


Louise K. Andersen1, Julia S. Lehman1,2 and Mark D. P. Davis1
Departments of 1Dermatology, and 2Laboratory Medicine and Pathology, Mayo Clinic Rochester, Minnesota, USA
Calciphylaxis causes calcification, thrombosis, cutaneous ischemia, and necrosis in the skin and subcutaneous tissue. It is unclear to what extent it involves other organs. To identify whether other organs are affected we reviewed pathology reports of patients with calciphylaxis who underwent autopsy at Mayo Clinic, Rochester, Minnesota, between January 1, 1970, and December 31, 2011. Three patients were identified: two patients had a diagnosis of end-stage renal disease secondary to diabetes mellitus before the diagnosis of calciphylaxis; the third patient had calciphylaxis associated with metastatic cholangiocarcinoma without end-stage renal disease. Autopsy reports showed that despite evidence of vessel calcification elsewhere, there was no evidence of calciphylaxis in other organs. All patients had histopathologic evidence of cardiovascular calcification, and atherosclerosis of coronary arteries and aorta. Calcification of pancreatic vessels and renal vessels was also noted. In this study population, calciphylaxis was a cutaneous process alone. Key words: autopsy; calcific uremic arteriolopathy; calciphylaxis.
Accepted Apr 2, 2013; Epub ahead of print Oct 3, 2013
Acta Derm Venereol 2013; 93: XX–XX.
Mark D. P. Davis, MD, Department of Dermatology, Mayo Clinic, 200 First St SW, Rochester, MN 55905, USA. E-mail: davis.mark2@mayo.edu)
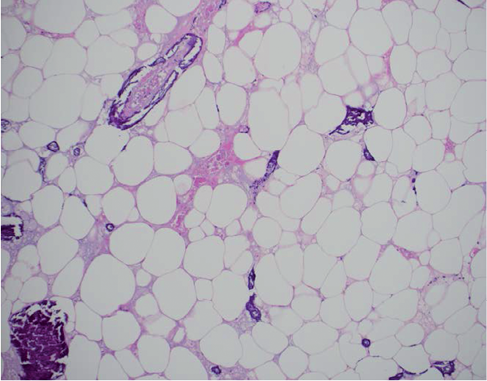
Calciphylaxis is a syndrome of vascular calcification, thrombosis, cutaneous ischemia, and necrosis (1). The diagnosis requires clinicopathologic correlation. Affected patients have clinical findings of painful indurated subcutaneous patches with overlying violaceous ischemic or infarctive skin involvement that progress to ulceration. Microscopic findings include cutaneous ischemia and necrosis due to calcification, intimal fibroplasia, and thrombosis of pannicular arterioles (Fig. 1). Calciphylaxis has been reported most commonly in patients with dialysis-dependent renal failure, although it can occur in many other clinical settings (2–5). The prognosis is dismal for patients with calciphylaxis, with an estimated one-year survival of 45.8% (1).
Fig. 1. Microscopic examination of subcutaneous tissue of a patient with calciphylaxis (hematoxylin-and-eosin stain). Pertinent features include intraluminal and extravascular calcification, intimal fibrosis of vessel walls, fat necrosis, and vascular thrombosis.
Whether calciphylaxis is a systemic process or is confined to the skin and subcutaneous tissue is unknown, since no formal studies have addressed this question. Calciphylaxis has been reported anecdotally to affect visceral organs in the setting of cutaneous calciphylaxis (6–10). In these cases, however, this conclusion rested on the presence of calcification of visceral blood vessels, a non-specific microscopic finding in patients with concomitant peripheral vascular disease. To investigate this question, we retrospectively reviewed the autopsy reports of patients at our institution with calciphylaxis to characterize extracutaneous findings related to vascular or tissue calcification or tissue ischemia. We also reviewed the medical literature to identify additional reported autopsy findings in patients with calciphylaxis.
