


1Department of Dermatology, Venereology and Allergology, University Hospital Wuerzburg, Josef-Schneider-Straße 2, DE-97080 Wuerzburg, 2Department of Dermatology, University Hospital Munich and Municipal Hospital of Munich, Munich, 3Department of Internal Medicine, Early Clinical Trial Unit, University Hospital Wuerzburg, and 4Institute of Pathology, Comprehensive Cancer Center Mainfranken, University of Wuerzburg, Wuerzburg, Germany. E-mail: Behle_V@ukw.de
Accepted May 16, 2017; Epub ahead of print May 17, 2017
Despite recent advances in basic and translational research in the field of cutaneous lymphomas (1, 2), effective treatment options for advanced mycosis fungoides (MF) and Sézary syndrome (SS) are limited. Conventional therapies usually result only in short-lived remission (3), lacking any long-term advantage of more aggressive chemotherapeutic regimens (4) and having septic complications. A recent retrospective meta-analysis found that immunological treatment approaches, such as interferon or extracorporeal photopheresis, as well as epigenetic modifiers, produce better rates of disease control in patients with MF and SS than does immuno-suppressive chemotherapy (5). Hence, better immunomodulating drugs addressing the tumour microenvironment of cutaneous lymphomas (6) as well as novel targeted therapies and innovative combinational approaches (7) are urgently required (8).
We report here a patient with SS and nodal CD30-positive manifestation who was treated with a combination of extracorporeal photopheresis (ECP) and the drug-conjugated anti-CD30 antibody brentuximab vedotin.
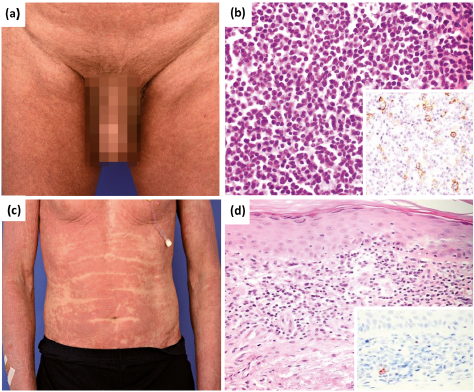
The 77-year-old man was diagnosed with SS in February 2011. Due to extensive erythroderma and blood manifestation (elevated lactate dehydrogenase > 500 U/l and a CD4/CD8 ratio > 100 with antigen loss of CD7 and CD26), lymph node and bone marrow involvement (stage IVA2 of the ISCL/EORTC classification), he underwent multiple systemic treatments. At first, the patient was treated with methotrexate, 15 mg/week, which was changed to bexarotene, gemcitabine and chlorambucil/prednisolone after only short-lived remissions and subsequent therapeutic failure, respectively. Rapid progression of skin lesions led us to apply total skin electron beam radiation therapy, but without success, so that 3 months later a dual LSD1-(lysine-specific demethylase)/HDAC- (histone deacetylase) inhibitor-inhibitor was started within a phase I study. Owing to further disease progression, treatment was changed after another 3 months to liposomal doxorubicin, under which the patient encountered multiple complications including bullous palmoplantar erythrodysaesthesia and serious bacterial infections. Finally, 46 months after the first diagnosis and after having undergone 6 prior and, in the long run, unsuccessful, systemic treatment modalities, chosen according to international standards, the patient presented with acute thrombosis on the left iliac vein due to compression by rapidly progressive inguinal and pelvic lymph nodes. Clinical examination and computed tomography (CT) scan revealed multiple enlarged lymph nodes (Fig. 1a). As biopsy of an enlarged lymph node showed nodal CD30-positive lymphoma infiltration (Fig. 1b), we decided to initiate treatment with brentuximab vedotin within an off-label setting after obtaining the patient’s consent. At this time-point, blood and skin manifestations showed partial expression of CD30 in 5–10% of lymphoma cells before initiation of brentuximab vedotin. Rapid partial remission of nodal disease, decline in blood tumour burden and initial amelioration of cutaneous manifestations was achieved under this treatment regimen. However, after 4 months of treat-ment, progressive pruritic papular infiltration of the skin with worsened erythroderma again developed (Fig. 1c). Of note, blood and skin manifestations were now repetitively negative for CD30 (Fig. 1d) despite continued tracking of the identical T-cell clone in respective compartments. This finding led us to choose an add-on treatment with ECP.
