
From the 1Department of Rehabilitation, Academic Medical Center, University of Amsterdam, Amsterdam, 2Rehabilitation Medical Center Groot Klimmendaal, Arnhem, 3Expert Centre for Chronic Fatigue, Radboud University Medical Centre, Nijmegen, and 4Department of Rehabilitation, Radboud University Medical Centre, Nijmegen, The Netherlands
Background: Cognitive behavioural therapy does not reduce fatigue in post-polio syndrome, but is effective in facioscapulohumeral dystrophy. This difference in efficacy might be explained by a different role of cognitions in these conditions.
Objective: To compare fatigue-related cognitions between patients with post-polio syndrome and facio-scapulohumeral dystrophy.
Subjects: Patients with post-polio syndrome (n = 21) and facioscapulohumeral dystrophy (n = 24) allocated to a cognitive behavioural therapy intervention in 2 identical trials.
Methods: Assessed cognitions included: sense of control over fatigue; catastrophizing; acceptance; focusing on fatigue; and perceived social support. Group
differences in cognitions (independent t-tests or Mann–Whitney U tests) and group differences in the association of cognitions with fatigue (linear regression models) were studied.
Results: No differences in cognitions were found between the 2 groups (p > 0.18). Furthermore, there were no cognition-by-group interaction effects, except for “perceived social support”, for which a different association with fatigue was found between the 2 groups (p = 0.01). However, univariate models revealed no associations per group.
Conclusion: Fatigue-related cognitions in severely fatigued patients with post-polio syndrome are not clearly different from those in facioscapulohumeral dystrophy. Thus, the lack of efficacy of cognitive behavioural therapy in post-polio syndrome cannot be attributed to unique cognitive characteristics of this population.
Key words: cognitive therapy; cognition; facioscapulohumeral muscular dystrophy; fatigue; post-poliomyelitis syndrome.
Accepted May 11, 2017; Epub ahead of print Jun 28, 2017
J Rehabil Med 2017; 49: 585–590
Correspondence address: Fieke S. Koopman, Department of Rehabilitation, Academic Medical Centre, University of Amsterdam, P.O. 22660, NL-1100 DD Amsterdam, The Netherlands. E-mail: s.koopman@amcu.uva.nl
Post-polio syndrome (PPS) is highly prevalent among the ageing population of polio survivors, affecting between 15% and 80% of all patients with previous paralytic polio (1). Given the large number of polio survivors worldwide (2), PPS is currently one of the most common motor neurone diseases.
Fatigue is a frequent complaint in people with PPS (3–5). In a study on disability and health problems in 76 Dutch patients with PPS, 78% of the subjects reported fatigue as their main problem, exceeding difficulties in walking outdoors (45%), climbing stairs (41%) and pain (39%) (6). Moreover, compared with healthy individuals, patients with PPS experienced much higher levels of fatigue (7, 8), which was shown to contribute considerably to reduced functioning and health-related quality of life (HRQoL) (9, 10).
Fatigue in PPS is considered a multidimensional phenomenon. Earlier studies have shown that biological, physical and psychological factors are associated with this fatigue (11, 12). Given this multidimensional character, a variety of interventions aimed at alleviating fatigue have been studied. These include both pharmacological and non-pharmacological interventions, such as exercise therapy, (online) fatigue management, transcranial direct current stimulation, and multidisciplinary rehabilitation. However, due to a lack of high-quality randomized controlled trials, no definite conclusions on the effectiveness of the above-mentioned interventions can be made (13).
We recently reported the results of a randomized controlled trial on the efficacy of cognitive behavioural therapy (CBT) in severely fatigued patients with PPS. In this study, no decrease in fatigue was found (14), despite the effectiveness of this intervention in reducing fatigue in various other patient populations (15–17). A recent trial investigating the effect of CBT in facioscapulohumeral dystrophy (FSHD), found a clinically relevant decline in fatigue after this intervention (18).
The lack of efficacy of CBT in PPS compared with FSHD, change in fatigue score on the subscale fatigue severity of the Checklist Individual Strength (CIS): +1.87 vs –13.3, respectively, may be linked to the role of fatigue-related cognitions. Effective CBT interventions for reducing fatigue are based on models of perpetuating factors for fatigue, which follow growing evidence that a patient’s cognitions and behaviour are related to fatigue (19). Also, in diseases characterized by loss of muscle function, it has been shown that cognitive-behavioural factors are associated with fatigue (20), which may be even more important in the persistence of this symptom than the severity of neurological impairment (21). More recent studies demonstrated that changes in cognitive factors, such as an increase in sense of control over fatigue and a reduction in focusing on fatigue symptoms (rather than behavioural changes), are mainly associated with a reduction in fatigue after CBT (22, 23).
Most patients with PPS were affected by acute polio in their first years of life, and usually grew up with residual paresis and deformities. Therefore, these patients have spent a lifetime managing the challenges of living with functional limitations and generally experience long durations of fatigue. As such, it can be hypo-thesized that they have developed different cognitions related to fatigue compared with patient populations with a more gradual symptom onset later on in their lives, such as in FSHD.
This study aimed to investigate cognitions related to fatigue in severely fatigued patients with PPS compared with severely fatigued patients with FSHD. The study tested the hypotheses that fatigue-related cognitions in PPS are different from those in FSHD, and that the association of cognitions with fatigue differs between the 2 conditions. Any such difference might explain the difference in efficacy of CBT between PPS and FSHD.
The data used in this study originate from a multi-centre 3-armed RCT, the Fitness And Cognitive behavioural TherapieS for Fatigue and ACTivities in PPS (FACTS-2-PPS) trial, which is part of a larger research programme investigating the effects of 2 rehabilitation interventions in different neuromuscular disorders (the FACTS-2-NMD programme). In the PPS trial, the efficacy of exercise therapy and of CBT on reducing fatigue and improving activities and HRQoL was compared with usual care in patients with PPS. The study design, the protocol of both interventions, and the main results of the trial are described in previous publications (14, 24). For the present study, data were used from participants who were allocated to the CBT intervention and, as part of this intervention, completed computerized questionnaires measuring fatigue cognitions. These questionnaires were administered to select the appropriate treatment modules in order to customize the CBT intervention to the patients’ personal needs.
The comparison group consisted of patients with FSHD who were allocated to the CBT intervention in a second RCT conducted within the FACTS-2-NMD programme. This RCT, the FACTS-2-FSHD trial (25), was similar to the PPS trial with respect to the study objectives, the measurement protocol and the protocol of the CBT intervention. Moreover, the interventions were carried out in the same centres by the same cognitive behavioural therapists (n = 4), who were highly trained in the protocol.
Participants in the PPS trial and the FSHD trial were recruited from 7 hospitals and rehabilitation centres throughout the Netherlands. In addition, patients with FSHD who were registered in a Dutch neuromuscular database (26) or who participated in a patient support organization were also invited to participate. Medical files were screened for potential eligibility. Patients willing to provide signed consent were evaluated by a physician to check the inclusion and exclusion criteria. Regarding PPS, the diagnosis was based on the criteria of the March of Dimes, which include a gradual or sudden onset of progressive and persistent muscle weakness, or abnormal muscle fatigability after a period of stable neurological function (2). As for FSHD, the diagnosis of FSHD type 1 was confirmed by DNA testing. Major inclusion criteria in both groups were: severe fatigue (CIS ≥ 35) (27) and walking ability with or without a walking aid. Major exclusion criteria were: clinical depression and disabling co-morbidity interfering with the intervention programme. A complete list of in- and exclusion criteria has been provided elsewhere (24, 25). The study protocols of the PPS trial and the FSHD trial were approved by the Medical Ethics Committee of the Academic Medical Centre in Amsterdam and the Radboud University Medical Center in Nijmegen, respectively, and all participating centres granted approval to participate. The RCTs were registered in the Dutch Trial Register (PPS trial: NTR1371; FSHD trial: NTR1447). Written informed consent was obtained from all participants.
Fatigue was measured with the subscale fatigue severity of the CIS (27), which consists of 8 statements regarding fatigue severity as experienced during the previous 2 weeks (I feel tired; Physically I feel exhausted; I feel fit; I feel weak; I feel rested; Physically I feel I am in a bad condition; I get tired very quickly; Physically I feel in a good shape). Participants had to indicate on a 7-point Likert scale (ranging from 1 to 7) to what extent the particular statement applied to them. The total score was calculated as the sum of the responses to the 8 statements. A higher fatigue severity score indicates a higher degree of fatigue. Fatigue severity scores collected at study entry (pre-treatment score) were used in the current study. The CIS fatigue has been shown reliable in polio survivors and patients with FSHD (Cronbach’s alpha: 0.93 and 0.83–0.92, respectively) (18, 28).
Appendix SI gives an overview of the instruments used for the assessment of cognitions related to fatigue, including sense of control over fatigue, catastrophizing, acceptance of the disease, focusing on fatigue symptoms, and perceived social support.
Sense of control over fatigue was measured with the Self-Efficacy Scale (SES) (29). Fatigue-related catastrophizing was measured with the Jacobsen-Fatigue Catastrophizing Scale (J-FCS) (30). This scale has been shown to be reliable in patients with breast cancer and chronic fatigue syndrome (CFS) (Cronbach’s alpha: 0.92 and 0.86, respectively) (30, 31). Pain-related catastrophizing was measured with the Pain Catastrophizing Scale (PCS) (32). The impact of being diagnosed with and treated for the disease was measured with the Impact of Event Scale (IES) (33). This instrument has been shown to be reliable and valid in different samples confronted with various kinds of traumatic incidents (33). Acceptance of the disease was measured with the corresponding subscale of the Illness Cognitions Questionnaire (ICQ acceptance) (34). This subscale is reliable and has been shown to be valid in patients with rheumatoid arthritis and multiple sclerosis (Cronbach’s alpha: 0.90 and 0.91; Pearson’s correlation coefficient: 0.76 and 0.78) (34). Focusing on fatigue symptoms was assessed with the corresponding subscale of the Illness Management Questionnaire (IMQ focusing on symptoms) (35). The IMQ was developed and validated in CFS and showed good internal consistency (Cronbach’s alpha: 0.88) (35). Discrepancies between the received amount of social support and the desired amount of social support were assessed with the Social Support Inventory (SSI discrepancies) (36).
Sociodemographic characteristics, disease characteristics and cognitions of both groups are presented as means (SD) or medians (range) for numerical variables, and as number (%) for categorical variables. Group differences in fatigue-related cognitions were studied using independent t-tests (continuous variables with normal distribution) or Mann–Whitney U tests (continuous variables with non-normal distribution). Associations between cognitions and fatigue were investigated with linear regression analyses. First, univariate associations between cognitions and fatigue were explored for the combined groups. Next, to evaluate group differences in the associations of cognitions with fatigue, multivariable linear regression models were built including cognition, group and the interaction term of cognition-by-group. In case of a significant cognition-by-group interaction effect, the univariate association between the respective cognition and fatigue for each group was investigated. Model assumptions (normality, linearity, homogeneity and independence of random errors) were checked using residual plots. All analyses were performed with SPSS Statistics 21. An alpha level of 0.05 was used for all tests of significance.
In the PPS trial, 23 participants were allocated to CBT. The intervention was not initiated with 5 participants because they did not prioritize fatigue as a treatment goal. Of these 5, for the same reason 2 also did not complete the computerized questionnaires. Therefore, data from 21 participants with PPS were available. Of the 25 participants allocated to CBT in the FSHD trial, the results for 1 participant were not available due to a technical problem with the computerized questionnaires. Therefore, data from 24 participants with FSHD were available.
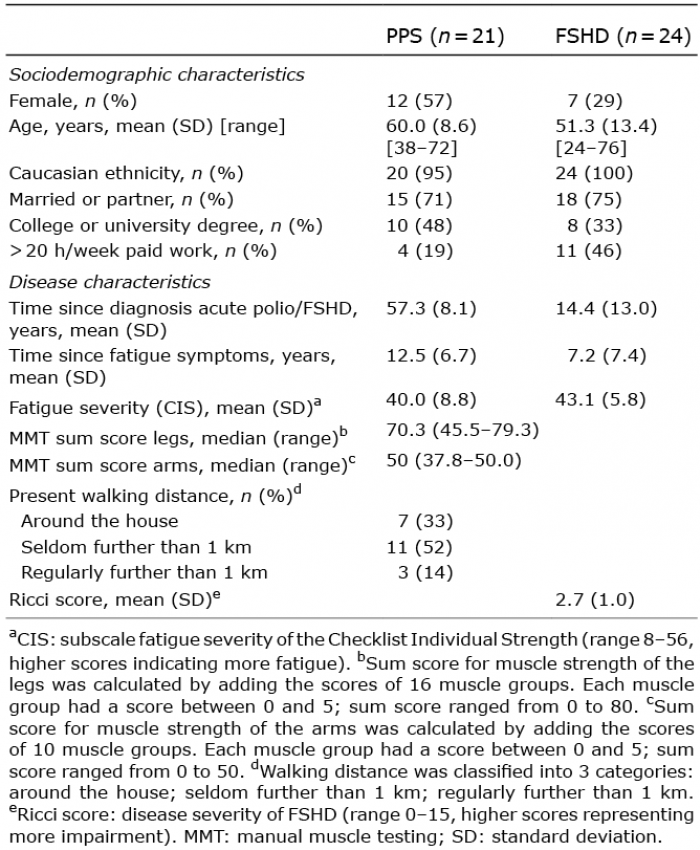
Sociodemographic and disease characteristics of both groups are shown in Table I.
Table I. Sociodemographic and disease characteristics of
patients with post-polio syndrome (PPS) and those with facioscapulohumeral dystrophy (FSHD)
The patients with PPS differed from those with FSHD in that they were older (mean difference: 8.7 years (95% confidence interval (95% CI) 1.8–15.6 years)), had a longer illness duration, defined as time since diagnosis of acute polio/FSHD (mean difference: 42.9 years (95% CI 36.4–49.4 years)), and had a longer duration of fatigue symptoms (mean difference: 5.2 years (95% CI 0.8–9.7 years)). No significant differences were found between the groups with respect to sex, ethnicity, social status, education, employment, and fatigue severity, as measured with the CIS. Also, the number of treatment sessions that participants received did not differ between the groups (median number of treatment sessions 8 (range 1–12) and 5 (range 1–13) for PPS and FSHD, respectively, p = 0.24).
Cognitions related to fatigue in PPS compared with FSHD are shown in Table II. No significant differences in the level of any of the cognitive factors were found between the groups. The results of the univariate and multivariate linear models for the whole group are shown in Table III. None of the models showed a significant cognition-by-group interaction effect, except for the model testing the association of perceived social support and fatigue (β “SSI discrepancies-by-group” = –2.65, SE 1.03, p = 0.01). Univariate models of this association for each group separately showed that there was no significant association (β = 2.03, SE 1.01, p = 0.06 and β = –0.62, SE 0.46, p = 0.19 for PPS and FSHD, respectively).
Table II. Fatigue-related cognitions in post-polio syndrome (PPS) compared with facioscapulohumeral dystrophy (FSHD)
Table III. Univariate and multivariate regression models for
fatigue severity (CIS) for the total group post-polio syndrome (PPS) and facioscapulohumeral dystrophy (FSHD)
Fatigue-related cognitions in severely fatigued patients with PPS were not found to be significantly different from those of severely fatigued patients with FSHD at the time of inclusion in an RCT aimed at alleviating fatigue. Also, no differences in the association of the assessed cognitions with fatigue were found between the 2 groups, except for the cognition perceived social support. As such, the results of this study do not support the hypothesis that patients with PPS develop different cognitions related to fatigue during their lives compared with a patient population with a more gradual symptom onset later in their lives, namely FSHD.
