


1Department of Dermatology, No. 1 Hospital of China Medical University, 155 North Nanjing Street, Shenyang 110001, and 2Liaoning Centre for Prenatal Diagnosis, Department of Gynecology & Obstetrics, Shengjing Hospital of China Medical University, Shenyang, China. *E-mail: hongduochen@hotmail.com, liyuanhong@vip.sina.com
#These authors contributed equally to this paper.
Accepted May 10, 2017; Epub ahead of print May 12, 2017
Hypohidrotic ectodermal dysplasia (HED) is one of approximately 200 different genetic conditions of ectodermal dysplasia (ED) identified by the lack, or dysgenesis of, at least 2 ectodermal derivatives, such as hair, nails, teeth and sweat glands (1, 2). The hereditary model in most cases is X-linked (XLHED) caused by mutations localized in the gene encoding ectodysplasin-A (EDA) (1, 3, 4). Less commonly, HED caused by mutations localized in the ectodysplasin-A receptor (EDAR) or ectodysplasin-A receptor-associated adapter protein (EDARADD) gene with an autosomal dominant or autosomal recessive pattern of inheritance. XLHED (OMIM: 305100) is characterized by a triad of signs of hypohidrosis, hypotrichosis and hypodontia. This study enrolled a single Chinese family with XLHED with the rare phenotype of remarkable hyperplasia of the sebaceous glands and performed next-generation sequencing (NGS) to scan for potential mutations.
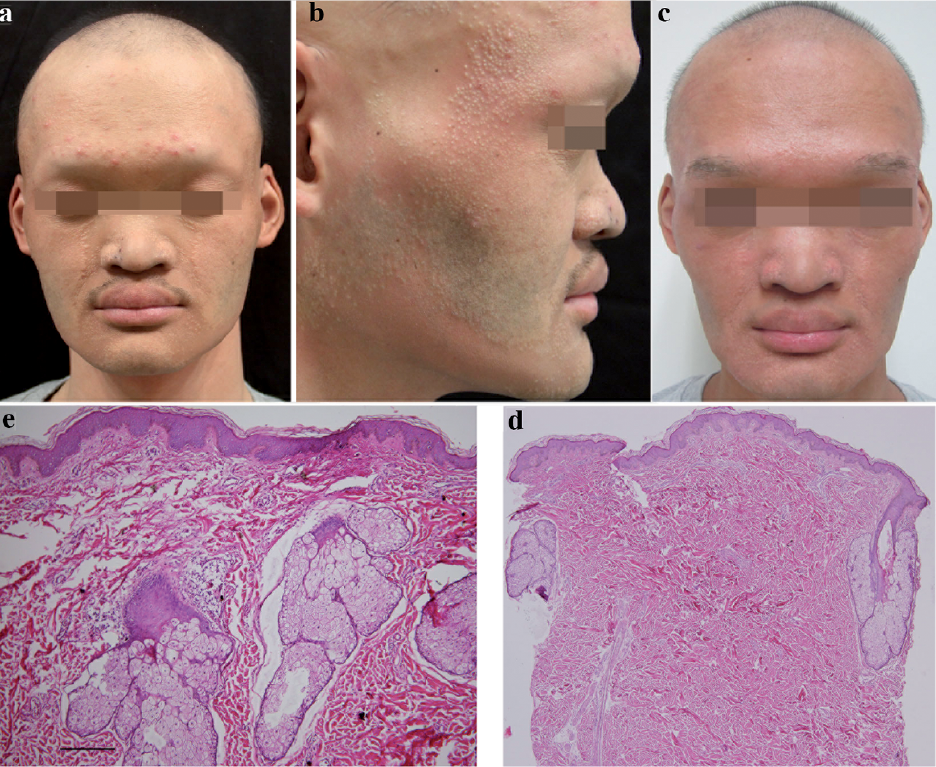
A Chinese pedigree of HED was collected. The proband was a 27-year-old male who reported absence of sweating, dry thin lustreless sparse hair over the scalp, absence of eyelashes, axillary, pubic and whole-body hair, and congenitally missing teeth (Fig. 1a,b). He also reported intolerance to heat. In particular, the patient had hundreds of solid, whitish yellow, milia-like papules distributed symmetrically over his whole face in confluent plaques, which had been present since puberty (Fig. 1b). A vellus hair was present in the centre of each papule. The patient had a prominent forehead and a saddle nose. The oral mucosa, nails and palmoplantar surfaces were roughly normal, except for dry skin. Histological findings from the scalp included the absence of anagen hair follicles and sweat glands (Fig. 1d). Biopsy of the papules on the face showed many large sebaceous gland lobules surrounding vellus hair follicles and the absence of sweat glands (Fig. 1e).
Fig. 1. (a) Clinical appearance of the proband. (b) Numerous papules in confluent plaques symmetrically distributed on his face. (c) Notable improvement after treatment with fractional CO2 laser. (d) Skin biopsy of the scalp revealed a complete loss of sweat glands (haematoxylin and eosin (HE) ×100). (e) Histological presentations of a skin biopsy from his face showed many large sebaceous gland lobules (HE×100). Written permission was given by the patient to publish these photographs.
NGS was performed as reported. Written informed consent was obtained from all subjects and approval for the study was provided by the Institutional Review Board and the ethics committee of No. 1 Hospital of China Medical University. Genomic DNA from the proband’s peripheral blood was random fragmented, and the targeted exon sequences plus ?anking sequences (all exons extending 100 bps on each side of an exon) of EDA, EDAR and EDARADD genes were specifically captured and enriched using an array-based hybridization chip (NimbleGen, Madison, WI, USA). Sequencing was performed on the HiSeq2500 (Illumina, San Diego, CA, USA) sequencer using 90-bps paired-end chemistry according to standard operating protocols. Single nucleotide polymorphisms (SNPs) and indels were identified using the SOAPsnp and GATK Indel Genotyper, respectively.
The mean of the targeted area of EDA, EDAR and EDARADD was 155.43×. A mean of 95.3% of base pairs with > 30× coverage were successfully detected. Six variants were detected. The frequency of the deletion variant (EDA: EX6 DEL) was 0 in SNPs database and it was predicted as candidate mutation (Fig. S1a). The other 5 variants (EDAR c.1109T>C, EDAR c.1056C>T, EDAR c.750C>T, EDARADD c.27G>A, EDARADD c.60G>A) were identi?ed as SNPs with a frequency of 0.022~0.869 in the 1000 Genome Project database.
To confirm the EDA: EX6 DEL variant, primers were designed according to EDA sequence (NM_001399) (forward primer 5’- GTAGTCAGTAACATCCCAAGA and reverse primer 5’- TGCTCAGGACAGCCAGTAG). We also recruited 200 unrelated healthy Chinese individuals of different ages with no family history of XLHED as controls. Genomic DNA of all family members and 200 normal controls was ampli?ed by PCR. GAPDH was also amplified as internal control (forward primer 5’- AGAAGGCTGGGGCTCATTTG and reverse primer 5’- AGGGGCCATCCACAGTCTTC). Electrophoresis of PCR products showed that there was one band of exon 6 of EDA and one band of GAPDH in the lanes of the proband’s parents and normal controls; however, there was no band of exon 6 of EDA in the proband’s lane (Fig. S1b). To detect the copy number of EDA, real-time PCR was performed with genomic DNA under standard conditions. Each sample was measured with 3 separate tubes and repeated 3 times. Real-time PCR showed that the proband’s mother and father carried 1 copy of EDA exon 6, but the proband carried 0 copies of EDA exon 6 (Fig. S1c). A carrier status was identified for the proband’s mother (Fig. 1f). This HED family was determined as XLHED. The proximal or distal breakpoints of the deletion were not identified, which might be due to the breakpoints being located in the intron areas.
The exon 6 deletion of EDA resulted in the deletion of 248–265 amino acid residues and frame shifting mutation of the following EDA amino acid residues. The new reading frame stopped early, with only 14 amino acid residues (IFQVECSMTGLASL) (Fig. S1d). The tumour necrosis factor (TNF) domain of EDA (248–388 amino acids) is the EDAR binding site. This mutation (EDA c.742-793del, p.P248_D265del, I248fsX261) should affect the interactions of EDA with its receptor EDAR.
The proband’s face was treated with fractional CO2 laser (ActiveFXTM microscanner handpiece, Ultrapulse Encore, Lumenis Ltd, San Jose, CA, USA). The parameters were set as followed: pulse energy 90 mJ, density 5, pulse size 10×10 mm, and repetition rate 300 Hz. The patient received 3 treatments at an interval of 6 months with remarkable improvement (Fig. 1c). He also received eyebrow transplantation with hair follicles collected from his beard (Fig. 1c). The patient was satisfied with the improvement.
The inheritance pattern of this pedigree and identification of EDA mutation were in accordance with XLHED. In general, patients with HED presented with a reduction in the number of sweat glands, hair follicles and sebaceous glands, which was responsible for the dry skin. However, this proband presented with remarkable hyperplasia of the sebaceous glands, which has rarely been reported (5–7). Dry skin was noted on the patient’s face, which indicated dysfunction of the hypertrophic sebaceous glands. It has been assumed that hyperplasia of the sebaceous glands might due to early ageing or hormonal influences. However, the significance of this particular feature remains unexplained.
EDA signalling is crucial for the morphogenesis of ectodermal appendages (8). The EDA/EDAR/EDARADD signalling pathway functions by stimulating NF-κB-mediated transcription of effectors or inhibitors of the Wnt, Sonic Hedgehog, fibroblast growth factor and transforming growth factor beta pathways (5). EDA is a 391 amino acid residue membrane protein with a C-terminal TNF homology domain for receptor binding (8). More than 200 EDA mutations have been reported (4, 9). However, there is no specific genotype–phenotype correlation in patients with HED. The TNF domain of EDA is also the EDAR binding site, so the mutation in our pedigree (EDA c.742-793del, p.P248_D265del, I248fsX261) should affect the interactions of EDA with its receptor EDAR, disturb the subsequent signalling pathway and cause the phenotypes of XLHED.
Treatment of XLHED is difficult. Sgontzou et al. (5) reported a case of XLHED treated with salicylic acid peels for the hyperplastic sebaceous glands. Our proband received eyebrow transplantation, wore dentures, and accepted fractional laser treatments for hyperplastic sebaceous glands with notable aesthetic improvement. Current optimal treatment requires multidisciplinary collaboration. Recombinant EDA or gene therapy may bring new hope to these patients in the future (1).
This work was supported by the Program for the National Science Grant (code: 81602740).
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize