


Department of Dermatology, CHA University College of Medicine, Bundang CHA Medical Center, Yatap-ro 59, Bundang-gu, Seongnam 13496, Korea. *E-mail: terios92@cha.ac.kr
Accepted May 16, 2017; Epub ahead of print May 17, 2017
Atopic dermatitis (AD) is strongly associated with skin barrier dysfunction, as indicated by a reduction in skin hydration and an increase in transepidermal water loss (TEWL) (1). Long-term use of topical corticosteroids poses a risk of developing adverse cutaneous effects, including skin atrophy and rebound flares. Topical calcineurin inhibitors, tacrolimus and pimecrolimus, were found to be as effective as moderately potent topical corticosteroids (2). However, the main obstacle to use of topical tacrolimus is its local side-effect, a burning sensation, which sometimes leads to discontinuation of treatment (3). Although the mechanism of the burning sensation after topical application of tacrolimus is thought to be associated with damaged skin barrier function, there has been no study to assess the association between TEWL and burning sensation following topical application of tacrolimus. This study evaluated the correlation between burning sensation following topical tacrolimus and skin barrier function in AD.
This prospective study was performed in accordance with the ethics guidelines of the Declaration of Helsinki 1975 and approved by the institutional review board of Bundang CHA Medical Center, CHA University, Seongnam, Korea from April 2011 to April 2015. All patients agreed to participate voluntarily and gave written informed consent. Patients aged ≥16 years with moderate to severe AD meeting the diagnostic criteria of Hanifin & Rajka, confirmed by the same dermatologists, were enrolled in the study. All patients were using topical tacrolimus ointment for the first time and had facial lesions. Patients were excluded from the study if they had any of the following conditions at the time of study entry: other concomitant dermatological disorders besides AD on the site to be treated; known hypersensitivity to macrolides or other ointments; tumour or a history of a tumour or systemic disease including HIV and chronic disease states where the patient is unstable or uncontrolled; pregnant or lactating women. There was a 1–4-week wash-out period for previous AD therapies before the trial: 4 weeks for systemic corticosteroid or other immunosuppressive drugs and one week for topical corticosteroids, topical antibiotics or other topical immunomodulators.
To assess the skin barrier function of patients with AD, TEWL was measured using a Vapometer® (Delfin Technologies Ltd, Kuopio, Finland) on the cheeks of patients with AD. Skin hydration was assessed with a Corneometer® (Courage & Khazaka electronic GmbH, Köln, Germany) in the same areas as for TEWL. Three repeated measures were taken using each tool, and the mean value was calculated. A thin coat of 0.1% tacrolimus ointment (Protopic; Astellas Pharma Korea Inc., Seoul, Korea) applied twice daily on the facial atopic lesion. At 2 weeks after the first visit, the occurrence of burning sensation was questioned. The definition of “burning sensation” in this study was a feeling of warmth or heat, including events such as pain, stinging and soreness at the application site (3).
Student’s t-test was used to compare the 2 groups of patients with/without burning sensation. The mean and standard deviation (SD) of the TEWL and skin hydration of the groups with or without a burning sensation after application of tacrolimus ointment were calculated and compared. SPSS (version 24.0, SPSS Inc. Chicago, IL, USA) was used to analyse the data and p-values < 0.05 were considered significant.
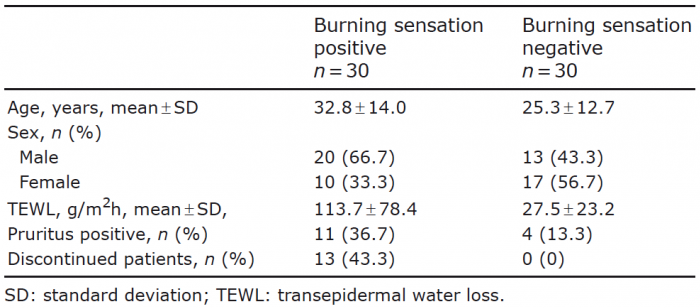
A total of 60 patients (age range 16–62 years, mean age 29.1 years) completed the study (Table I). Among them, 30 patients (50%) experienced a burning sensation. TEWL levels were statistically significantly higher in patients with a burning sensation than in those without (113.7 ± 78.4 g/m2h vs. 27.5 ± 23.2 g/m2h, p < 0.001). Skin hydration showed no statistically significant difference between patients with and without a burning sensation (51.8 ± 18.6 g/m2h vs. 53.6 ± 15.6 g/m2h, p = 0.673). Of the patients with a burning sensation, 11 had pruritus associated with tacrolimus, and 4 patients without a burning sensation had pruritus. Among 30 patients with a burning sensation, 13 (21.7%) discontinued the use of topical tacrolimus, 17 gradually became tolerant to topical tacrolimus without discontinuation (Table I). There was no statistically significant difference between patients who discontinued ointment and those who did not (122.8 ± 78.5 g/m2h and 106.7 ± 80 g/m2h, p = 0.586). In the event of intolerable burning sensation, patients were recommended to apply topical tacrolimus ointment mixed with any commercially available moisturizers in a 1:1 ratio. Most of the discontinued patients (12 of 13 patients) tolerated topical tacrolimus ointment when mixed with moisturizer.
Table I. Patients’ characteristics
In this study TEWL was statistically significantly higher in patients with a burning sensation after the application of tacrolimus ointment than in those without a burning sensation. Elevated TEWL can predict burning sensation after the application of tacrolimus ointment.
The main advantage of topical tacrolimus is the provision of proactive therapy (4). More recently, Chittock et al. (5) showed that proactive use of topical tacrolimus promotes reparation of the subclinical barrier defect in AD. Topical tacrolimus does not cause skin atrophy and can be used safely on the more vulnerable regions of the skin, such as the face and neck (6). Long-term safety of topical tacrolimus has been confirmed (7).
However, the adverse effects of topical tacrolimus are transient application-site reactions, such as burning or pruritus. These side-effects lead to treatment discontinuation in 1.6–5.3% of patients with AD (3). In the present study, 21.7% of patients discontinued the use of tacrolimus ointment due to the burning sensation. Approximately 16–59% of patients experienced a burning sensation and approximately 9–46% of patients reported pruritus in other clinical studies (3, 8). The burning sensation after application of tacrolimus ointment lasts for approximately 15–20 min, for the first few days of treatment. In general, the burning sensation, pruritus and erythema resolve within one week of initiating topical tacrolimus and occur more frequently in adults than in children. These complications are related to disease severity. Such events decrease rapidly as AD lesions heal with improving skin barrier and skin hydration (3, 8, 9).
The mechanism of the burning sensation following topical tacrolimus is not fully understood. Tacrolimus is known to activate dorsal root neurones in rodents and to induce neuropeptide release and mast cell degranulation in murine skin (10). The key molecule of cutaneous nerve activation is the non-selective cation channel, transient receptor potential vanilloid 1 (TRPV1).
The application of tacrolimus could stimulate sensory neurones and increase the phosphorylation of TRPV1 channels, which leads to the release of inflammatory neuropeptides, including substance P and calcitonin gene-related peptide. As a consequence, this may promote cutaneous neurogenic inflammation locally around nerve endings, transient burning or painful sensations (11, 12). With a disrupted skin barrier function, more tacrolimus molecules can be absorbed, and side-effects, such as burning or pruritus of the AD lesions, would occur.
Steroid-free over-the-counter moisturizers may counteract TEWL caused by a defective skin barrier. Controlled clinical trials have demonstrated that moisturizers improve the symptoms of AD, particularly pruritus, erythema, fissuring and lichenification (13). In the current study, most of the discontinued patients could tolerate topical tacrolimus mixed with moisturizer. Previously, Al-Khenaizan (14) suggested that pre-cooling of topical tacrolimus ointment reduced the burning sensation. This is another good method to mitigate the burning sensation, but cooling the tube for a prolonged time might cause the medication to become inspissated and difficult to extract.
In conclusion, increased TEWL can be a predictor of topical tacrolimus-associated burning sensation. Use of a moisturizer and a gradual increase in dose of topical tacrolimus are recommended for the prevention of the burning sensation.
This study was supported by grants from Astellas Pharma Korea, funding sources: BD2010-111 (Astellas Pharma Korea).


 Click to show fullsize
Click to show fullsize