Fatigue-related cognitions in patients with PPS in our study were shown to be similar to those in patients with FSHD, but also to those in other patient populations with a shorter duration of disease symptoms. For example, the mean scores on the factors “fatigue-related catastrophizing” and “focusing on fatigue symptoms” were similar to those in patients with CFS (31, 35). For the factor “acceptance of the disease”, our patients scored in the same range as patients with multiple sclerosis or rheumatoid arthritis (34). Our patients also scored similar levels of distress resulting from traumatic stressors (i.e. the traumatic life event of being diagnosed with or treated for polio and PPS) compared with patients with work-related trauma (33). As such, it is suggested that the role of fatigue-related cognitions in PPS does not explain the lack of efficacy of CBT in this patient group as observed in the FACTS-2-PPS trial. This suggestion is also corroborated by the fact that no differences in the association of the assessed fatigue-related cognitions with fatigue were found between the 2 groups, except for the cognition perceived social support. However, the low absolute scores on this factor in both groups, and the lack of an association with fatigue per group, indicate that perceived social support is not a major problem in these 2 groups. It therefore seems unlikely that this single finding could have explained the observed difference in efficacy of CBT in PPS and FSHD.
Thus, the question remains as to why a cognitive behavioural approach aimed at reducing fatigue in PPS was not effective. It may be that cognitive patterns in people affected with PPS are more difficult to change due to their specific disease history usually with functional limitations from an early age and, added thereto, the long-term duration of fatigue, as found in this study. However, there is currently no evidence in the literature to support this hypothesis and, as no post-treatment data on the cognitive factors were collected in this study, we were not able to test this hypothesis.
Another explanation for the lack of efficacy may be related to the possibility that alleviation of fatigue is not a priority for patients with PPS. Although all patients in this study experienced severe fatigue, a number of patients did not prioritize fatigue as a treatment goal, and, therefore, the CBT intervention was not initiated (n = 5) (14). This assumption is further supported by the findings of a qualitative study that ran parallel to the FACTS-2-PPS trial, in which CBT therapists indicated that most patients did not experience specific distress from the fatigue, nor had need for support in reducing fatigue (37). This finding of low perceived distress from fatigue is in contrast with the results found in a study performed in 1999 on disability and health problems in 76 Dutch patients with PPS, in which 78% of subjects selected fatigue as their main problem (6). It is possible that, in the population of ageing polio survivors, patients are becoming used to the persistent feeling of fatigue, and therefore experience less distress.
This study provides insight into cognitions related to fatigue in PPS compared with FSHD. A limitation of this study is that cognitions were measured with questionnaires that have not been previously validated in PPS or FSHD. Although the questionnaires have been successfully used for targeting CBT interventions in CFS and post-cancer fatigue, and seem to be sufficiently sensitive to distinguish individuals with different levels of dysfunctional cognitions in these populations (15, 38), their clinimetric properties in neuromuscular diseases, such as PPS and FSHD, need to be investigated in future studies.
We tried to maximize the generalizability of our study by recruiting patients from different centres throughout the Netherlands. However, patients had to be able to participate in a relatively demanding study with extensive assessments, for which they sometimes had to travel a long distance. As such, it may be argued that patients with extremely severe fatigue were not willing to participate, thereby restricting the generalizability of our results to the entire population of fatigued patients with PPS or FSHD. However, 33% of the patients with PPS had fatigue severity scores higher than 45. Considering the findings of a previous study that found no ceiling effects on the fatigue severity subscale of the CIS in an unselected sample of polio survivors (28), we believe that our results are fairly representative of (severely) fatigued patients with PPS.
This study showed that fatigue-related cognitions in severely fatigued patients with PPS were similar to those of severely fatigued patients with FSHD and probably also to other populations with a symptom onset later on in their lives who have been proven to benefit from CBT interventions aimed at reducing fatigue (31, 34, 35). Thus, the observed lack of efficacy of CBT in the FACTS-2-PPS trial cannot be attributed to unique cognitive characteristics of patients with PPS. Further studies should investigate the perceived distress from fatigue, acceptance of fatigue symptoms and the felt need for treatment in alleviating fatigue in PPS and, specifically, whether a low need for treatment of fatigue explains, at least in part, the lack of efficacy of a cognitive behavioural approach to reduce fatigue in this population. If this latter can be confirmed, better selection of PPS patients with a high priority for alleviating fatigue may result in more effective application of CBT in this population.
The authors would like to thank the therapists of the CBT interventions, especially Sandra de Moree, for help in carrying out the intervention and their contribution to the interpretation of the data.
This study was funded by Prinses Beatrix SpierFonds (PBF; The Dutch Public Fund for Neuromuscular Disorders)/ZonMw (the Netherlands Organisation for Health Research and Development, ID: ZonMw 89000003)/het Revalidatiefonds/ Revalidatie Nederland/ de Nederlandse Vereniging van Revalidatieartsen (the Netherlands Society of Physical and Rehabilitation Medicine).
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize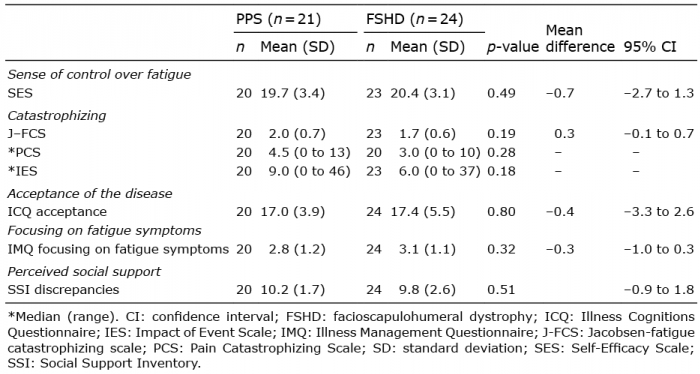 Click to show fullsize
Click to show fullsize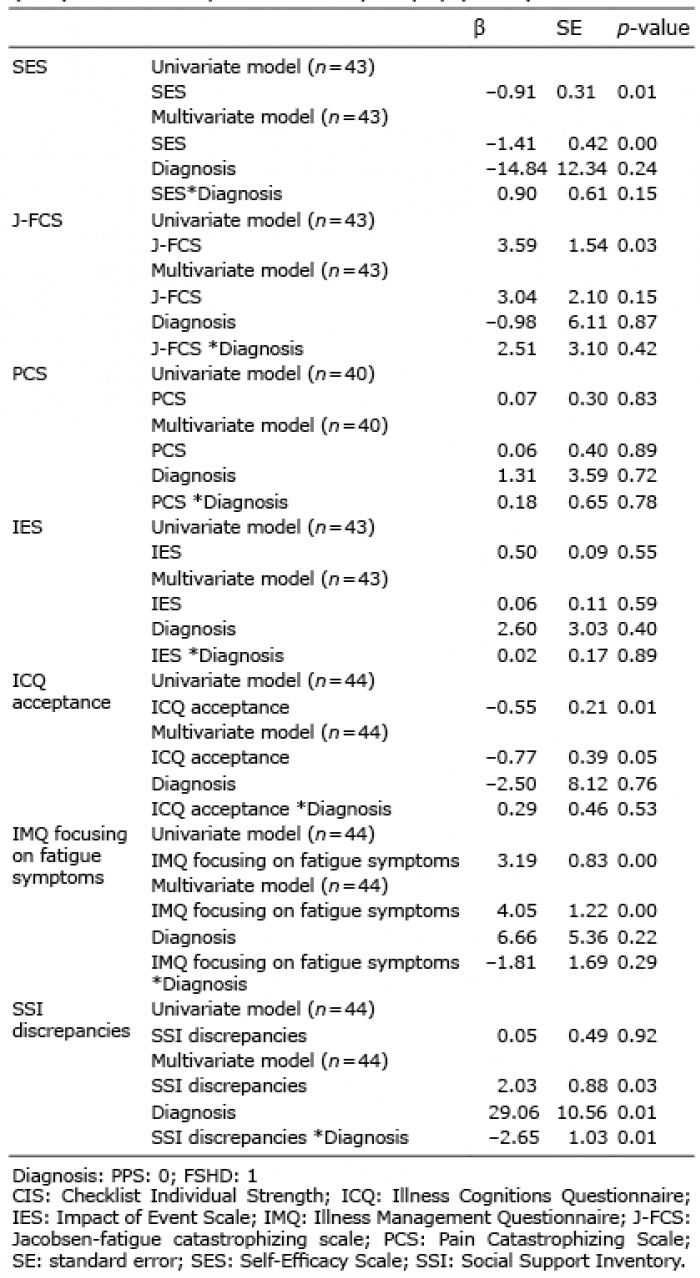 Click to show fullsize
Click to show fullsize