METHODS
We used the institutional medical index and text retrieval system to identify patients who 1) had received a diagnosis of calciphylaxis, calcific uremic arteriolopathy, vascular calcification, cutaneous necrosis syndrome, or calcifying panniculitis; and 2) underwent autopsy at Mayo Clinic, Rochester, Minnesota, between January 1, 1970, and December 31, 2011. Patients were excluded if they had denied research authorization or did not meet inclusion criteria. The Mayo Clinic Institutional Review Board approved this study. We reviewed all autopsy reports and microscopically examined representative archived tissue sections from extracutaneous organs reported to have calcification.
Definition of calciphylaxis
For the purposes of this study, we defined calciphylaxis as the clinical findings of indurated patches with ischemia or infarction and ulceration, with supportive histopathologic findings of tissue ischemia and necrosis due to arteriolar calcification, extravascular calcification, intimal fibroplasia, and thrombosis (1).
RESULTS
Description of patients studied
Three patients (2 women; 1 man) met the study inclusion criteria. The mean ± SD age at onset of calciphylaxis was 58.3 ± 5.1 years. Two patients had been diagnosed with end-stage renal disease secondary to diabetes mellitus before developing calciphylaxis. Both of these patients had been treated with hemodialysis. The third patient received a diagnosis of calciphylaxis associated with metastatic cholangiocarcinoma without end-stage renal disease. The treatment of this patient was previously described previously (11).
Antemortem skin biopsies substantiated a clinical diagnosis of calciphylaxis in all 3 patients (Fig. 1). Survival after diagnosis of calciphylaxis ranged from 19 to 331 days. The mean ± SD age at death was 58.7 ± 5 years. All 3 patients died from serious infections. Two of the study patients had sepsis due to necrotic skin ulcers. The third patient developed sepsis due to pneumonia. Table I summarizes the clinical characteristics of the 3 patients. Fig. 2 shows the clinical presentation of calciphylaxis in each of the 3 patients.
Table I. Characteristics of the 3 patients with calciphylaxis who were autopsied after death
|
Pat. No./Sex |
Age, years |
Medical history |
Dialysis |
Antemortem skin biopsy |
Survival after diagnosis, days |
Primary cause of death |
||
|
At onset |
At death |
|||||||
|
1/F |
64 |
64 |
End-stage renal disease; diabetes mellitus type 2; hypertension; stable coronary artery disease |
Yes |
Yes |
33 |
Sepsis due to necrotic calciphylaxis skin ulcers |
|
|
2/M |
57 |
58 |
End-stage renal disease; insulin-dependent type 2 diabetes; hypertension; dilated cardiomyopathy; antiphospholipid syndrome; hypothyroidism; alcoholism; penile gangrene; amputation at knee |
Yes |
Yes |
331 |
Sepsis due to pneumonia |
|
|
3/F |
54 |
54 |
Metastatic cholangiocarcinoma; diabetes mellitus type 2; deep vein thrombosis; frontal subdural hematoma |
No |
Yes |
19 |
Sepsis due to necrotic calciphylaxis ulcers |
|
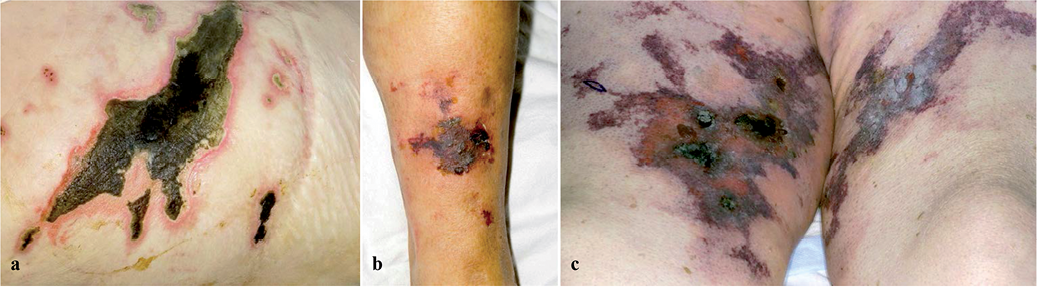
Fig. 2. The clinical presentation of calciphylaxis in each of the 3 patients. Lesions mainly on right buttock of Patient 1 (a). Lesions on left lower leg of Patient 2 (b). Lesions on both thighs of Patient 3 (c).
Autopsy reports
Autopsy reports are summarized in Table II.
Skin involvement: Skin biopsies were consistent with calciphylaxis. Anatomic distribution of calciphylaxis was reported on autopsy as involving upper extremity (n = 1), torso (n = 1), and lower extremity (n = 3).
Systemic involvement: Representative archived tissue sections from extracutaneous organs reported to have calcification were examined microscopically: none had histologic evidence to support calciphylaxis of the extracutaneous organs: specifically, none had evidence of extravascular calcification, vessel thrombosis, tissue ischemia, or luminal fibrosis.
Table II. Autopsy results of the 3 patients with calciphylaxis
|
Pat. No. |
Skin involvement with calciphylaxis by anatomical site |
Extracutaneous findings of calcification or vascular damage |
||||||||
|
Torso |
Lower extremity (including buttocks) |
Upper extremity |
Head |
Neck |
Atherosclerosis of aorta and coronary arteries |
Calcification of heart valves |
Calcification in other organs |
Calciphylaxis in other organs |
||
|
1 |
Yes |
Yes |
No |
No |
No |
Yes |
Mitral; aorta |
No |
No |
|
|
2 |
No |
Yes |
Yes |
No |
No |
Yes |
No |
No |
No |
|
|
3 |
No |
Yes |
No |
No |
No |
|
Yes |
Mitral |
Pancreas; kidney |
No |
The autopsy reports indicated that all 3 patients had histopathologic evidence of cardiovascular calcification (Fig. 3a), and atherosclerosis of the coronary arteries and aorta. Calcification of pancreatic vessels (n = 1) and renal vessels (n = 1; Fig. 3b) was also noted. Two patients had annular calcification of the heart valves (mitral [n = 2] and aortic [n = 1]).
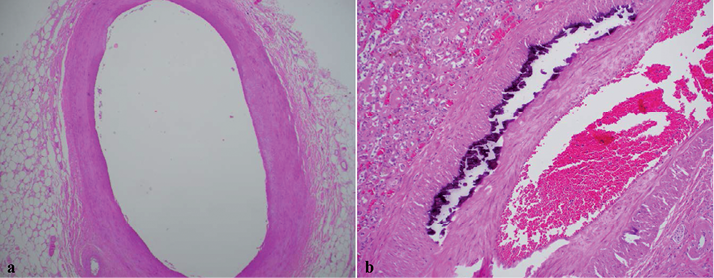
Fig. 3. Microscopic findings from autopsies (hematoxylin-and-eosin stain): (a) Aortic atherosclerosis, grade 1 (of 4), non-ulcerocalcific. Microscopic features of calciphylaxis are not present (b) Monkeberg medial calcification of a renal artery, with the changes of severe diabetic nephropathy, acute tubular injury, and mild interstitial chronic inflammation. Microscopic changes of calciphylaxis, including extravascular calcification, intramural thrombosis, and intimal fibrosis of the vessel walls, are not present.
Thus, although vessel calcification was identified in other organs, other microscopic features of calciphylaxis were not reported to be present in organs other than the skin.
