


Departments of 1Dermatology and Allergology, 2Medical Genetics and 4Ophtalmology, University of Szeged, Korányi fasor 6, HU-6721 Szeged, and 3MTA-SZTE Dermatological Research Group, Szeged, Hungary. *E-mail: lazarne.olah.judit@med.u-szeged.hu
#These authors contributed equally to this manuscript and should be considered as first authors.
Accepted Apr 27, 2017; Epub ahead of print Apr 27, 2017
Xeroderma pigmentosum (XP) is a potentially life-threatening disease, in which avoidance of ultraviolet light (UV) is necessary (1). In cases in which preventive measures fail, treatment of skin neoplasms is challenging and requires a multidisciplinary approach. Consecutive surgical interventions may result in devastating cutaneous defects, which determine the quality of life (QoL) of the patients. Electrochemotherapy (ECT) is a novel therapeutic option that ablates tumours with electrical current and simultaneously administered anticancer drugs (2). In various cutaneous and subcutaneous neoplasia, this method has been proven to provide long-lasting local control with minimal side-effects and good cosmetic results (3, 4).
An 11-year-old girl with XP was referred to our dermato-oncology centre with advanced non-melanoma skin cancers (NMSCs) on her face. Xerosis, skin atrophy, freckling and numerous scars from previous surgical interventions were noted on the skin surface. Unfortunately, her photoprotection in the past had been inadequate. Numerous plaques, nodules and ulcers 5–10 mm in diameter had presented, with the clinical appearance of basal cell carcinomas (BCCs). A locally advanced squamous cell carcinoma (SCC) had destroyed the surrounding tissues around the left nostril. On the left thigh, a tumour resembling keratoacanthoma (KA) 15 mm in diameter with a central keratotic plug was growing rapidly. Ophthalmological examination revealed photophobia and ectropion. Neurological examination, intelligence quotient (IQ) testing, radiological imaging and laboratory results were without significant pathological findings. Genetic investigations were performed on the genomic deoxyribonucleic acid (DNA) isolated from a peripheral blood sample from the patient. Direct sequencing of the XPC gene revealed a recurrent disease-causing homozygous nonsense mutation (c.463C/T; p.Arg155X) in the third exon (5).
Since the SCC in her central facial region could not be resected without causing a devastating defect, our multidisciplinary tumour board considered other treatment options. Although there are no published data regarding ECT in XP-C or in childhood, we decided to explore this treatment modality in our case (6). Our patient did not have risk factors for pulmonary fibrosis, which we had to consider before the administration of bleomycin. Prior to the procedure we obtained approval from the local ethics committee, the dermato-oncology and the paediatric-oncology tumour board. The patient’s parents also gave their written informed consent. ECT sessions were carried out in our department in accordance with the European Standard Operating Procedure guidelines with the Cliniporator TM device (IGEA Ltd., Modena, Italy) (7). Depending on the size and clinical feature of the tumours, different types of electrodes were chosen. In case of nodules smaller than 1.0 cm in diameter electrical pulses were delivered either using parallel arrays or, for exophytic lesions, plate electrodes. For larger nodules, hexagonal array needle electrodes were connected to the electroporation device. If required, a second run was delivered or the electrode was repositioned until complete tumour electroporation was obtained. A safety margin of 3–5 mm was treated around every nodule. Electrical parameters were as follows: for type II electrodes, 8 electric pulses of 1,000 V/cm amplitude over distance ratio and 100 ms duration, delivered at 1 or 5,000 Hz repetition frequency and, for type III electrodes, 96 electric pulses (8 pulses per pair of needles) of 1,000 V/cm amplitude over distance ratio and 100 ms duration, delivered at 5,000 Hz repetition frequency. At each session, the patient received intravenous bleomycin (15 mg/m2). Electrical pulses were delivered to the tumours during the pharmacokinetic peak (8–28 min following the administration of bleomycin). The ECT sessions were carried out under general anaesthesia, and the patient was monitored for the subsequent 24 h. During the follow-up period, dermoscopy, confocal microscopy and histology were used to detect residual tumours and new lesions. Response to treatment was assessed according to the World Health Organization (WHO) criteria at least 4 months after intervention. Sessions were repeated at 2-monthly intervals until a complete response (CR) was achieved.
The patient underwent 5 ECT sessions in one year. The mean number of treated tumours was 17 per session (11–25), the mean diameter was 0.85 cm (0.3–3.6 cm), and most of them (82%) were localized in the head and neck region. After 5 sessions of ECT, CR was achieved in 33 (97%) of the treated tumours (Fig. 1 and Fig. S1). Progressive disease (PD) was noticed in one lesion (3%), a rapidly growing KA-like lesion on the right hand, and appeared after the fourth ECT session. Following a biopsy from the lesion, our tumour board decided to refer the patient to a hand surgeon. Removal of the SCC was possible only with amputation of the fourth digit. None of the lesions showing CR relapsed during the follow-up period (4–15 months). Pain was not observed following the ECT sessions. We observed sore muscles, mild and transient erythema and oedema around the treated lesions. During the healing process, 2–3 weeks after ECT, central or complete necrosis developed in the treated tumours. Skin marks from the needle electrodes were visible for approximately one month. No systemic side-effects were observed, and the lung functional tests following the ECT sessions were normal. Due to her disease, our patient also had microstoma, ectropion and disfiguring scarring of the midface and upper lip. The patient had difficulty closing her eyelids and eating, with intubation also posing a challenge during general anaesthesia. Combined with ECT sessions, reconstructive surgeries were performed, and the function of the eyelids and lips improved significantly. Residual tumours were not detected with a histological examination of the lesions, which, clinically, had a CR.
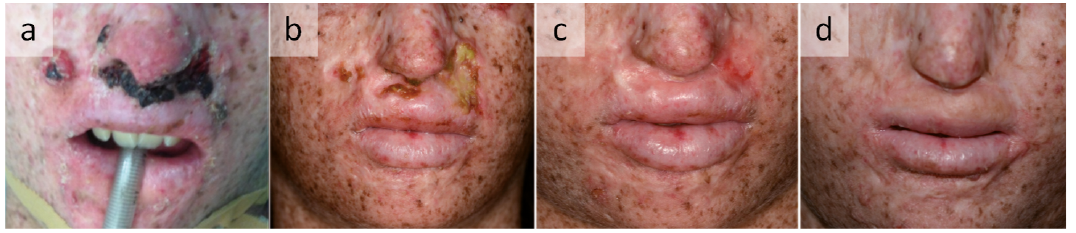
Fig. 1. (a) Squamous cell carcinoma and basal cell carcinomas before treatment, (b) 8 weeks after the first session of electrochemotherapy (ECT), (c) 2 weeks and (d) 15 months after the second session of ECT.
Based on a literature review, this is the first report of the successful use of ECT both in childhood NSMC and in XP-C.
In the XP-C group multifocal NMSCs may represent one of the main health problems and are often the major determinants of life expectancy in advanced cases.
Multiple interventions and drugs are potentially available for the treatment of NMSC, but data in the literature with regard to their use in XP are limited or conflicting. Radiotherapy (RT) can be used for patients with XP; how-ever, this is not recommended in the current guidelines and is debated in childhood (8). Surgery is the mainstay of therapy, but proper surgical management fulfilling oncological and aesthetic criteria is often difficult. Removal of the continuously arising tumours can result in disfiguring scars and devastating cutaneous defects.
ECT has proved to be safe and effective in the local tumour control of NMSCs (9, 10). The method is recommended in carefully selected patients for difficult-to-treat NMSCs, which do not respond to, or are no longer suitable for, surgery (11). CR can be achieved in most cases, with a single session of ECT. In cases with multiple tumours, the significant advantage of ECT compared with conventional surgery is, that numerous tumours can be treated at the same time and, while its effect on normal tissue is minimal, it leads to good cosmetic results.
The XPC polymorphisms (p.Lys939Gln, c.IVS11-5C>A) associated bleomycin-induced chromosomal aberrations signify clinically important risk for patients with XP-C (12). Based on the sequencing results, our patient carries the wild-type genotypes (TT and CC) of the p.Lys939Gln and c.IVS11-5C>A polymorphisms, therefore the repeated administration of bleomycin may not cause chromosomal aberrations, although long-term follow-up is necessary.
Based on the available evidence and on our experience with Gorlin–Goltz syndrome (13), we explore here the use of ECT for the numerous NMSCs in an 11-year-old child with XP-C. ECT provided good local control of the locally advanced, unresectable SCC on her face and of the multiple BCCs with preservation of organ function and an acceptable aesthetic result. There was no post-procedure pain after ECT, i.e. consistent with a previous report (14). Since numerous lesions can be treated during a single ECT session, the psychological burden of multiple surgeries can be reduced, which is especially important in childhood.
This work was supported by the János Bolyai Research Scholarship of the Hungarian Academy of Sciences and GINOP 2.3.2-15-2016-00020 grant.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize