


Akira Hashimoto, Ryuhei Okuyama, Hiroshi Watanabe, Hachiro Tagami and Setsuya Aiba
Department of Dermatology, Tohoku University Graduate School of Medicine, Sendai, Japan
The occurrence of opportunistic infections is not rare during the treatment of connective tissue diseases, including dermatomyositis because of the patient’s immunosuppression. We describe here cytomegalovirus (CMV) infection that affected two of our patients with dermatomyositis. CMV infection has not been considered to be a frequent event in dermatomyositis, and its significance for disease progression has not been sufficiently recognized. Our case reports demonstrate the importance of close monitoring of such patients and prompt initiation of appropriate therapy to manage a suspected CMV infection. Key words: dermatomyositis; cytomegalovirus; opportunistic infection.
(Accepted June 1, 2006.)
Acta Derm Venereol 2006; 86: 535–537.
Ryuhei Okuyama, Department of Dermatology, Tohoku University Graduate School of Medicine, 1-1 Seiryo-machi, Aoba-ku, 980-8574 Sendai, Japan. E-mail: rokuyama@mail.tains.tohoku.ac.jp
Dermatomyositis (DM) is a systemic autoimmune disease characterized by typical cutaneous changes and myositis. It is associated with high morbidity and mortality rates related to life-threatening muscle weakness and lung impairment as well as opportunistic infections, which have been described in 10–20% of such patients (1, 2). In a large series of patients with DM, most opportunistic infections were caused by fungi (2); there are only a limited number of reports regarding infections caused by virus such as cytomegalovirus (CMV) (3, 4). Because CMV infection in patients with DM is not well recognized, this opportunistic infection may have been under-reported in the dermatology literature. In light of the poor prognosis of CMV infection when it involves immunocompromised patients, promptly starting anti-viral therapies is necessary. Thus, we want to present two such cases in patients with DM treated recently.
Case report
Case 1. A 67-year-old Japanese woman visited us for a skin eruption and muscle weakness. Physical examination revealed the presence of purplish erythema involving her face and trunk (Fig. 1a). Abnormal laboratory findings were elevated serum lactic dehydrogenase (LDH) 797 IU/l (normal range 254–474 IU/l) and creatine kinase (CK) 353 IU/l (normal range 45–125 IU/l). KL-6, the marker for interstitial lung diseases, was within a normal range and the patient was HIV-seronegative. Based on the diagnosis of DM she was initially treated with 30 mg/day of prednisolone. However 2 months later, she developed fever together with an increase in serum LDH and especially KL-6 (1239 IU/l; normal range 100–458 IU/l). Chest computed tomography disclosed the presence of bilateral ill-defined multifocal ground-glass opacity (Fig. 1b). Cultures of sputa were negative for pathogenic microorganisms. She was diagnosed as having interstitial pneumonia occurring in association with exacerbation of DM. Cyclophosphamide (50 mg/day) was started together with an increase in the prednisolone dose, after which the abnormal laboratory data gradually improved. However, she suddenly developed severe dyspnoea, and 77 cells among 105 of leukocytes expressed CMV pp65 antigen immunohistochemically, which is absent in normal blood cells. Thus, we immediately halted the cyclophosphamide and initiated gancyclovir therapy (20 mg/kg/day) together with immunoglobulin infusion. In spite of the anti-viral therapy, the cytomegalovirus antigen positive cells did not disappear. She died 2 weeks after the appearance of dyspnoea. At autopsy, lung tissues showed epithelial cells with nuclear inclusions, which was immunohistochemically demonstrated to be positive for CMV antigen (Fig. 1c).
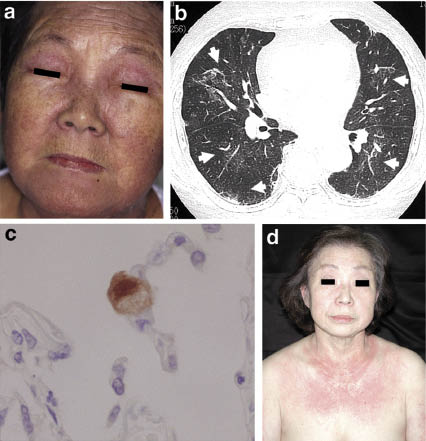
Fig. 1. (a) Clinical features and (b) computed tomographic image in case 1. Note the bilaterally present ill-defined ground-glass opacity in the lungs (arrows). (c) Immunohistochemical finding from the lung showing anti-CMV positive cell. (d) Clinical picture in case 2.
