


Stefano Tabolli1, Livia Alessandroni1, Jeanette Gaido2, Francesca Sampogna1, Cristina Di Pietro1 and Damiano Abeni1
1Health Services Research Unit, and 2Mycology Service, Istituto Dermopatico dell’Immacolata (IDI-IRCCS), Rome, Italy
Health-related quality of life (HRQoL) measurements in clinical practice ensure that treatment and evaluations focus on the patient rather than the disease. To verify whether these measurements are also relevant in a minor dermatological disease and whether a generic routine assessment is sufficient to capture different aspects of quality of life, we studied patients affected by nail disorders. The Skindex-29, the 12-item General Health Questionnaire and the 36-item Short Form of the Medical Outcomes Study questionnaires were used. A total of 114 patients were enrolled: 31% men aged 48 ± 15 years and 69% women aged 49 ± 14 years (mean ± SD). The mean values of SF-36 scales in nail disorders were higher than those reported for minor skin diseases, and Skindex-29 values were lower. A duration of disease ≥1 year was associated with higher Skindex-29 scores on the symptom and emotions scales. Patients with onychomycosis have higher values on the Skindex-29 social functioning scale compared with other nail disorders. The use of HRQoL measurements in routine clinical activities allows us to depict how nail disorders affect patients and show how relevant some neglected aspects, such as pain or emotional trauma, are and offers us the opportunity to address these issues in a patient-centred approach to treatment. Key words: nail disorder onychomycosis; life quality; dermatology; outcome research.
(Accepted November 14, 2006.)
Acta Derm Venereol 2007; 87: 255–259.
Stefano Tabolli, Istituto Dermopatico dell’Immacolata IDI IRCCS, Via dei Monti di Creta, 104, IT-00167 Rome, Italy. E-mail: ste.tab@idi.it
Patient-reported outcome measures in clinical practice, in particular those evaluating health-related quality of life (HRQoL), have been proposed as a means of facilitating doctor–patient communication by quantifying the patient’s problems, as well as a tool for monitoring disease activity during treatment and for screening for functional problems (1–3).
Many self-administered questionnaires are available for use in clinical settings, and are designed to measure either generic or disease-specific HRQoL. However, while HRQoL measures are now quite commonly included in the protocols of randomized controlled clinical trials and other clinical research studies, their use in routine clinical practice is still quite limited.
We have recently introduced evaluation of HRQoL into routine clinical practice in our Dermatology Unit, which is devoted mainly to severe conditions in hospitalized patients, in our Institute in Rome. HRQoL measures in clinical practice may be used as a way of investigating the personal and social context of patients and of linking it to the classical clinical view of disease (4, 5). In addition, these measures can be used to increase awareness among clinical personnel of the complexity of the negative effects of diseases, thus allowing problems to be prioritized and specific targets for intervention identified.
Our objective was to verify whether these measurements were also relevant in outpatients with conditions classified as “minor” dermatological diseases, such as nail disorders, and to evaluate if the generic routine HRQoL assessment performed was sufficient to capture different aspects of quality of life (QoL). Nail disorder is a generic clinical term for all those pathologies affecting nails, including nail dystrophy or onychomycosis.
Nail dystrophy can be caused by local factors, such as trauma or malformations, or by systemic factors such as arthrosis, and may be a manifestation of a skin disease, such as psoriasis, lichen planus, alopecia areata, eczema, or Darier disease. Moreover, different drugs can cause nail disorders: antibiotics, psoralene, cytotoxic agents and anti-malarials. Onychomycosis is a common fungal infection of the fingernails and toenails with, for example, dermatophytes, moulds or yeasts.
Apart from the aetiology, nail diseases have certain clinical characteristics in common, such as thickening, splitting, roughening, pitting and dyschromic changes. Although these are non life-threatening conditions, important nail functions may be severely altered in the presence of onychomycosis, with serious adverse effects on the QoL of patients. Dystrophic fungal nails can cause pain and inflammation, and can lead to loss of the nail. This condition can interfere with normal daily activities, such as walking and standing. It can cause shoes to fit poorly and may affect the productivity of those people whose work requires that they stand all day.
In this study, we analysed data on QoL and minor non-psychotic psychiatric disorders in a group of patients affected by nail disorders, seen at an outpatient clinic in our institute.
METHODS
Patients and investigation settings
The study was carried out in March and April 2005 at the Dermatological Institute IDI-IRCCS, Rome, Italy. All patients aged 18–75 years referred to the outpatient clinic for nail disorders were invited to participate in the study. Patients who were unable to complete the questionnaires due to illiteracy or who had severe mental or physical illnesses were excluded. We included in the study only patients who had not received specific antifungal treatment for at least the previous 3 months.
Full information about the study methods and purposes was provided, and patients who agreed to participate and signed a written informed consent form received three research questionnaires. Patients were invited to complete them immediately before the visit during which microscopic examination and specimen culture was performed. On average, completing the questionnaires took approximately 15–20 minutes. The questionnaires were then collected by a research dermatologist, who checked them for completeness and passed them to the unit devoted to data entry and processing. The questionnaires were not seen by the dermatologist who recorded the relevant clinical information and established the diagnosis for each patient. The study was approved by the ethics committee of IDI-IRCCS.
Instruments
The Skindex-29, the 12-item General Health Questionnaire (GHQ-12), and the 36-item Short Form of the Medical Outcomes Study questionnaire (SF-36) were used.
The Skindex-29 is a reliable and valid instrument that has been designed specifically for measuring HRQoL in dermatological patients (6): its Italian version has been validated recently (7, 8). The Skindex-29 comprises 3 scales assessing burden of symptoms, social functioning and emotional state. Patients answered the 29 questions referring to the previous 4-week period, on a 5-point scale from “never” (= 0) to “all the time” (= 4). The score of each scale ranges from 0 to 100 (as a percentage of the maximum score obtainable on that scale), and higher scores reflect a worse QoL.
The GHQ-12 is a self-administered questionnaire designed to measure psychological distress and to detect current non-psychotic psychiatric disorders (9), usually depressive or anxiety disorders. The reliability and validity of the Italian version has been documented in many types of patients, including those with dermatological conditions (10). Answers are given on a 4-point scale. When scored with the binary method (0-0-1-1), the GHQ-12 can be used as a screening tool to detect minor non-psychotic psychiatric disorders. In this way, each subject obtains a score from 0 to 12 (11): operationally, patients scoring 4 or more were considered as “GHQ-cases” (GHQ+).
The SF-36 is a generic indicator of health status, designed to be applicable to a wide range of types and severity of conditions (12). It is a useful instrument for monitoring patients with multiple conditions, for comparing the health status of patients with different conditions, and for comparing patients with the general population. The SF-36 includes 36 items, in a Likert-type or forced-choice format, intended to measure the following 8 dimensions: physical functioning (limitations in performing physical activities such as bathing or dressing), role-physical (limitations with work and other daily activities as a result of physical health), bodily pain (how severe and limiting is pain), general health (how general personal health is evaluated by the patient), vitality (feeling tired vs. feeling full of energy), social functioning (interference with normal social activities due to physical or emotional problems), role-emotional (limitations with work and other daily activities as a result of emotional problems), mental health (feeling nervous and depressed vs. peaceful, happy and calm). Scores for each domain range from 0 to 100, with high scores indicating a better status. We used the Italian version of the SF-36 (13), cross-culturally validated within the framework of the International Quality of Life Assessment (IQOLA) Project.
Statistical analysis
The mean score was calculated for all the instruments in all the levels of the variables of interest, such as sex, age, presence or absence of onychomycosis, duration and extension of the disease. Differences between subgroups were tested using the Student’s t-test.
Skindex 29 and SF-36 values in nail disorders were compared with values observed in minor skin diseases (i.e. dermatitis, warts, erythema, etc. These patients were involved in another study about HRQoL assessment in the routine practice during the same period).
The computer package Stata 9.0 for Windows (Stata Corp., College Station, TX, USA) was used for all statistical analyses.
RESULTS
During the 2-month study period, 114 patients were enrolled: 31% men and 69% women, with a mean age ± SD of 48 ± 15 and 49 ± 14 years, respectively. Three patients declined to participate.
Table I shows the mean values of the Skindex-29, SF-36 and GHQ-12 score (expressed as percentage of patients with a score ≥4) in nail disorders in relation to relevant variables, such as sex, age, presence or absence of onychomycosis, duration and extension of the disease. Skindex-29 values are low compared with other dermatological diseases and with the mean of values reported for all dermatological outpatients (14), however in particular the emotional scores were often also in the “fair” range of HRQoL. In Skindex-29, even if it is not specific for nail disorders, 17% of patients answered “all the time” to the item “I worry that my skin condition may get worse”, 15% at “I am annoyed by my skin condition” and 12% for “I am ashamed of my skin condition” (emotions scale). Almost 10% said “My skin hurts”(symptoms scale) and 11% reported “I tend to do things by myself because of my skin condition” (social functioning scale) “all the time”. No differences were observed between males and females for HRQoL measurement in the 3 Skindex-29 domains, while all SF-36 mean values were higher for males, as generally observed (13). The percentage of GHQ+ cases, as defined in the Methods section, was slightly higher in men (36.4%) than in women (33.8%), while in other studies we had constantly observed a significantly higher prevalence among females (14, 15).
Table I. Mean values for Skindex-29 and SF-36, and percentages of GHQ+ (minor psychiatric disorder) cases in patients with nail disorders (n=114)
| n | % | Skindex-29 | SF-36 | GHQ-12 (≥4) | |||||||||||
| Symptomsa | Emotionsb | Social-functioningc | PF | RP | BP | GH | VT | SF | RE | MH | % | ||||
| Sex | Male | 35 | 30.7 | 16.5 | 19.5 | 12.2 | 91.7 | 89.3 | 86.4 | 68.4 | 68.1 | 84.3 | 81.9 | 68.1 | 36.4 |
| Female | 79 | 69.3 | 16.4 | 21.1 | 11.1 | 88.2 | 74.4 | 70.2 | 65.6 | 60.6 | 74.1 | 61.8 | 65.3 | 33.8 | |
| Age (years) | |||||||||||||||
| <40 | 32 | 28.0 | 16.7 | 21.5 | 9.1 | 96.1 | 89.1 | 81.8 | 72.5 | 63.8 | 77.7 | 79.2 | 66.9 | 36.7 | |
| 40–55 | 37 | 32.5 | 17.4 | 22.2 | 15.4 | 92.1 | 77.0 | 76.2 | 65.1 | 59.7 | 74.0 | 56.8 | 64.5 | 37.8 | |
| >55 | 45 | 39.5 | 15.5 | 18.5 | 9.9 | 82.1 | 73.3 | 69.6 | 62.6 | 65.1 | 79.4 | 69.9 | 67.1 | 30.2 | |
| Diseases | |||||||||||||||
| Onychomycosis | 66 | 57.9 | 18.8 | 22.1 | 14.7 | 88.9 | 78.0 | 75.0 | 66.2 | 64.0 | 77.7 | 66.7 | 67.9 | 34.9 | |
| Other nail disorders | 48 | 42.1 | 13.3 | 18.5 | 6.9* | 89.8 | 80.2 | 75.4 | 66.9 | 61.6 | 76.6 | 70.3 | 64.1 | 34.0 | |
| Onychomycosis | |||||||||||||||
| Dermatophytes sp. | 23 | 34.8 | 21.6 | 21.8 | 14.1 | 87.8 | 80.4 | 76.3 | 71.5 | 63.1 | 79.9 | 69.6 | 69.5 | 30.4 | |
| Non-dermatophytes moulds sp. | 22 | 33.3 | 15.7 | 22.2 | 14.4 | 93.1 | 85.2 | 80.3 | 61.1 | 61.5 | 74.4 | 66.7 | 65.0 | 50.0 | |
| Candida sp. | 17 | 25.8 | 21.5 | 22.0 | 15.2 | 84.7 | 66.2 | 70.5 | 65.8 | 72.6 | 79.4 | 62.2 | 72.0 | 29.4 | |
| Mixed | 4 | 6.1 | 8.0 | 24.4 | 18.2 | 88.8 | 75.0 | 57.8 | 66.5 | 53.8 | 75.0 | 66.7 | 61.0 | 0.0 | |
| Duration | |||||||||||||||
