


Departments of 1Dermatology, and 2Psychiatry, Medical School, University of São Paulo, Rua Itapeva 500, 3A, CEP-01332-000 São Paulo, Brazil. *E-mail: mentanico@hotmail.com
Accepted Apr 18, 2017; Epub ahead of print Apr 19, 2017
Factitious dermatologic disorder (FDD), formerly called dermatitis artefacta or factitious dermatitis, is a disorder of self-induced behavior (1). FDD can be defined as any condition that involves self-inflicted skin lesions for which the patient denies all responsibility due to extant personality disorder (2, 3). Patients induce lesions to fulfill an unconscious psychological need (1). The clinical profile of FDD varies significantly and depends on how the patient traumatizes the skin. The lesions observed can include erosions, ulcers, eschars, blisters, nodules that follow injection of foreign material (4), and mutilation (1, 2).
We present a case of FDD who showed extraordinary radiological findings. In addition, during a psychiatric follow-up, the patient revealed her motivations in producing the lesions, prompting a discussion on her psychopathology.
A 60-year-old married woman presented with cutaneous lesions on her left lower limb that had been present for 6 months. Her husband, who was concerned about her complaints – the patient claimed to have been possessed by evil spirits – had taken her to the hospital. Since the initial presentation, the patient had been examined in many hospitals, stating that no doctor could identify the cause of her ailments.
An examination showed several irregularly shaped, well-demarcated, shallow cutaneous ulcers on the left leg and calf, with no signs of inflammation (Fig. 1). The patient affirmed that the lesions developed suddenly, without any preexisting symptoms. FDD was promptly suspected; the lower limb was X-rayed, upon insistence of the patient. On the X-ray, radio-opaque images of many intact and broken sewing needles could be seen, residing at various depths of the lower limb soft tissues (Fig. 2). The patient claimed that no person had inserted the needles into her body, and she was certain that they were the result of witchcraft. Her husband supported this theory.
Fig. 1. Multiple cutaneous ulcers.
Fig. 2. Left lower leg radiograph: lateral view (left), and front view (right) multiple self-embedded needles.
The patient was admitted to the dermatology ward and underwent a systematic psychiatric evaluation. Initially, the patient insisted on nearly solely discussing the purely cutaneous and mystic aspects of her disease, failing to provide details about her mental health. The psychiatrist’s clinical impression was that the patient showed significant emotional detachment with regard to her situation. In a subsequent psychiatric evaluation, the patient reluctantly mentioned that her husband, despite being a caring companion, was extremely short-tempered and had frequent bursts of anger that scared and intimidated her, leading her to secretly embed the needles in her body. She now started fearing that her husband would leave her if he discovered the true nature of her condition and urged the psychiatrist to keep these revelations confidential.
Presently, monthly psychiatric consultations are being held. The psychiatrist has assumed the role of mediator in resolving the emotional conflict between the patient and her husband, but the patient continues to feign illness, frequently asking to be admitted to the ward. It has been decided that the needles may remain in the body, since none of them lies near any vital structures.
Patients with FDD typically deny their behavior due to extant personality disorder and constantly develop new lesions and seek medical care (4). These cases are difficult to treat dermatologically and psychiatrically – the lesions fail to heal due to continuous manipulation, and the patient’s mental disease typically does not respond to behavioral or psychopharmacological therapy (1, 2). To this end, perseverant psychological and psychodynamic approaches have recently been advocated (5). In our case, the patient had visited many hospitals, where she had been examined, challenging the attending physicians with her striking lesions and radiological images. By arranging several medical appointments at several institutions, she managed to impersonate a sick person and receive care from her husband and doctor.
There are several notable peculiarities of our case. Even considering the high variability of lesions that can be observed in FDD, the self-insertion of dozens of needles into the skin is most unusual. Self-embedding is seen more often in adolescent patients with psychiatric comorbidities (6).
It is also unusual that a patient with this type of self-inflicted lesion acknowledges manipulation of the skin. Our patient moved from one medical institution to another, where she was always confronted by attending physicians due to the obvious artificial nature of her clinical profile. Our approach consisted of establishing a good therapeutic bond with the patient – listening attentively to what she had to say, requesting laboratory tests, prescribing topical medications, admitting her to the ward, and ultimately requesting help from the psychiatry team (5). After several psychiatric interviews, the patient admitted to inserting the needles.
We considered the case to be typical FDD, considering all elements – from the patient’s history to when she came to be in our care. At that time, we gained insights into the underlying motivation for her behavior, which was unusual in similar instances, induced by the following chain of events: her husband loses his temper; the patient becomes emotionally distressed and does not know how to respond to his behavior; acts on this feeling of helplessness by harming herself; and complains to him about her physical symptoms, causing him to develop a caring attitude toward her. Thus, the patient realizes that there is a favorable outcome to her actions.
Emotional detachment when faced with an alarming physical condition is a non-defining but common trait in factitious disorder. However, unlike patients who are diagnosed with borderline personality disorder – a facilitating psychological condition that underlies FDD – the self-harm behavior in this case did not intend to alleviate emotional distress of an ill-defined origin by replacing it with physical pain; instead, it aimed to avoid a source of distress that was clearly perceived as such from the outset. Eventually, growing anxiety led the patient to self-insert the needles to shift her husband’s behavior toward a caring stance. Her success in this endeavor had both favorable and disadvantageous effects, and she found herself juggling an increasingly complex situation. At this time, when properly questioned, she acknowledged the nature of her lesions, favoring a better rapport over a therapeutic approach, possibly improving her outcome.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize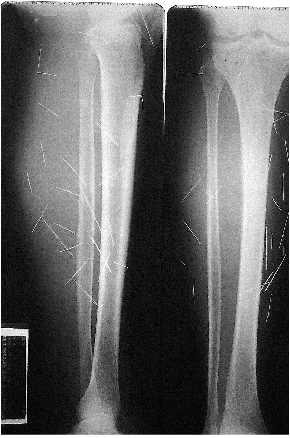 Click to show fullsize
Click to show fullsize