Gui Jun Yun1* Kyung Min Kim1* Yun-Jeong Bae1, You Sook Cho1, Hee-Bom Moon1, Jaechun Lee2# and Tae-Bum Kim1#
1Division of Allergy and Clinical Immunology, Department of Medicine, Asan Medical Center, University of Ulsan College of Medicine, 388-1 Pungnap-2dong, Songpa-gu, Seoul, 138-736, Korea, and 2Department of Medicine, School of Medicine, Jeju National University, Jeju, Korea. *E-mail: allergy@medimail.co.kr
*These authors contributed equally to this article and should be considered as first authors. # These authors should be considered as corresponding authors.
Accepted February 2, 2010.
Although angioedema, a condition characterized by swelling of the deeper layers of the skin, is common, its aetiology remains unknown in the majority of cases (80–90%) (1). We have described previously a 32-year-old woman with a variant of idiopathic angioedema presenting as facial swelling with a duration of more than one year (2). We now wish to report that after 7 months she was diagnosed with NK/T-cell lymphoma and died suddenly.
case report
At her first visit to the allergy clinic at Asan Medical Center, the patient had prolonged facial swelling, of more than one year duration, which was so severe that she was sometimes unable to open her eyes (Fig. 1A). At that time, the patient had no familial history of angioedema, exposure to drugs, foods, or chemicals, and no associations were found. Before treatment, laboratory assays were normal, including erythrocyte sedimentation rate (ESR), auto-antibodies, serum concentration of C1q, C3, C4, and C1 inhibitor, except for mild leucopaenia. Bone marrow aspiration and biopsy results were all normal. Skin biopsy did not show any evidence of lymphoma (Fig. 1B). Computed tomography (CT) scans did not show any evidence of a smouldering lymphoma. She was treated with systemic corticosteroid therapy, which reduced the swelling within a few days. After the swelling had disappeared almost completely, administration of systemic corticosteroids was tapered out. Although laboratory examinations were performed several times, no abnormalities were found, except for leucopaenia and anemia.
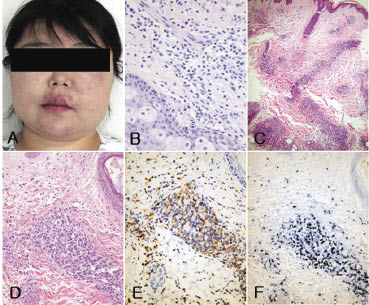
Fig. 1. (A) Prolonged facial swelling with a duration of more than one year. (B) Skin biopsy showing dense lymphocyte infiltration into the deep dermis with no evidence of lymphoma at first admission (haematoxylin and eosin (H&E) original magnification ×400). (C–F) Punch biopsy of the skin lesion from the forehead taken during a visit to the emergency room 7 months after her first visit. (C) Scanning view showing a patchy perivascular and periadnexal infiltrate in the reticular dermis and subcutis, sparing the epidermis and papillary dermis (H&E ×25). (D) High magnification of the perivascular infiltrate in the upper dermis showing a dense collection of large atypical lymphocytes (H&E ×400), positive for: (E) CD56; and (F) Epstein-Barr virus (by in situ hybridization). Fig. 2A is adopted from ref 2 with permission.
Seven months after her first visit, the patient visited the emergency room at Jeju University Hospital with fever. A complete blood count revealed pancytopaenia with 14% immature cells, suggesting leukaemia. Bone marrow examination could not be performed due to her poor general condition. The next day, she was found to have 88% blasts, with progressive liver and renal failure, and she died the same day. A skin biopsy from her forehead showed a predominantly dermal lymphocytic infiltrate with extension into the superficial subcutis (Fig. 1C). The vascular plexuses and the skin appendages in the reticular dermis showed heavy infiltration by large atypical lymphocytes with irregularly shaped nuclei, hyperchromasia, inconspicuous nucleoli, and variable amounts of pinkish to amphophilic cytoplasm, admixed with small mature lymphocytes, plasma cells and some macrophages. While the infiltrate was angiocentric, there was no evidence of angioinvasion with destruction of the vascular wall, or skin necrosis (Fig. 1D). However, the infiltrated cells were positive for CD56, suggesting extranodal NK/T-cell lymphoma of the nasal type (Fig. 1E). In situ hybridization for Epstein-Barr virus was also positive (Fig. 1F). A review of the initial skin biopsy was also positive for CD56, which means that the initial facial angioedema might include some infiltrates of NK/T-cell lymphoma cells, although this could not explain all angioedema (figure not shown).
DISCUSSION
Several reports have evaluated the relationship between acquired angioedema and lymphoproliferative diseases, most notably chronic lymphocytic leukaemia (3–5). Acquired angioedema in patients with lymphoproliferative disorders has been attributed to intermittent activation of the complement system by membrane components of neoplastic cells or by abnormal circulating immunoglobulins and depression of C1 inhibitor activity (5). This patient had normal serum levels of complements and C1 inhibitor while having NK/T-cell lymphoma. Normal concentrations of C1 inhibitor at diagnosis of angioedema is thought to be due to functionally abnormal C1 inhibitor (5).
The second unusual point is that her leukaemia, which arose from an NK/T-cell lymphoma, developed suddenly, 20 months after the first symptoms of angioedema and 7 months after its evaluation. In comparison, a previous case report described a 43-year-old man who presented with long-standing angioedema, with a duration of 6 years, and was diagnosed with lymphocytic lymphoma of intermediate differentiation (6).
In conclusion, the development of a facial NK/T-cell lymphoma should be considered in patients with long-standing angioedema.
REFERENCES