


1Department of Specialized, Clinical and Experimental Medicine, Division of Dermatology, University of Bologna, Via Massarenti 1, IT-40138 Bologna, 2Dermatology Unit, Department of Clinical and Molecular Sciences, United Hospital of Ancona, Polytechnic Marche University, Ancona, 3Clinica Dermatologica, Policlinico Di Bari, Bari, 4Department of Dermatology, University of Rome La Sapienza-Polo Pontino, Rome, 5Dermatology Unit, Arcispedale Santa Maria Nuova IRCCS, Reggio Emilia, and 6U.O. Dermatologia, Fondazione IRCCS Ca’ Granda – Ospedale Maggiore Policlinico, Milan, Italy. *E-mail: michela.magnano@gmail.com
Accepted May 16, 2017; Epub ahead of print May 17, 2017
In HIV-infected patients psoriasis is often severe (1) and biologic therapy may therefore be needed. However, most dermatologists are cautious when using immuno-suppressive agents in patients with HIV, as these agents may reactivate or induce infection in already immunocompromised patients (1). To date, only a few cases of HIV-infected psoriatic patients treated with biologics have been reported (2). We report here 10 cases of HIV patients treated for plaque psoriasis with biologic therapies in 6 psoriasis centres in Italy.
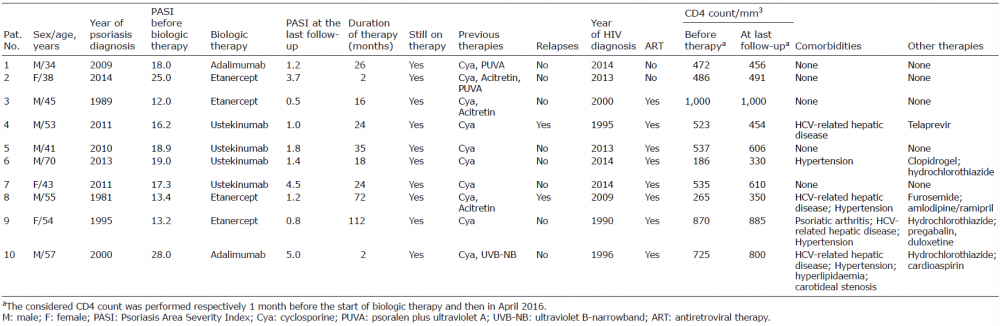
Ten HIV-infected patients were included in this study, mean age 49 years, who had had moderate-to-severe plaque psoriasis for at least 2 years (mean Psoriasis Area Severity Index (PASI) 18.1) (Table I).
Table I. Patients’ characteristics including features of psoriasis and HIV
All of the subjects had received a diagnosis of HIV at least 2 years before the diagnosis of psoriasis and 4 patients also had concomitant hepatitis C virus (HCV) infection. All of the patients had been treated intermittently for at least one year with cyclosporine, which had to be discontinued to avoid side-effects (3), while 4 also failed to respond to phototherapy or acitretin. We therefore decided to start biologic therapy in these patients.
Patients had had a stable viral load for at least 12 months, a stable CD4 count for at least 12 months and showed no signs of infection. CD4 count was monitored monthly. In patients with concomitant HCV infection, their viral load and liver enzymes were checked every 2 months, and a hepatic ultrasound was performed every 6 months.
In 4 patients ustekinumab was started at a dose of 45 mg then 45 mg after 4 weeks and then every 12 weeks, while in the other 6 patients an anti-tumour necrosis factor (anti-TNF) agent was administered at the standard dose. Four patients were treated with etanercept and 2 with adalimumab (adalimumab was administered at a dose of 80 mg at time zero, then 40 mg after a week followed by 40 mg every 2 weeks, while etanercept was started at a dose of 50 mg twice weekly for the first 12 weeks than 50 mg weekly). The choice of the biologic was made according to the lifestyle of each patient.
The mean duration of therapy was 34.8 months. None of the patients developed adverse effects, including infectious complications, or had to interrupt the treatment. All patients are still on biologic therapy. All patients reached 75% of clearance of the lesions (PASI75) after 3 months. However, relapses were observed after 10 and 13 months in 2 patients treated with ustekinumab and these were managed by adding phototherapy.
The totality of patients showed overall stable or slightly decreased levels of CD4, which subsequently resolved without changing the antiretroviral therapy (ART). This is in accordance with other reports (2) in which significant fluctuations in CD4 count were not observed.
Although the relationship between HCV reactivation and the use of biologic therapies is still debated (4), 4 of our subjects also had a concomitant HCV infection. Two were treated with etanercept, one with adalimumab, and one with ustekinumab, without experiencing adverse effects. The HCV viral load and liver enzymes remained at low levels throughout the whole duration of the therapy, and the hepatic ultrasound, performed every 6 months, did not show any substantial changes.
Since psoriasis is often difficult to treat in HIV-infected patients, the use of biologic therapies may be unavoid-able. Given the paucity of literature, it is not easy to determine when it is appropriate to start a biologic therapy, which particular therapy to choose, and how to follow up the patient. In addition, the best biologic agent for patients with HIV is unclear. Most case reports describe the use of an anti-TNF agent, mainly because dermatologists are likely to have had more experience with the use of such agents, but also because TNF-alpha seems to have a role in viral replication and the pathogenesis of HIV, improving HIV symptoms and sequelae (2).
Two case reports on the use of ustekinumab in psoriatic HIV-infected patients have been published so far (1, 4) with good results. However, interleukins (IL)-12 and IL-23, targets of ustekinumab, seem to have a positive involvement in the control of opportunistic infections, inflammation and tumourigenesis associated with HIV infection (5), whereas high levels of TNF-alpha, the target of adalimumab and etanercept, are related to viral replication and progression of the disease (6).
For the reason given above, although there are more cases of infectious complications in HIV-infected patients treated with anti-TNF agents than ustekinumab, probably due to their longer use, it may be reasonable to first choose an anti-TNF agent to avoid possible long-term infectious complications in HIV-infected patients and then, if these are not effective or are contraindicated, switch to an interleukin (IL)-12/23 inhibitor.
This is the largest case series reported so far of HIV-infected patients treated with biologics, with one of the longest follow-ups. Although the number of cases is still limited, we believe that the use of biologic agents may be considered a possible effective choice in psoriatic patients with a stable HIV infection. It is also mandatory to monitor CD4 count and HIV viral load, in order to avoid possible causes of infections.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize