Hideo Tokunaga, Ryuhei Okuyama*, Hachiro Tagami and Setsuya Aiba
Department of Dermatology, Tohoku University Graduate School of Medicine, 1-1 Seiryo-machi, Aoba-ku, 980-8574 Sendai, Japan. *E-mail: rokuyama@mail.tains.tohoku.ac.jp
Accepted March 8, 2007.
Sir,
Lupus miliaris disseminatus faciei (LMDF) or acne agminata is a chronic inflammatory disorder that occurs singly or in crops on the eyelids, cheeks and nasolabial folds (1). Clinically it consists of multiple indolent bright-red or brown papules. Histologically, it is characterized by dermal masses of tuberculoid granulomas with central caseation necrosis. LMDF is currently widely considered as a variant of rosacea (2). However, in contrast to rosacea, which shows a chronic course, LMDF runs a self-limiting course with spontaneous resolution of the lesions during 12–24 months, often leaving disfiguring scars. The occurrence of LMDF appears to be related to an immune response to the pilosebaceous units (3), suggesting that immunosuppressants would be good candidates for therapy. We describe here a patient with LMDF who was treated successfully with intramuscularly administered triamcinolone acetonide.
Case report
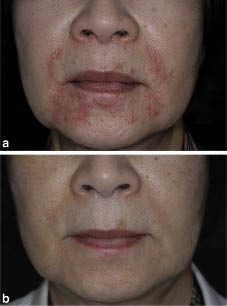
A 68-year-old Japanese woman presented with a 2-year history of a non-pruritic papular facial eruption. She did not have a history of topical steroid exposure to her face. On examination, the eruption consisted of multiple erythematous and gelatinous papules 1–3 mm in diameter, which were predominantly distributed on the nasolabial fold and perioral region with some extending to the eyelids and neck (Fig. 1a). Facial erythema or telangiectasia suggestive of rosacea was absent. Full blood count, electrolytes, liver function tests, serum calcium, angiotensin-converting enzyme and chest X-ray were all within normal limits.
Fig. 1. Lupus miliaris disseminatus faciei, (a) before and (b) after 3 injections of triamcinolone acetonide.
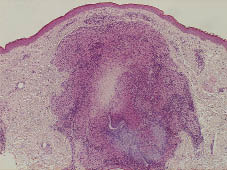
A skin biopsy specimen taken from one of the facial papules showed the presence of granulomatous changes in the upper- and mid-dermis consisting of epithelioid macrophages and giant cells with central caseation necrosis (Fig. 2). Granulomatous changes were also seen around the hair follicles, partially destroying them. Staining for fungi or acid-fast organisms was negative. Based on the diagnosis of LMDF, the patient was initially treated with oral doxycycline, 100 mg/day. However, one month later, her condition failed to improve and the lesions became more extensive. Intramuscular injection of triamcinolone acetonide was started at a dose of 40 mg once every month. Within one month improvement was seen clinically. After 3 injections of triamcinolone acetonide, all the papules disappeared without leaving any scars (Fig. 1b). There were no specific side-effects. No recurrence of the skin lesions occurred over the following period of 12 months.
Fig. 2. Granuloma consisting of epithelioid macrophages and giant cells with central caseation necrosis (H&E ×100).
Discussion
Granuloma with caseation necrosis is the hallmark of LMDF. However, the facial changes of the woman described resembled perioral dermatitis. This condition is usually improved by antibiotics including doxycycline and is deteriorated by steroid after temporary remission (4). LMDF was originally considered to be a variant of lupus vulgaris or tuberculid from its histopathological resemblance to tuberculosis. However, the evidence supporting its tuberculous aetiology is largely circumstantial and not always convincing (5). Currently, LMDF is widely regarded as a papular form of rosacea, which is supported by the observation that the granulomas found in LMDF appear in close approximation to the pilosebaceous units, and by the fact that epithelioid granulomas have been found in some patients with rosacea (6). On the other hand, the clinical features of LMDF are distinct from those of rosacea in several points. In particular, its predilection sites are those not involved by rosacea, such as the eyelids and upper lip, in addition to its self-limiting course leaving scars.
Although the precise pathomechanism of LMDF is still unknown, an immune response to the pilosebaceous units seems highly likely to be involved in the granuloma formation in LMDF (2, 3). The histological picture of LMDF could be regarded as a granulomatous reaction to the breakdown products of the pilosebaceous apparatus. In fact, epithelioid cell granuloma was experimentally produced by intradermal injection of sebum and comedones (7). Furthermore, LMDF was reported to be associated with numerous small epidermal cysts, which suggests the possibility that rupture of the epidermal cysts may also induce inflammation leading to the granuloma formation in LMDF (8). In addition, we can not neglect the possibility that Demodex folliculorum influenced the immune response to the pilosebaceous units.
For treatment of this condition, antibiotics (9, 10), dapsone (11) and oral steroids (12) have been reported to show variable success. Based on the close correlation of the inflammation in LMDF with the pilosebaceous apparatuses, immunosuppressants would be expected to have a therapeutic effect. However, topical steroids are often ineffective. Oral steroid administration has shown some benefit, depending on the timing of its start; it is less effective when started late in the course of the disease. As shown in the present case, intramuscular triamcinolone acetonide could offer a significant advantage over orally administered steroids. We do not have a plausible explanation for this therapeutic effect, but since an injection of 40 mg of triamcinolone acetonide produces a suppressive effect on the adrenal gland for 4 weeks, we think that the effect on the skin lesions resulted from the long-acting, high levels of circulating corticosteroid (13). It has been shown that intramuscular triamcinolone is beneficial in the management of a variety of inflammatory dermatoses (14). Additionally, in cases of severe asthma, intramuscular triamcinolone was shown to be significantly more effective than oral prednisolone for controlling the condition (15). Furthermore, the side-effects from intramuscularly administered triamcinolone would probably be no more troublesome than those from oral prednisolone (15, 16). Four mg of triamcinolone corresponds to 5 mg of prednisolone. The total dose of monthly administered triamcinolone, usually 40 mg, is much lower than that of prednisolone (17). In addition, despite the fact that the common adverse effects of corticosteroids, such as menstrual irregularities, muscle weakness, and facial hirsutism are more pronounced with triamcinolone, such side-effects would rarely warrant the cessation of its short-term use in cases of LMDF.
References
1. Mullanax MG, Kierland RR. Granulomatous rosacea. Arch Dermatol 1970; 101: 206–211.
2. el Darouti M, Zaher H. Lupus miliaris disseminatus faciei – pathologic study of early, fully developed, and late lesions. Int J Dermatol 1993; 32: 508–511.
3. Shitara A. Lupus miliaris disseminatus faciei. Int J Dermatol 1984; 23: 542–544.
4. Dolenc-Voljc M, Pohar M, Lunder T. Density of Demodex folliculorum in perioral dermatitis. Acta Derm Venereol 2005; 85: 211–215.
5. Hodak E, Trattner A, Feuerman H, Feinmesser M, Tsvieli R, Mitrani-Rosenbaum S, et al. Lupus miliaris disseminatus faciei – the DNA of Mycobacterium tuberculosis is not detectable in active lesions by polymerase chain reaction. Br J Dermatol 1997; 137: 614–619.
6. Helm KF, Menz J, Gibson LE, Dicken CH. A clinical and histopathologic study of granulomatous rosacea. J Am Acad Dermatol 1991; 25: 1038–1043.
7. Strauss JS, Pochi PE. Intracutaneous injection of sebum and comedones. Histological observations. Arch Dermatol 1965; 92: 443–456.
8. Watabe A, Okuyama R, Tagami H, Aiba S. Lupus miliaris disseminatus faciei associated with epidermal cysts. Dermatology 2007; 214: 272–273.
9. Dekio S, Jidoi J, Imaoka C. Lupus miliaris disseminatus faciei – report of a case in an elderly woman. Clin Exp Dermatol 1991; 16: 295–296.
10. Goh BK, Tan HH. Doxycycline in the treatment of acne agminata. Clin Exp Dermatol 2003; 28: 677–679.
11. Kumano K, Tani M, Murata Y. Dapsone in the treatment of miliary lupus of the face. Br J Dermatol 1983; 109: 57–62.
12. Uesugi Y, Aiba S, Usuba M, Tagami H. Oral prednisone in the treatment of acne agminata. Br J Dermatol 1996; 134: 1098–1100.
13. Mikhail GR, Livingood CS, Mellinger RC, Paige TN, Salyer HL. Effect of long-acting parenteral corticosteroids on adrenal function. Arch Dermatol 1969; 100: 263–268.
14. Rosten M. The treatment of skin disorders with intramuscular triamcinolone acetonide. NZ Med J 1970; 72: 253–255.
15. Veeraraghavan S, Sharma OP. Parenteral triamcinolone acetonide: an alternative corticosteroid for the treatment of asthma. Curr Opin Pulm Med 1998; 4: 31–35.
16. Ogirala RG, Aldrich TK, Prezant DJ, Sinnett MJ, Enden JB, Williams MH Jr. High-dose intramuscular triamcinolone in severe, chronic, life-threatening asthma. N Engl J Med 1991; 324: 585–589.
17. Arnold HL Jr. Safer long-term steroid therapy with injected triamcinolone acetonide. Int J Dermatol 1978; 17: 216–217.