


1Department of Dermatology – STD Centre, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, IT-20122 Milan, and 2Department of Dermatology, University of Milan, Milan, Italy. E-mail: m.cusini@policlinico.mi.it
A 24-year-old circumcised man presented with an ulcerative lesion on the penis which had been present for 3 days. He reported that the lesion had appeared after sexual intercourse with his girlfriend. He had been circumcised in childhood for religious reasons. Clinical examination revealed an ulcerative and crusted posthitis with multiple ulcers, penile oedema and bilateral inguinal lymphadenopathy (Fig. 1). The patient reported having fever and malaise. Cutaneous swabs for herpes simplex virus types 1 and 2, Treponema pallidum and Chlamydia trachomatis PCR were negative, whereas cutaneous swab for bacterial culture detected Streptococcus pyogenes and Staphylococcus aureus. Serological tests for syphilis, HIV and hepatitis C virus were negative. Systemic therapy with ceftriaxone, 1 g i.m. for 5 days, was prescribed, which resulted in improvement in the ulcerative lesions and general symptoms, but hard penile oedema was still present.
Fig. 1. Ulcerative and crusted posthitis with multiple ulcers and penile oedema.
The patient denied any aberrant sexual activity or other sexual practices, even upon further questioning. The personal history of the otherwise healthy patient was inconspicuous.
A biopsy from the thick portion on the penis was performed.
What is your diagnosis? See next page for answer.
Histological examination revealed dense presence of empty optical gaps, corresponding to an exogenous substance, surrounded by foamy histiocytes granulomas in the deep dermis and in the subcutaneous fat tissue (Fig. 2). The histology was compatible with “siliconoma”.
Fig. 2. Hematoxylin and eosin staining, 4x magnification. Empty optical gaps in the mid and deep dermis, surrounded by granulomas.
During the third control visit following another interview, the patient reported that he had undergone silicone injections 2 years previously. The procedure was performed in the Philippines with the support of the patient’s father.
Although penis girth enlargement, using permanent fillers, may, in general, yield good results in the short term, the possible severe complications in the longer term, such as migration of silicone, granulation, and infection, cannot be ignored. Silicone and other permanent fillers are also used elsewhere in the body for cosmetic purposes and for medical indications (e.g. lipoatrophy based on highly active antiretroviral therapy or atrophic facial deformities as a result of Romberg’s disease) with the same type of complications (1).
Complications resulting from enlargement of the penis by applications of unknown types of silicone and mineral oils are well described (2).
Injections of permanent fillers into the penis introduce additional risks that are inherent to the anatomy of the penis. The skin of the penis is thin, and subcutaneous fat is lacking, so the injected material has little protection. In addition, the penis has a great deal of mobility between the skin layer and the underlying corpora, so that the penis can vary in size. Sexual intercourse causes many small traumas at the location of the deformed filler deposits, so the risk of infection is high (1, 3).
In our patient sexual intercourse with his girlfriend probably caused the breakup of a silicone deposit and consequently ulcerative lesions with bacterial superinfection.
In conclusion, injections with permanent filling substances should be taken into consideration in the differential diagnosis of ulcers of the penis.


 Click to show fullsize
Click to show fullsize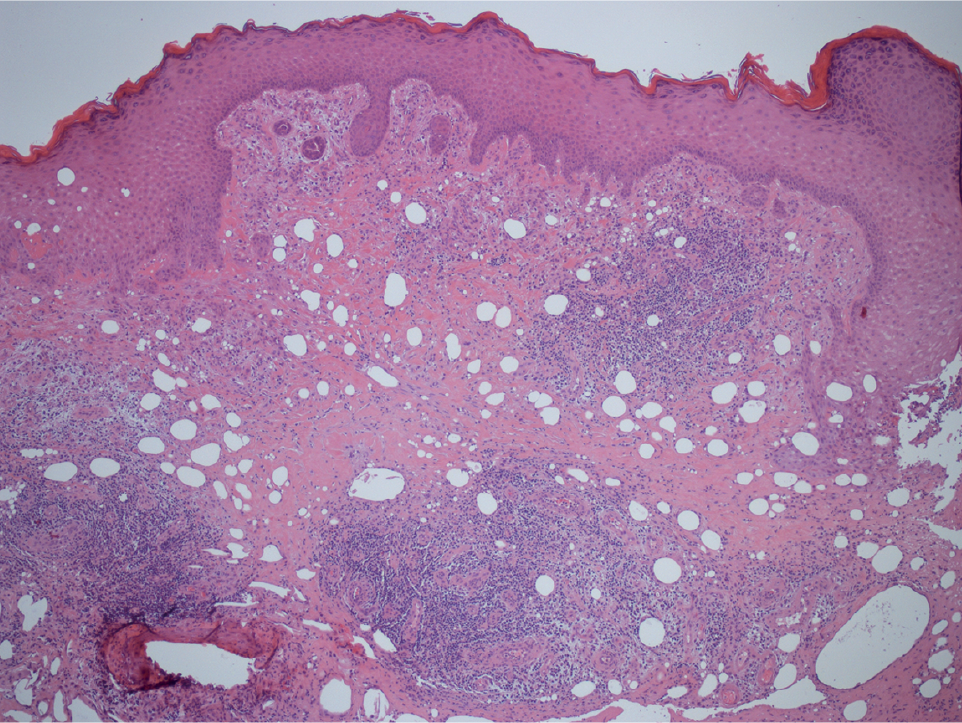 Click to show fullsize
Click to show fullsize