


1Division of Dermatology and Venereology, 3Department of Laboratory Medicine, Division of Medical Diagnostics, Region Jönköping County, Jönköping, 2Division of Drug Research, Department of Medicine and Health Sciences, and 4Department of Clinical and Experimental Medicine, Faculty of Medicine and Health Sciences, Linköping University, Linköping, Sweden
#These authors contributed equally to this work.
CD93 is involved in angiogenesis and inflammation, both of which are key processes in the pathogenesis of psoriasis. CD93 was studied in serum, peripheral blood mononuclear cells and skin of patients with psoriasis and controls. Furthermore, allele frequencies for CD93 single-nucleotide polymorphisms rs2749812 and rs2749817 were assessed in patients with psoriasis compared with controls and the effect of narrowband ultraviolet B (NB-UVB) treatment on CD93 gene expression was evaluated in the skin of patients with psoriasis. CD93 gene expression was significantly increased in lesional and non-lesional skin from patients with psoriasis compared with controls. Immunohistochemistry revealed CD93 staining in dermal endothelial cells in lesional skin, and psoriasis was significantly associated with rs2749817 CD93 gene polymorphism. NB-UVB treatment of patients with psoriasis did not alter skin CD93 gene expression. Increased protein expression of CD93 psoriatic skin and association with the rs2749817 polymorphism suggests that CD93 plays a role in psoriasis disease pathogenesis.
Key words: psoriasis; CD93; angiogenesis; single nucleotide polymorphism; ultraviolet B; phototherapy.
Accepted Apr 18, 2017; Epub ahead of print Apr 19, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Albert Duvetorp, Division of Dermatology, Ryhov Hospital, SE-55185 Jönköping, Sweden. E-mail: albert.duvetorp@rjl.se
Psoriasis is a chronic inflammatory skin disease characterized by activated innate immunity, altered differentiation and hyperproliferation of keratinocytes and angiogenesis (1). In lesional skin of patients with psoriasis, dermal papillae are elongated and dilated blood vessels are present. In fact, angiogenesis and vascular changes are early signs in psoriasis, being detectable even before visible epidermal hyperplasia (2).
High levels of pro-angiogenic factors, such as vascular endothelial growth factor (VEGF), interleukin 17 (IL-17), interferon (IFN)-γ, tumour necrosis factor (TNF)-α, angiopoietins and hypoxia inducible factor (HIF), are present in lesional skin (2), and it is suggested that many of the current systemic therapies for psoriasis are not solely immune modifiers, but also inhibit angiogenesis. Recent case reports have shown that vascular endothelial growth factor (VEGF)-inhibitors used in anti-tumour therapy can improve the clinical appearance of psoriasis (3, 4). Targeting angiogenesis may be a new future treatment strategy for psoriasis (5).
Recent studies suggest that CD93 may have implications in inflammation and inflammatory diseases as well as in angiogenesis (6). CD93 is a transmembrane glycoprotein that, together with human endosialin and thrombomodulin, constitutes a small family of transmembrane proteins with epidermal growth factor (EGF)-like domains (7, 8). CD93 is mainly expressed in endothelial cells, but is also present in granulocytes, monocytes, platelets and stem cells (9–13). The EGF-like domains of CD93 induces endothelial cell proliferation and migration in vitro and stimulates angiogenesis in vivo (14). 4E1, a monoclonal antibody against CD93 has been shown to inhibit angiogenesis, both in vitro and in vivo, without affecting endothelial cell survival (15). Previous studies suggest that the expression of CD93 on endothelial cells may also play a role in the regulation of cell adhesion and in the skin homing of inflammatory cells (10, 16, 17), which are important steps in initiating and maintaining inflammation in psoriasis (18).
At present, there are no studies on CD93 in psoriasis. The aim of this study is to analyse CD93 expression in non-lesional and lesional skin, in peripheral blood mononuclear cells (PBMCs) and serum of patients with chronic plaque-type psoriasis compared with healthy controls. Two CD93 single-nucleotide polymorphisms (SNPs; rs2749812 and rs2749817) previously associated with increased risk for cardiovascular disease and cancer development (19, 20) were analysed for a genetic association with psoriasis.
Narrowband UVB (NB-UVB) is a well-tolerated and effective treatment for psoriasis. The anti-inflammatory effect of NB-UVB is partly explained by increased T-cell apoptosis, reduced epidermal proliferation and inhibition of angiogenesis (21–29). To investigate a possible role of CD93 in the anti-inflammatory effect of NB-UVB CD93 gene expression was analysed in psoriasis patients before and after receiving a full standard NB-UVB regime.
All patients with chronic plaque psoriasis were recruited from the outpatient clinic at the Division of Dermatology, Ryhov Hospital, Jönköping, Sweden. Skin biopsies from healthy controls were obtained from patients with benign naevi at the same clinic. Serum samples from healthy controls were obtained from blood donors with no known history of psoriasis from the Ryhov Hospital, Jönköping, Sweden. This study was conducted in compliance with good clinical practice and according to the principles of the Declaration of Helsinki. Written informed consent was obtained from all subjects under protocols approved by the ethics committee at Linköping University, Linköping, Sweden (Dnr 243-08 and Dnr 2014/353-32). Sex and age was recorded for all individuals and an assessment of disease severity using the Psoriasis Area and Severity Index (PASI) were recorded for subjects with psoriasis. Patients’ demographic data are summarized in Table I.
Table I. Patient’s demographic data, illustrating patient’s sex, Psoriasis Area and Severity Index (PASI) and age
Analysis performed and the number of individuals included for each analysis are illustrated in Fig. 1. The patient population undergoing NB-UVB treatment was included separately and were not subject for other analysis than CD93 gene expression before and after NB-UVB treatment. Study participants subject to skin biopsy did not use any systemic or topical anti-psoriatic treatments 2 weeks prior to study inclusion.
Fig. 1. Number of patients with chronic plaque psoriasis (n) and controls (c) included in the different parts of the study regarding to the CD93 analysis performed. nb: narrow band, PBMC: peripheral blood mononuclear cell. aBecause of an error during laboration one sample was lost and only 109 were available for subsequent allele analysis.
Full-thickness punch biopsies for CD93 gene expression and immunohistochemistry (IHC) were taken from non-lesional skin (at least 10 cm distance from any psoriatic lesion; 4 mm diameter) and from the active margin of a psoriatic plaque (4 mm diameter) after application of local anaesthetics. Biopsies were obtained from corresponding anatomical sites from healthy controls. Immediately upon removal, biopsies were stored in either formalin for IHC or RNAlater RNA Stabilization Reagent (Qiagen, Hilden, Germany) for gene expression analysis and stored at –80°C.
Whole-blood samples were taken from patients with psoriasis and controls for genotyping and CD93 protein analysis in serum and in PBMCs. Blood samples were stored at –80°C prior to subsequent analysis. Mononuclear cell separation was carried out in a BD Vacutainer CPT (BD Biosciences, Franklin Lakes, NJ, USA) according to the manufacturer’s instruction. PBMCs were counted using Sysmex XE-5000 (Sysmex Europe GmbH, Norderstedt, Germany) before freeze media containing foetal calf serum (FCS) and dimethylsulphoxide (G-Biosciences, MO, USA) was added. The samples were stored at –80°C for 24 h before they were moved and stored at –150°C prior to subsequent analysis.
For analysis of CD93 gene expression in response to NB-UVB treatment, full-thickness 2-mm punch biopsies were taken after application of local anaesthetics from a single psoriatic plaque and non-lesional skin of patients before and after performing a full NB-UVB treatment series according to standard clinical protocol at the Division of Dermatology, Ryhov Hospital. The location of the biopsies before treatment was recorded to ensure that biopsies after treatment were taken from approximately the same location.
CD93 staining was performed using a standard protocol on 4-µm sections from formalin-fixed paraffin-embedded tissue blocks, as described previously (30). Sections were subsequently incubated with a primary goat anti-human C1qR1/CD93 antibody (0.2 μg/ml; R&D Systems, Inc., MN, USA) overnight at 4°C, and then with a horse secondary biotinylated affinity purified anti-goat IgG antibody (1.5 μg/ml; Vector Laboratories Ltd, Burlingame, CA, USA). Avidin-biotin peroxidase complexes (Vector Laboratories) were added, followed by visualization with 3.3’-diaminobenzidine (Vector Laboratories). Sections were counterstained with haematoxylin (Vector Laboratories) and rehydrated before cover-slips were added. Microscopy of the sections was performed using a Zeiss light microscope (Carl Zeiss Microscopy GmbH, Göttingen, Germany) along with the Zen lite software (Zeiss)). As a control, IHC was performed without the primary antibody and only with the horse secondary biotinylated affinity purified anti-goat IgG antibody (1.5 μg/ml; Vector Laboratories) to exclude any possible background effects.
Total RNA was purified according to the manufacturer’s instructions. Briefly, biopsies were homogenized using a TissueRuptor and disposable probes (Qiagen, Hilden, Germany), and RNA was purified using the RNeasy Fibrous Tissues mini kit (Qiagen). Concentration and purity was measured using a Nanodrop ND-1000 (Thermo Fisher Scientific Inc., Waltham, MA, USA), and RNA integrity was assessed using the RNA integrity number with a 2100 Bioanalyzer (Agilent Technologies, Santa Clara, CA, USA).
RNA was reverse transcribed using the high-capacity cDNA reverse transcription kit with RNase inhibitor (Applied Biosystems, Waltham, MA, USA), according to the manufacturer’s instructions, and the resulting cDNA was stored at –80°C.
Gene expression was analysed on the 7500 Fast real-time PCR system (Applied Biosystems) and the standard run mode using Taq-Man Universal Master Mix no UNG (Applied Biosystems) and Taqman Gene Expression Assays (Applied Biosystems) for CD93 (Hs00362607_m1), TBP (Hs00427620_m1), ACTB (Hs99999903_m1) and GAPDH (Hs03929097_g1). For each assay and sample, cDNA based on 10 ng total RNA were analysed in a total volume of 20 μl.
Threshold cycle (Ct) values were established using the 7500 software version 2.0.6 (Applied Biosystems). Reference genes (TBP, ACTB and GAPDH) were evaluated for low sample-to-sample variation using the NormFinder (31) algorithm implemented in the GenEx Professional software version 5.4.2.128 (MultiD Analyses AB, Göteborg, Sweden). CD93 Ct values were normalized to the TBP reference gene showing the best stability value. Relative gene expression was compared using the comparative Ct (2–ΔΔct) method (32).
CD93 was measured in serum and in PBMCs using a commercial enzyme-linked immunosorbent assay (ELISA) kit (R&D Systems Europe Ltd, UK) and performed as described previously (20). CD93 levels were determined using the Sunrise Tecan Microplate Reader (Tecan Austria GmbH, Salzburg, Austria) along with the Magellan 7.x 2010 software (Tecan). CD93 levels in patients and controls were expressed as ng/ml.
DNA was extracted from whole blood using the QiaAmp DNA blood kit (Qiagen). 10 ng of each DNA sample was genotyped using the TaqMan Universal PCR Master mix II (Applied Biosystems), TaqMan SNP genotyping assays rs2749812 and rs2749817 (Applied Biosystems assay-IDs C__3206246_10 and C__16068002_10, respectively), and the 7500 Fast Real-Time PCR system (Applied Biosystems).
Statistical evaluation of multiple groups was performed using Kruskal-Wallis analysis of variance (ANOVA) followed by Mann–Whitney U test as a post hoc test used to compare 2 groups. Wilcoxon signed-rank test was used when analysing dependent samples (i.e. effect of NB-UVB treatment on CD93 expression). Hardy-Weinberg equilibrium was confirmed for the investigated genotypes using the exact test implemented in the Haploview software version 4.2 (33). SNPs were investigated for a relationship to psoriasis using a multiplicative genetic model and the likelihood-based association analysis implemented in the Unphased software version 3.1.7 (34). No multiple testing correction was conducted because of the low number of tests (2 SNPs). All statistical analysis, with exceptions stated above, was performed using Statistica 12 software (StatSoft, Tulsa, OK, USA) and SPSS statistics version 22 (IBM, New York, USA). All results given p < 0.05 were considered significant.
CD93 staining was positive in vascular endothelial cells in small and large blood vessels throughout the whole dermis of lesional skin from patients with psoriasis (Fig. 2C). In normal skin of healthy controls and in non-lesional skin from patients with psoriasis immunohistochemistry showed no epidermal or dermal staining of CD93 (Fig. 2A, B). Lymphohistiocytic perivascular infiltrate in lesional skin did not show positive CD93 staining.
Fig. 2. Increased CD93 expression in lesional skin of patients with psoriasis. Immunohistochemistry shows positive staining for CD93 in dermal endothelial cells in lesional skin of patients with psoriasis. Expression of CD93 protein (brown staining) in skin from (A) healthy controls, (B) non-lesional, and (C) lesional skin from patients with psoriasis. 20× magnification (n = 3).
CD93 gene expression was significantly increased in lesional and non-lesional skin from patients with psoriasis compared with control samples (p < 0.05) (Fig. 3). There was no significant difference in CD93 gene expression between lesional and non-lesional skin.
Fig. 3. Increased CD93 gene expression in lesional and non-lesional skin from patients with psoriasis (control n = 15, non-lesional and lesional n = 14. • mean, box=mean ± 0.95 conf. interval, whiskers=mean ± SD, *p < 0.05).
A total of 19 individuals were subject to NB-UVB treatment. The mean number of treatments was 21.63 (± 3.87) and mean PASI change (ΔPASI%) was 68.2% (± 24.9) (see Table II for treatment outcome). There was no significant difference in CD93 gene expression in lesional and non-lesional skin before and after NB-UVB treatment (Fig. S1). Post hoc analysis excluding non-responsive patients (ΔPASI% < 50) did not render significant results.
Table II. Treatment outcome after narrow-band ultraviolet B (NB-UVB) expressed in Psoriasis Area and Severity Index (PASI)
Our data revealed no significant differences in CD93 protein levels in serum or in PBMCs between psoriasis patients and controls (Figs S2 and S3).
Our results showed a significantly increased frequency of the C allele rs2749817 in patients with psoriasis compared with control subjects (p = 0.045). The CD93 polymorphism rs2749812 was not significantly associated with psoriasis (p = 0.05) (Table III).
Table III. Allele frequencies of CD93 gene polymorphisms rs2749812 and rs2749817 in patients with psoriasis (n = 218) and in healthy control subjects (n = 610)
To our knowledge, the present study is the first to show increased endothelial CD93 protein staining and significantly increased CD93 gene expression in lesional skin in patients with psoriasis compared with skin from healthy controls. The distinctive staining of CD93 in dermal endothelial cells in lesional skin, together with previously published studies on the role of CD93 (35–39) suggest that CD93 could be involved in the pathogenesis of psoriasis, either as an angiogenetic factor or as a factor promoting endothelial adhesion of inflammatory cells. Further studies are required to determine the exact role of CD93 in the pathogenic processes of psoriasis and to study the expression of CD93 within other inflammatory dermatoses to understand if the current findings are specific for psoriasis.
The present study revealed significantly increased CD93 gene expression in both lesional and non-lesional skin, while immunohistochemistry showed protein staining exclusively in lesional skin. While divergence between mRNA and protein expression is a common finding (40), the exact mechanism explaining these results is unknown. Several mechanisms, such as post-translational or post-transcriptional regulation of CD93 in the skin, may attribute to these differences. Previously it has been shown that glycosylation is important for the stabilization of CD93 expression on the cell membrane, possibly by protecting it from proteolysis (41) and Ikewaki et al. have shown that the regulation of CD93 cell surface expression is possibly controlled by protein kinase C (42). Such regulatory mechanisms may be responsible for maintenance of normal angiogenetic homeostasis in non-lesional skin preventing angiogenesis and development of psoriasis plaque or for the upregulation of CD93 cell surface expression in lesional skin. Analysing CD93 gene and protein expression in relation to an isomorphic response reaction (Koebner phenomenon) could be of interest. Increased CD93 gene expression may be a precursor for psoriasis plaque development following increased protein presence in dermal vascular endothelium and increased angiogenesis as the actual development of psoriasis plaques occur.
As to the genotype distributions of 2 CD93 SNPs investigated, we found no significant association with the allele frequencies of SNP rs2749812, a SNP in the 3´UTR region of the CD93 gene. However, we showed a significant increase in C allele frequency of SNP rs2749817 among patients with psoriasis compared with healthy control individuals. The significance of increased C allele frequency is currently not known, but rs2749817 has previously been associated with risk of breast cancer and colorectal cancer (19, 43). Rs2749817 is located downstream of the 3′ untranslated region (UTR) of the CD93 gene, which could potentially affect translation and post-translational modifications of the CD93 gene. Our observations might suggest an association of this SNPs C allele as a potential risk allele for psoriasis. It is of importance to stress that these results have to be carefully interpreted as our study population is relatively small. Larger association studies are needed to confirm our results.
UVB radiation is a well-established and highly efficacious treatment for the management of psoriasis (21–25). Increased T-cell apoptosis, induction of vitamin D and reduced epidermal and endothelial proliferation are known key factors in the anti-inflammatory effect of UVB radiation (26, 27, 44–48). In the present study, NB-UVB treatment regimen was moderately effective for our patients, with 47% reaching PASI75. Our results showed no significant effect of NB-UVB treatment on CD93 gene expression in patients with psoriasis. Immunohistochemical studies are needed in order to investigate protein presence in endothelial cells in lesional skin, since NB-UVB may have an effect on CD93 protein level not reflected in a change in gene expression. However, our results suggest that CD93 is not involved in mediating the anti-inflammatory effect of NB-UVB treatment.
It has previously been shown that CD93 is proteolytically cleaved from the surface of activated human monocytes and neutrophils in response to inflammatory signals and that a soluble form of CD93 (sCD93) exists in human blood. The presence of TNF-alpha (TNF-α) which is increased in psoriasis, has also been found to stimulate ectodomain cleavage of CD93 from monocytes (49). These data propose that inflammation triggers release of sCD93 and suggest an implication of sCD93 in inflammatory diseases (6, 36, 39, 50). However, we found no difference in sCD93 or CD93 in PBMCs levels when comparing psoriasis patients with controls. In our study population patients with mild to moderate disease were frequent (see Table I). It cannot be excluded that CD93 cleavage and elevated sCD93 levels are present in patients with severe disease. Elevated sCD93 levels have in previous studies been associated with coronary artery disease and adverse clinical outcomes in patients with acute myocardial infarction (20, 51). Since patients with severe psoriasis have an increased risk of cardiovascular morbidity and mortality further studies on sCD93 levels in patients with severe psoriasis are needed to investigate a possible correlation.
In conclusion, this is the first study showing increased CD93 expression in patients with chronic plaque psoriasis and proposing the C allele of rs2749817 as a new risk allele for psoriasis. Further studies are necessary to evaluate skin levels of CD93 protein after NB-UVB treatment and to determine the significance of the SNP association. Inhibition of CD93 is proposed as a potential anti-angiogenic target in cancer therapy, as suggested by the development and investigations on the 4E1 CD93 monoclonal antibody (26). We propose that future therapies targeting CD93 may also have a role in targeting psoriasis.
This study was supported by grants from the Swedish Psoriasis Foundation and from Futurum, The Academy of Healthcare, County Council of Jönköping, Sweden. We are grateful for the help of Siv Nilsson, Division of Dermatology, Ryhov Hospital.


 Click to show fullsize
Click to show fullsize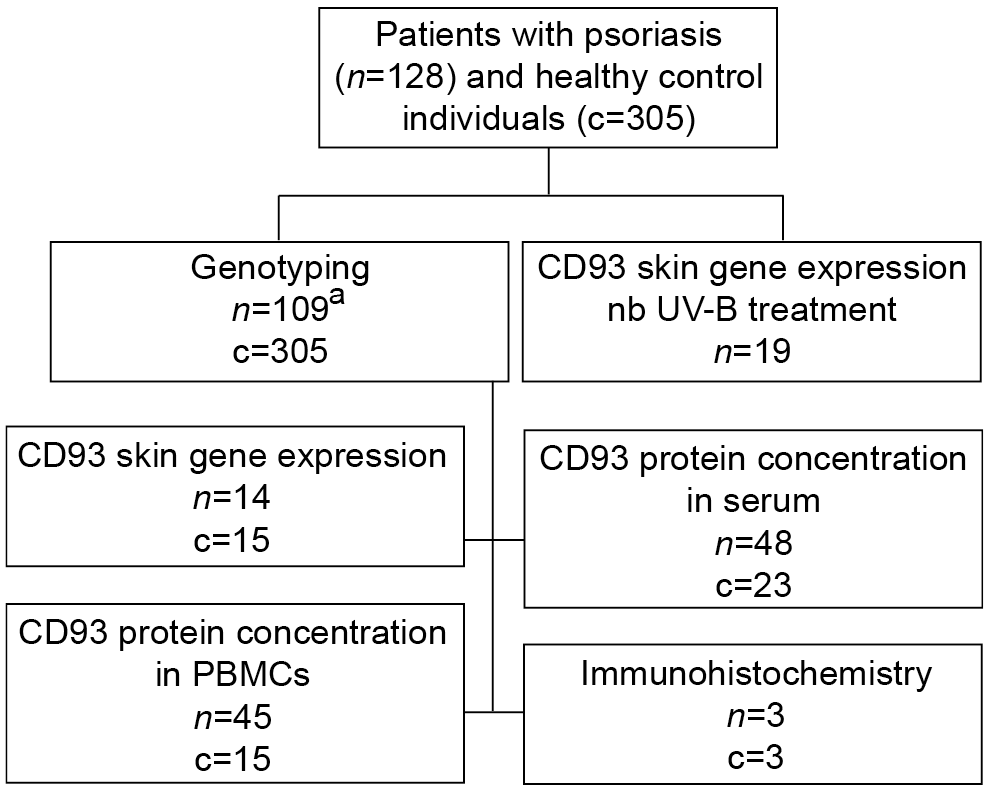 Click to show fullsize
Click to show fullsize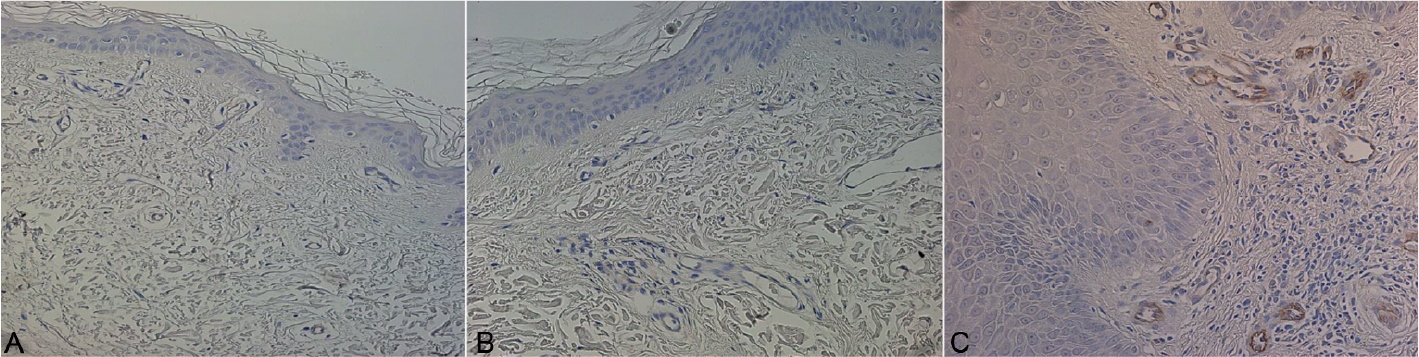 Click to show fullsize
Click to show fullsize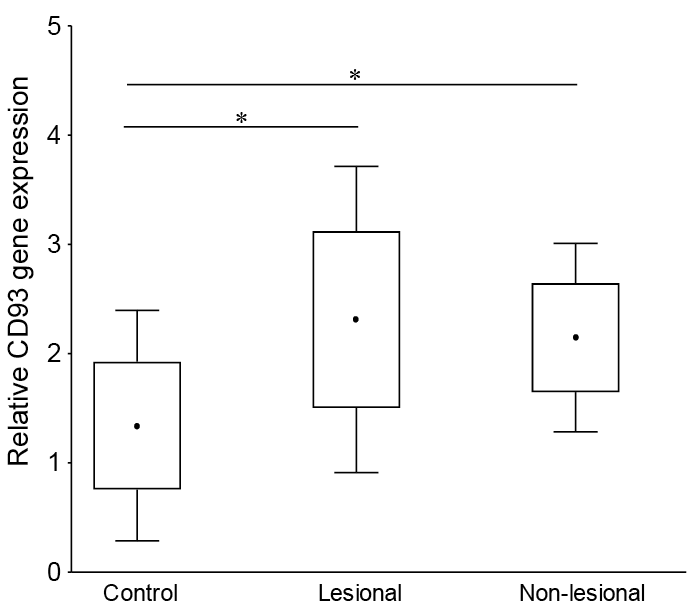 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize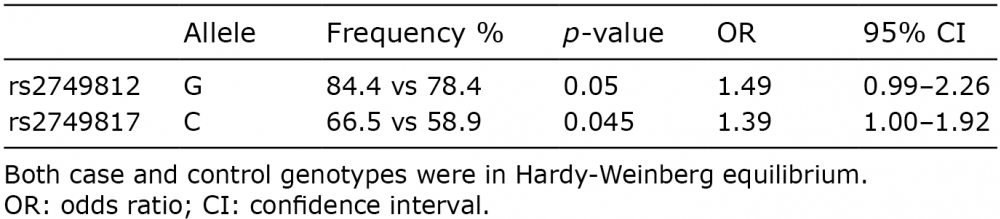 Click to show fullsize
Click to show fullsize