DISCUSSION
The histopathologic diagnosis of calciphylaxis in any organ system requires the presence not only of vascular and tissue calcification but also of associated tissue necrosis. Other findings, such as vascular occlusion by thrombi and intraluminal fibrosis, may support the diagnosis. Calcification in unusual anatomical locations or that it is extensive is insufficient for a diagnosis of systemic calciphylaxis. Calciphylaxis was identified only in the skin of these 3 patients. Although intra- and extravascular calcium deposition was noted in other organs, associated tissue ischemia or necrosis (as required for calciphylaxis) was not reported. The extracutaneous calcium deposition noted postmortem in these patients was related to comorbidities, including diabetes mellitus, atherosclerosis, and end-stage kidney disease. Therefore, although patients with calciphylaxis not surprisingly have systemic evidence of chronic vascular stress and injury, the pathophysiology of calciphylaxis appears to have been confined to the skin in these patients.
We chose to study the autopsy data from these patients because postmortem examination is more thorough and systematic than antemortem physical examination, biopsy findings, or imaging studies. Scattered case reports have reported autopsy findings in patients with calciphylaxis (Table III) (6–8, 11–21). The vast majority of the reports document vascular calcification but not calciphylaxis of these internal organs (defined as in methods); in only 2 case reports would criteria perhaps fit with these criteria. One reported “extensive vascular calcium deposition within multiple mesenteric vessels in the small bowel, with full-thickness necrosis; also in the dura” (7), and another reported “diffuse medial calcification, with intimal fibrosis and cellular thickening, partly accompanied by microthrombi involving small- to medium-sized visceral arteries” (8). Without reviewing this reported pathology, it is difficult to confirm whether or not these findings truly represented calciphylaxis of these organs.
Other reports have noted “visceral calciphylaxis” in patients on whom an autopsy was not performed or reported (9, 10). These patients had antemortem biopsies from extracutaneous organs that showed findings said to be consistent with calciphylaxis in the lungs and gastrointestinal tract. In most of these cases, calcium deposition was noted systemically, but microscopic criteria that would satisfy a diagnosis of calciphylaxis were not described. This raises the possibility that it was intra- and/or extra-vascular calcification alone that was identified rather than calciphylaxis in organs other than the skin.
The pathogenesis of calciphylaxis is not well understood. The term was coined by Hans Selye (22) in 1962 to describe skin necrosis that was provoked by exposure to substances such as parathyroid hormone and vitamin D, and it was associated with cutaneous calcification in experimental animals. The pathogenic mechanism of calciphylaxis has since been likened to “the skin equivalent of a myocardial infarction,” since vessel narrowing by intravascular calcification and fibrosis leads to tissue ischemia after an acute event such as thrombo-occlusion (23). While vascular mural calcification is not sufficient for a diagnosis of calciphylaxis, mural calcifation does appear to be an early and essential process in the development of a calciphylaxis plaque. In one postmortem study, an incisional skin biopsy specimen from a patient with calciphylaxis showed subcutaneous vascular mural calcification, extravascular calcification, which extended peripherally by as much as 3 cm, and thromboses within the dermis and subcutis (24).
We acknowledge the limitations of this review, including its retrospective design, the small number of patients with calciphylaxis who had autopsy and thus met inclusion criteria, and the possible selection bias of including only those patients on whom an autopsy had been performed. We recognize that it is difficult to extrapolate findings from 3 cases.
We conclude that in the study population, calciphylaxis was a cutaneous process alone and did not involve other organs. Our study is of just 3 patients: further autopsy studies from patients with calciphylaxis are needed to confirm or refute our findings that calciphylaxis only involved skin and does not seem to involve extracutaneous organs.
Table III. Published case reports describing postmortem results of patients with calciphylaxis
|
Author (year) |
Patient age, years/Sex |
Etiology of ESRD |
HD |
Kidney transplant |
Cutaneous involvement |
Cause of death |
Autopsy reports (calciphylaxis or calcification?) |
Meets histopathologic criteria for calciphylaxis in extracutaneous organs? |
|
Conn et al. (1973) (6) |
23/F |
Glomerulonephritis |
Yes |
Yes |
Yes |
Not reported |
Generalized medial calcification, with fibrous obliteration of the lumen of all vessels studied |
Partially |
|
Asmundsson et al. (1988) (16) |
25/F |
Hypertension |
Yes |
Yes |
Yes |
Sepsis |
Arterial calcium deposits; calcification outside vessels in heart valves and lungs |
No |
|
Edelstein et al. (1992) (20) |
50/M |
Analgesic nephropathy |
Yes |
Yes |
Yes |
Not reported |
Coronary arteries showed marked medial calcification and intimal thickening, with resultant luminal narrowing, and extensive metastatic calcification within alveolar walls |
No |
|
Tamura et al. (1995) (8) |
50/F |
Diabetes mellitus |
Yes |
No |
Yes |
Sepsis |
Diffused medial calcification, with intimal fibrosis and cellular thickening, partly accompanied by microthrombi involving small- to medium-sized visceral arteries |
Likely |
|
McAuley et al. (1997) (15) |
46/M |
Hypertension |
Yes |
No |
Yes |
Cardiac arrest |
Metastatic calcification in all organs |
No |
|
McAuley et al. (1997) (15) |
48/M |
History of hypertension; non–insulin-dependent |
Yes |
No |
Yes |
Sepsis |
Widespread calcification of small vessels, including the coronary vasculature |
No |
|
Brown et al. (1998) (13) |
38/F |
Diabetes mellitus |
Yes |
No |
Yes |
Sepsis |
Diffuse ulceration of all segments of large intestine without specific microscopic findings; widespread medial calcification in many organ systems, including myocardium, lung, and kidney |
No |
|
Oh et al. (1999) (12) |
54/M |
Cyclosporine-induced nephrotoxicity |
Yes |
Yes |
Yes |
Sepsis |
No parenchymal involvement by calciphylaxis |
No |
|
Oh et al. (1999) (12) |
40/F |
Lupus nephritis |
Yes |
No |
Yes |
Sepsis |
Extensive ulcers and calcium deposits in parenchyma and vascular walls of multiple viscera |
No |
|
Kloeppel et al. (2001) (17) |
30/F |
Unknown etiology |
Yes |
Yes |
No |
Progressive heart failure |
Extended calcifications of the entire myocardium; peripheral vessel calcifications |
No |
|
Matsuo et al. (2001) (18) |
57/M |
Glomerulonephritis |
Yes |
No |
No |
Not reported |
Calcium deposits in alveolar septal capillary walls of the lung |
No |
|
Riegert-Johnson et al. (2001) (11)a |
54/F |
No kidney disease (metastatic cholangio-carcinoma) |
No |
No |
No |
Sepsis |
Extensive mitral annular calcification and intramyocardial calcification |
No |
|
Pliquett et al. (2003) (19) |
53/F |
Hypertension; recurrent ascendant UTI and renal atherosclerosis were likely causes of renal failure |
No |
No |
Yes |
Sepsis |
Unusual locations of calcifications were the wall of the left atrium of the heart and the pulmonary arteries |
No |
|
Suryadevara et al. (2008) (21) |
11/M |
No kidney disease (systemic calciphylaxis developed during induction therapy for ALL) |
No |
No |
No |
Cardiac arrest |
Extensive calcium deposition in the visceral organs, involving the heart, lungs, and kidneys |
No |
|
Volpini & Kinonen (2011) (7) |
43/F |
Glomerulosclerosis |
Yes |
No |
Yes |
Abdominal catastrophe |
Extensive vascular calcium deposition within multiple mesenteric vessels in the small bowel, with full-thickness necrosis; also in the dura |
Likely |
|
Alam et al. (2012) (14) |
45/M |
Not reported |
Yes |
No |
Yes |
Not reported |
Large areas of calcification present within the media of the coronary vessels and within the myocardium |
No |
aOur patient no. 3
ALL: acute lymphoblastic leukemia; HD: hemodialysis; UTI: urinary tract infection.
The authors declare no conflicts of interest.
REFERENCES

