


1Department of Dermatology & Venereology, Karolinska University Hospital Solna, SE-171 76 Stockholm, and 2Department of Gastroenterology and Hepatology, Karolinska Institutet and Karolinska University Hospital, Stockholm, Sweden. E-mail: toomas.talme@sll.se
#These authors contributed equally to the article.
Accepted Apr 18, 2017; Epub ahead of print Apr 19, 2017
Methotrexate (MTX) can provide remission and is recommended as first-line systemic therapy for psoriasis (1). However, despite reasonable efficacy, its use is restricted by concerns regarding the risk of developing liver fibrosis (2). Liver biopsy, which is considered the gold standard for assessment of fibrosis, is invasive and has become less accepted for monitoring liver injury during long-term treatment with MTX (3, 4). Several scoring systems based on laboratory parameters have therefore been created to identify liver fibrosis (5–7). Serial monitoring of the amino terminal of type III procollagen peptide (PIIINP) is proposed as an alternative for liver biopsy (8, 9).
Several studies have shown that transient elastography (TE) may be useful for monitoring patients treated with MTX (10, 11). We have identified several cases of advanced liver fibrosis confirmed with liver biopsies despite normal levels of PIIINP. The aim of this case-control study in a cohort of patients with psoriasis treated with MTX was to compare TE measurements with serological markers for liver fibrosis.
Consecutive psoriasis patients ≥ 18 years old requiring systemic treatment were recruited prospectively between 2012 and 2015. The study was approved by the regional ethics committee (Dnr: 294/576-32). Patients with hepatitis were excluded. Patients on MTX were stratified into 2 groups: treatment ≤ 24 months (range 1–24 months) (n = 47) and treatment > 24 months (range 25–432 months) (n = 122). Patients receiving biologicals as single systemic treatment, who had received MTX for a maximum of 6 months >4 years ago, served as controls (n = 32). Most patients were treated with 10–20 mg MTX once weekly.
Liver stiffness measurements were performed using FibroScan 502 (Echosens, Paris, France) (12). Most patients were examined with the M-probe, but for obese patients the XL probe was used. Ten validated TE measurements and interquartile range (IQR) < 30% of median liver stiffness were deemed reliable. We used 6.5 kilopascal (kPa) (5.5 kPa with the XL–probe) as a cut-off value for mild fibrosis (grade 1–2), and 11.5 kPa (10 kPa XL–probe) for severe fibrosis (grade 3–4) and cirrhosis (13).
The following laboratory parameters were determined in blood: aspartate transaminase (AST) (laboratory reference < 0.76 µkat/l), and alanine transaminase (ALT) (< 1.20 µkat/l), platelet count (165–387 × 109/l) and PIIINP (300–800 IU/l). AST/ALT > 0.8 ratio was used as a cut-off for possible liver fibrosis and a ratio > 1.0 indicating cirrhosis (5). The AST to Platelet Ratio Index (APRI) score was calculated as AST (IU/l)/(upper limit of normal)/platelet count (×109/l)×100. Values for APRI > 0.7 were used to predict fibrosis and >1.0 to predict cirrhosis (6). The Fibrosis-4 (FIB-4) score was calculated as age × AST (IU/l)/platelet count (× 109/l) × √ALT (IU/l) and a score > 1.45 was used to predict fibrosis and >3.25 to predict cirrhosis (7).
Results are expressed as odds ratio (OR), with 95% confidence interval (95% CI) and corresponding p-values. Significance was set at p-values below 0.05. Comparisons of quantitative data were made using Student’s t-test. When data did not exhibit a normal distribution Kruskal–Wallis rank sum test was used for testing 3 groups and Wilcoxon rank sum test with continuity correction was used for testing 2 groups. Normal distribution was tested with Shapiro–Wilk test of normality. A χ2 test was used to check for differences between groups. Statistical analyses of confounders were performed with GLM in R program v 3.1.3 (http://www.r-project.org/).
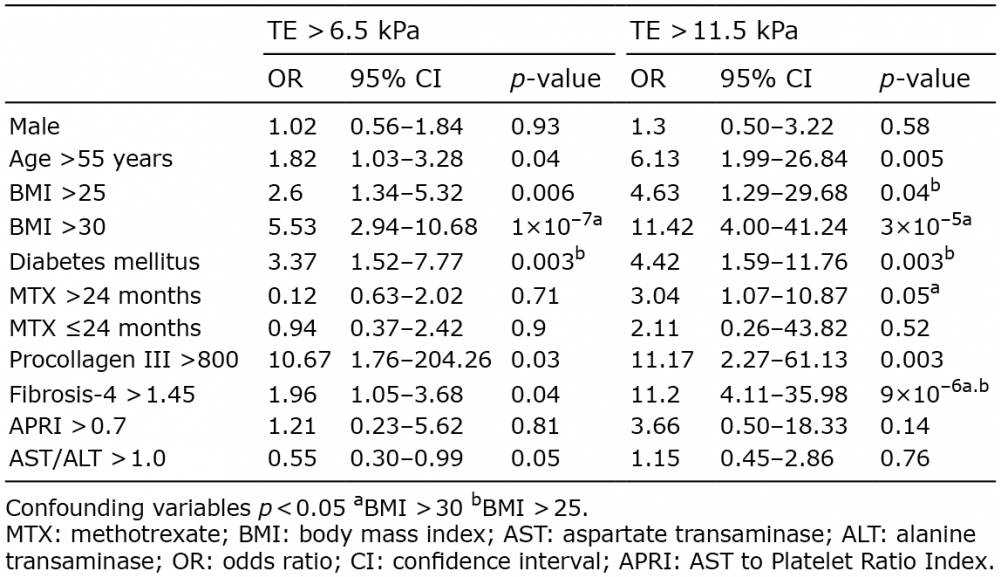
A total of 201 consecutive psoriasis patients were included in this study (Fig. S1). Demographic and clinical characteristics of the study population are shown in Table SI. There was no statistical difference in median liver stiffness between the 3 groups. Of those who received MTX > 24 months, 46 out of 122 patients (37.7%) had a liver stiffness indicating mild liver fibrosis, and 11 patients (9.0%) indicating severe fibrosis. In patients who received MTX ≤ 24 months 15 out of 47 (31.9%) had a liver stiffness indicating mild fibrosis, and 3 (6.4%) indicating severe fibrosis. In the control group 12 out of 32 patients (37.5%) had a liver stiffness indicating mild liver fibrosis, and 1 (3.1%) indicating severe fibrosis (Table SI). Statistical analysis showed that a body mass index (BMI) >30 and diabetes were the strongest predictors for liver fibrosis (Table I).
Table I. Factors associated with transient elastography (TE)
There was no statistical difference in median values for APRI, AST/ALT– ratio or FIB-4 between the 3 groups. In patients with TE measurements indicating advanced fibrosis APRI > 0.7 was seen in 20%, AST/ALT-ratio > 1.0 in 46.7% and FIB-4 > 1.45 in 66.7% of these cases. PIIINP was measured in 36 out of 47 patients treated with MTX ≤ 24 months and in 120 out of 122 patients treated with MTX > 24 months. Six patients showed elevated PIIINP and all had received MTX treatment > 24 months (Table SI). In 14 patients with TE values indicating advanced fibrosis only 4 showed an elevation in PIIINP. Two patients with elevated PIIINP had normal TE values. Eight patients with a TE indicating severe liver fibrosis/cirrhosis were examined with liver biopsy. Six of these were confirmed as advanced liver fibrosis grade 3. In the remaining 2 the fibrosis was evaluated as mild (Table SII). Six patients were examined with abdominal ultrasound, which showed liver fibrosis and/or steatosis and, in 4 of them, signs of liver cirrhosis (Table SII). One patient underwent a magnetic resonance imaging (MRI) examination, which showed liver cirrhosis.
It is likely that MTX will remain a common treatment for severe psoriasis because of its long-established safety profile and low cost. Several studies have shown that the cumulative MTX dose does not associate with an abnormal TE result, suggesting that alternative factors play a significant role in fibrosis development (10, 11). In line with previous studies (14) we found that a BMI >30 and diabetes mellitus were significantly associated with increased TE values indicating liver fibrosis (Table I).
Increased levels of PIIINP occur as a consequence of tissue repair and fibrosis. Serial measurements of PIIINP have been advocated as a reliable non-invasive test for ongoing hepatic fibrogenesis (8, 9). As a consequence, many dermatologists have stopped referring patients for liver biopsies. In the present study only 4 of the 14 patients with TE values indicating advanced fibrosis showed an elevation in PIIINP. Notably, high serum PIIINP is not specific for liver fibrosis (15). PIIINP levels are high in children and adolescents as a result of physiological growth. Increased collagen turnover and raised PIIINP levels may occur in inflammatory arthritis, and psoriatic arthritis affects approximately one-third of patients with psoriasis. Also, liver cirrhosis may not be detected by determining PIIINP levels when inflammation is minimal.
The limitations of our study are that only patients with TE values indicating severe liver fibrosis were examined with liver biopsy and/or ultrasound and that no specific markers for alcohol were investigated. The control group also contained fewer patients than the 2 MTX groups.
In conclusion, many patients with psoriasis have pre-existing risk factors for liver disease, and advanced liver fibrosis is not uncommon among patients with severe psoriasis requiring systemic treatment. Serial PIIINP monitoring alone may not be sufficient to reveal liver fibrosis in psoriasis patients on MTX treatment. In addition to serum markers, monitoring with TE can improve the detection of clinically significant liver fibrosis, especially in patients with pre-existing risk factors. We therefore propose recurrent TE measurements as a simple non-invasive method to increase safety in patients receiving long-term treatment with MTX (Fig. S2).
This study was supported by grants from Medical Research Council, Psoriasis Foundation, the Welander Finsen Foundations and the Stockholm County Council. The authors would like to thank Ingrid Ackzell and Helena Griehsel for technical support in this study.
Disclosure: TT has participated in advisory boards or panels and given lectures for Abbvie, Celgene, Eli Lilly, Jansen, Merck, Novartis, Pfizer Inc, and UCB. MS has participated in advisory boards or panels and given lectures for Abbvie, Celgene, Eli Lilly, Jansen, Novartis, Pfizer Inc, and UCB.


 Click to show fullsize
Click to show fullsize