 (123/751) |
20.6 (26/126) |
17.0 (149/877) |
|
Aspirin |
33.7 (253/751) |
15.5 (20/129) |
31.0 (273/880) |
|
Aspirin high dose (> 100 mg) |
3.4 (8/236) |
16.7 (3/18) |
4.3 (11/254) |
|
Anticoagulants |
6.0 (45/753) |
6.2 (8/130) |
6.0 (53/883) |
|
Anti-platelets |
6.7 (50/750) |
6.2 (8/128) |
6.6 (58/878) |
|
OTC medication for OAb |
20.9 (144/689) |
21.8 (27/124) |
21.0 (171/813) |
|
Oral bisphosphates |
13.2 (99/750) |
7.1 (9/127) |
12.3 (108/877) |
|
PPI |
43.9 (330/751) |
43.0 (55/128) |
43.8 (385/879) |
|
aSystolic/diastolic blood pressure ≥ 140/90 mmHg and/or using anti-hypertensive medication. bType of OTC medication was not recorded, but may include medications such as paracetamol, ibuprofen, glucosamine or aspirin. NSAID: non-steroidal anti-inflammatory drug; OTC: over-the-counter; PCPs: primary care providers; PRMs: physical and rehabilitation medicine specialists; SSRI: selective serotonin re-uptake inhibitor. |
|||
Gastrointestinal risk profile
The large majority of patients were designated high GI risk (Fig. 1). There was a significant difference in GI risk profile by healthcare provider (p < 0.0001), with patients treated by PRMs less likely to be high risk than those treated by PCPs. The GI risk profile also varied by age, with 70.7% (319/451) of patients aged < 70 years designated high risk, compared with 86.4% (306/354) of patients aged ≥ 70 years. The difference between patients treated by PRMs or PCPs was more pronounced in patients < 70 years, with 51.3% (39/76) and 74.7% (280/375) high risk, respectively. In patients ≥ 70 years, this difference was not apparent (PRMs, 89.7% [35/39]; PCPs, 86.0% [271/315]), although the number of patients ≥ 70 years treated by PRMs was low. There was no difference in GI risk profile by recruitment region (French-speaking Belgium, Dutch-speaking Belgium and Luxembourg) (p = 0.86).
Both current users of NSAIDs (72.1%; 581/806) and candidates for NSAID treatment 27.9%; 225/806) were well represented in this study population. The majority of patients who were candidates for NSAID treatment were rated high GI risk (62.2%; 140/225), with smaller proportions of moderate (27.6%; 62/225) and low (10.2%; 23/225) risk. This was lower than the proportion of current users of NSAIDs who were high GI risk (83.6%; 486/581). The proportion of current users of NSAIDs who were GI moderate and low risk was 16.4% (95/581) and 0.0% (0/581), respectively. The difference in GI risk profile between current users of NSAIDs and candidates for NSAID treatment was statistically significant (p < 0.0001).
Use of combinations of medications relevant to gastrointestinal risk
Over 10% of patients, from both PCPs and PRMs, were treated with NSAIDs together with a SSRI (Table IV), despite the fact that this combination is known to increase GI risk (23). In addition, only 37.0% of patients in the GI high-risk group were treated with concomitant NSAID and PPI, with lower proportions in patients with a lower GI risk profile (Fig. 2).
|
Table IV. Use of combinations of medications relevant to gastrointestinal risk |
|||
|
|
PCPs % (n/N) |
PRMs % (n/N) |
All % (n/N) |
|
PPI & NSAID |
32.9 (236/718) |
24.8 (30/121) |
31.7 (266/839) |
|
PPI & antiplatelet, anticoagulant or aspirin |
18.5 (139/751) |
13.4 (17/127) |
17.8 (156/878) |
|
NSAID & antiplatelet, anticoagulant or aspirin |
28.2 (203/720) |
17.2 (21/122) |
26.6 (224/842) |
|
NSAID & SSRI |
11.7 (84/718) |
10.9 (13/119) |
11.6 (97/837) |
|
NSAID: non-steroidal anti-inflammatory drug; PCPs: primary care providers; PPI: proton pump inhibitor; PRMs: physical and rehabilitation medicine specialists; SSRI: selective serotonin re-uptake inhibitor. |
|||

Fig. 2. Concomitant use of proton pump inhibitors (PPI) and non-steroidal anti-inflammatory drug (NSAID) by gastrointestinal risk profile and healthcare provider. PCPs: primary care providers; PRMs: physical and rehabilitation medicine specialists.
There were notable differences between patients who did, and did not, receive a PPI (Table V). These differences were most apparent in GI history (patients with a history of ulcers or dyspepsia being more likely to use a PPI) and concomitant use of an SSRI (with these patients being more likely to use a PPI).
|
Table V. Proton pump inhibitor use by patient demographic and clinical characteristics |
||
|
|
Use of PPI |
|
|
No % (n/N) |
Yes % (n/N) |
|
|
Healthcare provider is SP |
14.8 (73/494) |
14.3 (55/385) |
|
Male sex |
40.4 (199/493) |
32.0 (123/385) |
|
Current smoker |
19.5 (95/488) |
18.9 (72/381) |
|
Excessive alcohol usea |
19.4 (91/468) |
19.1 (69/361) |
|
Comorbidities |
|
|
|
Rheumatoid arthritis |
3.3 (16/490) |
6.8 (26/382) |
|
Diabetes mellitus |
14.5 (71/490) |
18.1 (69/382) |
|
Cardiovascular disease |
21.8 (107/490) |
27.8 (106/382) |
|
Cerebrovascular disease |
4.1 (20/490) |
8.1 (31/382) |
|
Hypertensionb |
64.3 (301/468) |
68.3 (254/372) |
|
Other |
12.4 (61/490) |
18.6 (71/382) |
|
Gastrointestinal history |
|
|
|
Symptomatic GI ulcer |
6.9 (34/490) |
32.9 (124/377) |
|
Complicated GI ulcer |
1.2 (6/491) |
5.6 (21/377) |
|
Dyspepsia |
32.0 (156/488) |
75.5 (286/379) |
|
Helicobacter pylori infection |
7.1 (11/155) |
10.8 (25/231) |
|
Use of SSRI |
11.4 (56/491) |
24.1 (92/382) |
|
a> 2 units/day for females and > 3 units/day for males. bSystolic/diastolic blood pressure ≥ 140/90 mmHg and/or using anti-hypertensive medication. SSRI: selective serotonin re-uptake inhibitor; PPI: proton pump inhibitor. |
||
DISCUSSION
In this population of patients with OA from Belgium and Luxembourg there was a very high prevalence of GI risk factors, both in patients seen by PCPs and by PRMs. Overall, 77.8% of patients were identified as high GI risk. These patients either had a history of complicated GI ulcer and/or were receiving anticoagulants/anti-platelets concurrent with NSAIDs, or they had ≥ 3 of the other GI risk factors (see Table I). There was no difference in GI risk profile across the different recruitment regions of this study.
There were differences between patients treated by PCPs and those treated by PRMs. Patients treated by PRMs were significantly less likely to be designated high-risk GI than those treated by PCPs (p < 0.0001). Patients treated by PRMs were notably younger than those treated by PCPs (mean 61.7 compared with 66.9 years), with 45.7% of patients treated by PRMs being <60 years of age compared with 25.3% of patients treated by PCPs. Patients treated by PRMs were also less likely to have comorbidities, such as rheumatoid arthritis (with these patients typically treated by specialist rheumatologists in Belgium), diabetes mellitus, and cardiovascular and cerebrovascular disease. PRMs in Belgium and Luxembourg tend to treat younger patients with more severe OA and, with higher age (> 60 years) and comorbidities being significant GI risk factors, this difference in risk profiles was not unexpected. Although, it is possible that some PRMs may have a lesser knowledge of their patient’s medical history, compared with PCPs, which could have contributed to the fewer comorbidities recorded in these patients.
In this study, over 95% of patients (97.2%) were classified as being of moderate or high GI risk, which is broadly comparable with the findings of a similar study conducted by rheumatologists in Spain (24). In the Spanish LOGICA study, 86.6% of patients displayed ≥ 1 GI risk factor and were designated as moderate or high GI risk (24). The most common individual GI risk factor in the LOGICA study, as in this study, was advanced patient age (≥ 60 years) (24). In another earlier study, conducted in the Canadian healthcare system, a slightly less exhaustive list of GI risk factors, including patient age ≥ 65 years, produced a more conservative result; with only 61.3% of patients classified as having ≥ 1 GI risk factor (25).
While all patients in this study were, at the least, candidates for NSAID therapy, 71.0% were currently being treated with an NSAID. This was lower than the proportion currently being treated with an NSAID in the LOGICA study (82.5%) (24). At the same time, the proportion of patients treated with an NSAID and a gastro-protective agent concomitantly in this study (31.7%) was greater than in the LOGICA study (25.4%) (24). A total of 21.0% of all patients were using an OTC medication for OA. This may have included the use of ibuprofen, which is available OTC in Belgium and Luxembourg and, despite also being an NSAID, may not always have been included in the 71.0% of patients reported as currently being treated with an NSAID. At the same time, 4.6% of patients were taking a combination of NSAIDs. This may have included a combination of an oral and a topical NSAID or of a prescribed and an OTC NSAID. The use of 2 oral NSAIDs increases GI risk and healthcare providers should question patients on any OTC medications they are using prior to prescribing an oral NSAID.
It was particularly notable that a minority of moderate and high GI risk patients in this study were being treated concomitantly with an NSAID and a PPI (19.5% and 37.0%, respectively). This was surprisingly low, given that both European (4) and international (5) guidelines on the treatment of patients with OA suggest that patients who are at increased risk of GI harm should be treated with either an NSAID together with a gastro-protective agent (such as a PPI), or a COX-2 selective inhibitor. It may be that some of the patients in this study were treated with a COX-2 selective inhibitor, but the proportion with concomitant NSAID and PPI treatment was still lower than we would have expected. In addition, the overall proportion of patients using a PPI (43.8%) was higher than the proportion using a PPI together with an NSAID (31.7%). This discrepancy is probably a result of many individuals in Belgium and Luxembourg being treated with a PPI for gastro-oesophageal reflux.
Given the high prevalence of GI risk factors in patients with OA, safer treatment approaches, such as COX-2 selective inhibitors or combinations of traditional NSAIDs with PPIs, are indicated by guidelines and clinical data (4, 5, 26). The results of this study are consistent with past studies that have suggested that PPIs are underutilized as a gastro-protective therapy in patients with higher GI risk treated with NSAIDs (7, 27, 28). Healthcare providers treating patients with OA should perform a GI risk assessment before prescribing an NSAID and, in patients with higher GI risk, prescribe either a concomitant PPI or a COX-2 selective inhibitor. Helicobacter pylori infection status was unknown in over 50% of the patients in this study, but long-term use of a PPI and active Helicobacter pylori infection is associated with increased gastric inflammation and it has been recommended that patients be tested for infection, and the infection eradicated, before starting long-term PPI therapy (29).
A notable limitation of this study was that the total number of patients enrolled was lower than the projected numbers desired. In particular, the proportion of patients enrolled from PRMs (131 of 884 total patients; 15.8%) was lower than the proportion projected (400 of 1,300; 30.8%). The study did reveal key differences between PRMs and PCPs in patient demographics and GI risk profile. However, larger numbers of patients from PRMs may have provided a clearer indication of whether or not PRMs were less (or more) likely than PCPs to prescribe PPIs together with NSAIDs in patients with higher GI risk. Furthermore, when recording NSAID use, the study did not differentiate between non-selective NSAIDs and COX-2 selective inhibitors, although based on prescription patterns and previous studies it was assumed that the majority of patients were treated with a non-selective NSAID (24).
This study was also limited by being based on information gathered at a single visit. While this enabled the study to remain simple and focused on the key research questions, it also resulted in limitations on how much detail was gathered on each patient’s medical history. For example, a large proportion of patients (24.3%) had comorbid cardiovascular disease, but the type, or degree, of disease was not recorded. The assignment of GI risk profiles in this study was based on the presence of a number of risk factors. While the majority of these are well-established, the use of oral bisphosphonates has perhaps not been as well-documented. Nevertheless, oral bisphosphonate use can directly result in GI intolerance (30), and has also been associated with increased GI risk, both alone (31), and in combination with NSAIDs (32).
This study reveals that many patients with OA in Belgium and Luxembourg have significant GI risk. Together with data from prior studies in other countries, a clear picture emerges in which the potential harms of NSAID use in the ageing population that often presents with OA are significantly underestimated. Many patients with OA are at increased GI risk and, as such, healthcare providers should always perform a GI risk assessment prior to prescribing an NSAID.
ACKNOWLEDGEMENTS
We thank all physicians and patients who participated in this study. This study was sponsored by Pfizer, which had no influence on the interpretation of data and the final conclusions drawn. GV, TL, HP, and DDB have no relevant financial disclosures. CW and BDB are employees of Pfizer and hold stock options with Pfizer. Medical writing support was provided by Joshua Fink, PhD, of Engage Scientific Solutions, and funded by Pfizer.
REFERENCES