Fig. 1. Clinical and histologic features. (a) Progressive enlarged ilioinguinal lymph nodes are present before treatment start with brentuximab vedotin. (b) Histology of an excised inguinal lymph node shows diffuse infiltration of T-cell lymphoma with large cell transformation (haematoxylin and eosin (HE) ×200). Expression of CD30 in at least 10% of lymphoma cells is present within the lymph node (CD30 staining ×200) (insert). (c) Progressive skin disease with infiltrated, papular erythroderma was present 4 months after initiation of brentuximab vedotin (5 cycles). (d) Histology of skin shows an epidermotropic atypical T-cell infiltrate of medium-sized cerebriform lymphoma cells with indented nuclei (HE × 200). Neoplastic T cells of the skin are negative for CD30 (CD30 staining × 200) (insert).
Over a period of 8 consecutive months the patient received combination therapy with intravenous brentuximab vedotin, 1.8 mg/m2, every 3 weeks and ECP on 2 consecutive days every 4–6 weeks. Lymph nodes returned to almost normal size and the cutaneous tumour burden improved significantly after the addition of ECP with almost resolution of confluent erythroderma and novel, steadily enlarging “nappes claires” corresponding to clinically uninvolved skin (Fig. S1a, b). Moreover, since the start of treatment with brentuximab vedotin the lactate dehydrogenase levels returned to 300–400 U/l, albeit exhibiting an undulating course without strict correlation with clinical response and the CD4/CD8 ratio in peripheral blood declined significantly from pre-therapeutic levels of 195 vs. lowest levels of 45, the latter especially after the addition of ECP to the therapeutic regimen (Fig. S1c). Undulating and minor paraesthetic sensations in the legs were managed successfully by intermittent increase in dose intervals of brentuximab vedotin to 4 weeks, as initial neuropathy could not be excluded with certainty; otherwise, the patient did not experience any serious (> grade 2) complications like neutropaenia, sensorimotor neuropathy or infections under this treatment and presented with a good quality of life. However, 16 months after the start of brentuximab vedotin and 8 months after initiation of combination therapy, ECP was discontinued due to repetitive failure to achieve sufficient vascular access and further refusal by the patient. After discontinuation of this combined treatment, blood and skin manifestations were rapidly progressive and refractory to next-line treatment with bendamustine and the patient died 9 months after discontinuation of brentuximab vedotin/ECP treatment.
A better understanding and more detailed characterization of the immunophenotypic and molecular genetic features of systemic lymphomas has paved the way for the development of more specific and better tolerated anti-neoplastic drugs (2, 7). In this respect, the common expression of CD30 in Hodgkin’s lymphoma, as well as in systemic anaplastic large-cell lymphoma, can be targeted by immunotherapeutic approaches. This has led to the approval of the drug-conjugated anti-CD30 antibody brentuximab vedotin-monomethyl auristatin E for treatment of relapsed or refractory disease condition in European countries (9). Beside primary cutaneous CD30-positive lymphoproliferative disorders, expression of CD30 may also be observed in advanced MF and, rarely, in SS, especially within the context of large cell transformation (10). However, CD30-positive cells in MF and SS are usually present to a more variable and, altogether lower, extent and are often not universally found in all affected disease compartments, such as skin, blood, lymph nodes or viscera. Nevertheless, several case reports for SS (11–13) and a recent phase II clinical study evaluating brentuximab vedotin in MF and SS have demonstrated high efficacy (14), and a phase III trial is in progress (ALCANZA trial; https://ash.confex.com/ash/2016/webprogram/Paper91517.html). Of note, the response was rather irrespective of the level of CD30 expression in lymphoma tissue, hinting at possible additional bystander-effects of the drug within the tumour microenvironment (15). Based on these promising clinical data, we treated our patient with brentuximab vedotin in an off-label setting. Owing to prior, life-threatening infectious complications in our patient, and a putative risk of neutropaenia under brentuximab vedotin, an add-on therapy with non-immunosuppressive ECP was chosen for CD30-negative non-responsive manifestations. Several topical or systemic combination modalities have been evaluated in conjunction with ECP, with additional therapeutic success (16). However, to date, there are no reports on such a multimodal approach combining ECP with brentuximab vedotin for SS and, altogether, only a few patients with SS have been reported to be treated successfully with brentuximab vedotin monotherapy.
Therefore, our approach is new, in combining the rather unspecific immunomodulating treatment effects of ECP with a compartment-directed targeted therapy and thus exploiting super-additive therapeutic effects with distinct kinetics, producing both rapid and long-term response.
Disclosures: MW is on the Advisory Board TAKEDA.


 Click to show fullsize
Click to show fullsize