Case 2. A 72-year-old Japanese woman visited us with erythema and myalgia. Physical examination revealed skin abnormalities characteristic of DM consisting of a heliotrope rash, Gottron’s papules, and violaceous erythematous lesions (Fig. 1d). Abnormal laboratory findings were elevated serum levels of CK 359 IU/l, LDH 949 IU/l, and aspartate aminotransferase (ASAT) 46 IU/l (normal range 12–30 IU/l), but alanine aminotransferase (ALAT) was 29 IU/l (normal range 8–35 IU/l). She was seronegative for HIV. Under a diagnosis of DM she was treated with oral prednisolone (60 mg/day). Since her clinical symptoms and abnormal laboratory data had all normalized, we gradually decreased the dose of prednisolone. However, after 3 months of oral prednisolone administration, she suddenly developed fever together with an elevation of serum liver enzymes; her serum ASAT and ALAT reached 178 IU/l and 241 IU/l, respectively. A chest roentgenogram revealed no abnormality. However, CMV pp65 antigen immunostains revealed the presence of 51 positive cells per 105 of leukocytes. Intravenous gancyclovir was initiated as an attempt to reach a diagnosis and for therapy. One week after the start of this treatment, the cytomegalovirus positive cells had totally disappeared.
Discussion
We describe here 2 cases of CMV infection affecting patients with DM, both of whom had no internal malignancy. One of them was an immunohistochemically proven case of CMV infection, while the other showed only CMV antigenaemia with a dramatic improvement in the clinical conditions after treatment with gancyclovir. DM is sometimes associated with opportunistic infection, and fungi have been reported to be responsible for about 50% of the cases (1, 2). In contrast, there are only a limited number of reports regarding CMV infection in DM (3, 4). Serious CMV infection occurs frequently in immunocompromised patients, such as transplant recipients and patients with AIDS, but is rare in people without underlying diseases (5). Our present cases suggest that CMV infection may occur more frequently in DM patients than previously recognised.
Opportunistic infections with CMV usually demonstrate retinitis, colitis and pneumonitis, without symptoms specific to CMV. Thus, it is sometimes difficult to determine whether these clinical manifestations are due to DM or due to a concomitant infection. A definite diagnosis of CMV infection is based only on the histological identification of CMV proliferation, but organ biopsy is rarely conducted. Recently, the introduction of molecular-based diagnostic tests, such as polymerase chain reaction (PCR) and immunohistochemical staining specific to CMV pp65 antigen, have made it possible to intervene early in the course of CMV infection (6). PCR is a sensitive and specific assay to detect CMV DNA. Especially, real-time PCR has provided rapid result and the capability for producing quantitative levels of CMV DNA that are useful for predicting disease and monitoring response to anti-viral therapy (7). The antigenaemia assay against pp65 antigen, the CMV-specific protein, detects CMV in polymorphonuclear leukocytes, which is disseminated from viral-invaded organs (7). Although the clinically relevant threshold for the number of infected polymorphonuclear leukocytes differs among patient populations, generally the presence of more than 10 positive cells per 2 × 105 cells has been suggested as an indication for CMV therapy.
Several drugs such as gancyclovir, valgancyclovir, and foscarnet are now available for treating CMV (8). However, they should be used with caution because of side-effects that include myelosuppression and renal impairment. Although prophylactic antiviral medication can reduce the risk of CMV infection in recipients of solid-organ transplants, its efficacy has not been established for other immunocompromised hosts. It is imperative to evaluate carefully the benefit of the prophylactic therapy and its adverse effects in patients with DM who present with suspected symptoms, especially during the therapy with immunosuppressants.
References
1. Viguier M, Fouere S, de la Salmoniere P, Rabian C, Lebbe C, Dubertret L, et al. Peripheral blood lymphocyte subset counts in patients with dermatomyositis: clinical correlations and changes following therapy. Medicine (Baltimore) 2003; 82: 82–86.
2. Marie I, Hachulla E, Cherin P, Hellot MF, Herson S, Levesque H, Hatron PY. Opportunistic infections in polymyositis and dermatomyositis. Arthritis Rheum 2005; 53: 155–165.
3. Sepkowitz KA. Opportunistic infections in patients with and patients without Acquired Immunodeficiency Syndrome. Clin Infect Dis 2002; 34: 1098–1107.
4. Kasifoglu T, Korkmaz C, Ozkan R. Cytomegalovirus-induced interstitial pneumonitis in a patient with dermatomyositis. Clin Rheumatol 2006; 25: 731–733.
5. Nichols WG, Boeckh M. Recent advances in the therapy and prevention of CMV infections. J Clin Virol 2000; 16: 25–40.
6. Humar A, O’Rourke K, Lipton J, Messner H, Meharchand J, Mahony J, et al. The clinical utility of CMV surveillance cultures and antigenemia following bone marrow transplantation. Bone Marrow Transplant 1999; 23: 45–51.
7. Razonable RR, Paya CV, Smith TF. Role of the laboratory in diagnosis and management of cytomegalovirus infection in hematopoietic stem cell and solid-organ transplant recipients. J Clin Microbiol 2002; 40: 746–752.
8. Hodson EM, Jones CA, Webster AC, Strippoli GF, Barclay PG, Kable K, et al. Antiviral medications to prevent cytomegalovirus disease and early death in recipients of solid-organ transplants: a systematic review of randomised controlled trials. Lancet 2005; 365: 2105–2115.