| <1 year | 42 | 36.8 | 12.0 | 16.3 | 8.4 | 90.9 | 84.5 | 71.8 | 68.9 | 61.5 | 77.1 | 70.8 | 68.5 | 30.8 | |
| ≥1 year | 72 | 63.2 | 19.1* | 23.1* | 13.2 | 88.3 | 75.7 | 77.2 | 65.3 | 63.8 | 77.3 | 66.7 | 64.8 | 36.6 | |
| Area involved | |||||||||||||||
| Fingernails | 25 | 21.9 | 18.8 | 18.9 | 12.7 | 87.1 | 76.0 | 70.3 | 69.8 | 72.2 | 77.0 | 73.9 | 74.0 | 25.0 | |
| Toenails | 85 | 74.6 | 15.8 | 20.3 | 10.2 | 90.1 | 79.1 | 76.6 | 66.1 | 61.1 | 77.4 | 65.9 | 64.3 | 39.0 | |
| Both | 4 | 3.5 | 15.9 | 37.5 | 29.6 | 83.8 | 93.8 | 75.0 | 62.3 | 53.8 | 75.0 | 83.3 | 68.0 | 0.0 | |
*p < 0.05.
aReference values: 0.1– <14 (very good), 14–<29 (good), 29–<50 (fair).
bReference values: 0.1–<11 (very good), 11–<26 (good), 26–<51 (fair).
cReference values: 0.1–<9 (very good), 9–<23 (good), 23–<44 (fair).
PF: physical functioning, RP: role-physical; BP: bodily pain; GH: general health; GHQ: general health questionnaire; VT: energy/fatigue; SF: social functioning; RE: role-emotional; MH: mental health.
No significant differences were observed in the Skindex-29 scales for different age groups, with a moderate increase of values for the group 40–55 years. As expected, a reduction in SF-36 values in each scale, especially for physical domains, was observed with increasing age.
HRQoL as measured by Skindex-29 was more impaired when the disease lasted more than one year (p <0.05 for symptoms and emotions; not significant for social functioning), however this difference was not observed in the SF-36 scales. Also, the percentage of GHQ+ cases was higher in the group with longer duration of the disease but the differences were not statistically significant. After direct microscopy and culture medium of nail material, 58% of nail disorders were recognized as onychomycosis and these had higher values in all Skindex-29 scales, and especially in the functioning scale, where the difference was statistically significant (p <0.05). Among onychomycoses, Candida sp. were the infections that compromised the SF-36 physical domains the most.
Almost 75% of patients had toenail involvement and only 3.5% of this group of patients had an involvement of both fingernails and toenails.
GHQ+ cases had somewhat higher Skindex-29 and lower SF-36 mean values in each scale (data not shown).
Fig. 1 represents the mean values of SF-36 dimensions and Skindex-29 scales for all examined patients with nail disorders, compared with minor skin diseases (25 patients with dermatitis, warts, erythema, etc., involved in a study about HRQoL assessment in the routine practice, examined in the same period). HRQoL as measured by the SF-36 was slightly higher in patients with nail disorders than in the group with minor skin diseases, and significantly better in all the Skindex-29 scales.
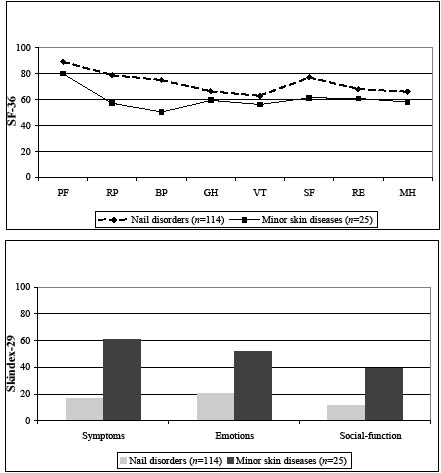
Fig. 1. Mean values of SF-36 and Skindex-29 scores for patient with nails disorders vs. minor skin diseases. Norms for the general Italian population: PF 88.7 ± 14.9, RP 81.7 ± 30.3, BP 75.2 ± 27.0, GH 66.5 ± 17.5, VT 63.4 ± 18.2, SF 78.4 ± 20.1, RE 79.2 ± 33.6, MH 67.8 ± 18.2.
PF: physical functioning; RP: role-physical; BP: bodily pain; GH: general health; VT: vitality; SF: social functioning; RE: role-emotional; MH: mental health.
DISCUSSION
In many patients nail problems can interfere significantly with important aspects of daily living. Individuals may have reduced self-confidence and avoid social and leisure activities. However, many physicians perceive onychomycosis, which accounts for half of all nail disorders and about one-third of cutaneous fungal infection (16, 17), as a cosmetic rather than a medical problem, so that its impact on the QoL of patients is often underestimated.
Until now, only a few studies have tried to assess the possible effect of onychomycosis on different aspects of patients’ QoL and only a few specific questionnaires have been developed (18–23). All of these studies demonstrated that, although onychomycosis is not a life-threatening condition, it is associated with a significant degree of physical and psychological morbidity for a large proportion of patients, and they emphasized the importance of HRQoL assessment in the clinician’s decision to initiate the treatment.
Here we also reported that with generic HRQoL instruments, used in routine clinical activities in a dermatological setting, it was possible to identify how nail disorders affected the patients’ QoL and that the group of patients with onychomycosis had lower QoL.
In the present study, data indicate that symptoms of onychomycosis and their impact on personal appearance are an important determinant of patients’ perceptions of their own health. As for fingernail disorders, QoL in Italian patients seemed to be less impaired compared with other countries. This may depend on different levels of severity, but it may also reflect cultural differences in the importance attributed to this condition. However, it was reported (19) that QoL scores in nail disorders were significantly different between countries, especially for the social and emotional scale.
As for mental disorders, it is known that they are frequent among dermatological patients. Epidemiological studies reported prevalence estimates ranging between 21% and 43% (15, 24, 25) and showed that the most frequent mental disorders in patients with skin diseases are depressive and anxiety disorders. In our study, the percentages of 36% and 34% of positive GHQ-12 cases in men and women with nail disorders were in the range expected of GHQ-12-positive cases for skin diseases. However, we observed more positive cases of GHQ-12 in men than in women. One interpretation of this result could be that men in general do not camouflage their affected nails, so their social life might be affected more and consequently they may have psychological problems. Another interpretation of such data could be that men who were referred to our outpatient department for nail disorder had minor psychiatric problems per se, or for some reason the group of men was a selected one. It should be taken into account that the patients in this study were referred by the general practitioner, probably after unsuccessful therapy, or because patients were dissatisfied with the previous outcome, thus generalizations should be made with caution.
In conclusion, nail disorders and onychomycosis may have a substantial negative effect on patients’ QoL. Physicians should be aware that these conditions are not just a cosmetic nuisance, but are painful and potentially disabling disorders that can have a serious impact on a patient’s life, and that they therefore deserve more medical attention.
Using specific questionnaires and general instruments usually applied in routine HRQoL assessment, it is possible to obtain important information on the impact that nail disorders have on the emotional and social life of patients with respect to disease involvement, duration of the disease and therapy.
ACKNOWLEDGEMENTS
This study was partially supported by progetto Ricerca Corrente of the Italian Ministry of Health.
REFERENCES
1. Higginson IJ, Carr AJ. Measuring quality of life: using quality of life measures in the clinical setting. BMJ 2001; 322: 1297–1300.
2. Lohr KN. Advances in health status assessment. Overview of the conference. Med Care 1989; 27: S1–11.
3. Lohr KN. Applications of health status assessment measures in clinical practice. Overview of the third conference on advances in health status assessment. Med Care 1992; 30: MS1–14.
4. Bowling A, editor. Measuring disease. Buckingam: Open University Press, 1995.
5. Rosser RM. A history of development of health indices. In Smith GT, editor. Measuring the social benefits of medicine. London: Office of Health Economics, 1985.
6. Chren MM, Lasek RJ, Flocke SA, Zyzanski SJ. Improved discriminative and evaluative capability of a refined version of Skindex, a quality-of-life instrument for patients with skin diseases. Arch Dermatol 1997; 133: 1433–1440.
7. Abeni D, Picardi A, Puddu P, Pasquini P, Chren MM. Construction and validation of the Italian version of Skindex-29, a new instrument to measure quality of life in dermatology [in Italian, abstract in English]. G Ital Dermatol Venereol 2001; 136: 73–76.
8. Abeni D, Picardi A, Pasquini P, Melchi CF, Chren MM. Further evidence of the validity and reliability of the Skindex-29: an Italian study on 2242 dermatological outpatients. Dermatology 2002; 204: 43–49.
9. Piccinelli M, Bisoffi G, Bon MG, Cunico L, Tansella M. Validity and test-retest reliability of the Italian version of the 12-item General Health Questionnaire in general practice: a comparison between three scoring methods. Compr Psychiatry 1993; 34: 198–205.
10. Picardi A, Abeni D, Pasquini P. Assessing psychological distress in patients with skin diseases: reliability, validity and factor structure of the GHQ-12. J Eur Acad Dermatol Venereol 2001; 15: 410–417.
11. Picardi A, Abeni D, Mazzotti E, Fassone G, Lega I, Ramieri L, et al. Screening for psychiatric disorders in patients with skin diseases: a performance study of the 12-item General Health Questionnaire (GHQ-12). J Psychosom Res 2004; 57: 219–223.
12. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992; 30: 473–483.
13. Apolone G, Mosconi P. The Italian SF-36 Health Survey: translation, validation and norming. J Clin Epidemiol 1998; 51: 1025–1036.
14. Sampogna F, Picardi A, Chren MM, Melchi CF, Pasquini P, Abeni D. Association between poorer quality of life and psychiatric morbidity in patients with different dermatological conditions. Psychosom Med 2004; 66: 620–624.
15. Picardi A, Abeni D, Melchi CF, Puddu P, Pasquini P. Psychiatric morbidity in dermatological outpatients: an issue to be recognized. Br J Dermatol 2000; 143: 983–991.
16. Shear RK, Drake LA. Onychomycosis: a significant disease. In: Proceedings of the 2nd International Symposium on Onychomycosis, Florence, Italy, Sept 28–29 1995. Macclesfield: Gariner-Calwell Communication Ltd, 1996.
17. Shear NH, Gupta AK. Terbinafine for the treatment of pedal onychomycosis: a foot closer to the promised land of cured nails? Arch Dermatol 1995; 131: 937–942.
18. Lubeck DP, Gause D, Schein JR, Prebil LE, Potter LP. A health-related quality of life measure for use in patients with onychomycosis: a validation study. Qual life Res 1999; 8: 121–129.
19. Drake LA, Patrick DL, Fleckman P, André J, Baran R, Haneke E, et al. The impact of onychomycosis on quality of life: development of an international onychomycosis-specific questionnaire to measure patient quality of life. J Am Acad Dermatol 1999; 41: 189–196.
20. Turner RR, Testa MA. Measuring the impact of onychomycosis on patient quality of life. Qual Life Res 2000; 9: 39–53
21. Whittam LR, Hay RJ. The impact of onychomycosis on quality of life. Clin Exp Dermatol 1997; 22: 87–89.
22. Elewski BE. The effect of toenail onychomycosis on patient quality of life. Int J Dermatol 1997; 36: 754–756.
23. Shaw JW, Joish VN, Coons SJ. Onychomycosis: health -related quality of life considerations. Pharmacoeconomics 2002; 20: 23–36.
24. Hughes JE, Barraclough BM, Hamblin LG, White JE. Psychiatric symptoms in dermatology patients. Br J Psychiatry 1983; 143: 51–54.
25. Picardi A, Abeni D, Renzi C, Braga M, Puddu P, Pasquini P. Increased psychiatric morbidity in female outpatients with skin lesions on visible parts of the body. Acta Derm Venereol 2001; 81: 410–414.

