


1Oaro Dermatology Clinic, Seoul, 2Department of Dermatology, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Korea
An optimized therapeutic regimen involving a non-ablative fractionated laser or radiofrequency therapy for acne scars has not yet been established. To evaluate whether the combination of a non-ablative fractional laser (NAF) and fractional micro-needling radiofrequency (FMR) has clinical advantages for the treatment of atrophic acne scars compared with NAF alone, a 16-week prospective, randomized split-face study was performed. Each facial side of a patient was treated with 3 sessions of either NAF with FMR or NAF alone, with a 4-week interval between each session. Although both sides demonstrated significant decreases in the échelle d’évaluation clinique des cicatrices d’acné (ECCA) score, the facial side treated using the combination regimen demonstrated greater improvement in ECCA score regarding degree and onset time than the NAF-treated side. Histopathological and immunohistochemical results confirmed the clinical findings. This study demonstrated that a combination regimen involving NAF and FMR could be a viable option with satisfactory efficacy.
Key words: acne scar; fractional photothermolysis; laser surgery; radiofrequency.
Accepted May 16, 2017; Epub ahead of print May 17, 2017
Acta Derm Venereol 2017; 97:
Corr: Gyeong-Hun Park, MD, PhD, Department of Dermatology, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, 7, Keunjaebong-gil, Hwaseong-si, Gyeonggi-do 18450, Republic of Korea. E-mail: borelalgebra@gmail.com and Jae Yoon Jung, MD, MS, Oaro Dermatology Clinic, 507, Nohaero, Nowongu, Seoul 01695, Republic of Korea. E-mail: jaeyoon007@hanmail.net
Facial atrophic acne scarring, a permanent sequelae of acne vulgaris, may be a socially disabling and psychologically devastating disease (1, 2). Among a multitude of treatment options, recent application of various devices based on ‘fractional photothermolysis (FP) technology’ has brought remarkable advances and broadened therapeutic options (3, 4). However, there are still no guidelines regarding the selection of fractional devices from the perspective of maximum efficacy and minimal downtime. Although ablative FP may be more efficacious in fewer treatments, patients tend to experience more downtime and a higher risk of various side effects including pain, pigmentation, scarring, and prolonged healing, especially in patients with darker skin (5, 6).
In that sense, non-ablative fractional lasers (NAF) or radiofrequency (RF) devices have been actively applied to minimize treatment-related adverse effects (7). NAF such as a 1,550-nm erbium-glass fractional laser has been proven to deliver effective improvements to scarred skin with low complication rates (8, 9). It results in shorter downtime than ablative lasers, and re-epithelialization is complete within one day (8). Fractional micro-needling radiofrequency (FMR) delivers bipolar RF directly to the dermis using an array of microneedles (10). FMR has been recently reported to improve skin laxity, wrinkles, and acne scarring (11, 12). Given its association with epidermal preservation and a rapid recovery time, it has become popular recently.
Despite the advantages of non-ablative fractional devices, previous studies have rarely evaluated whether combination treatments involving these devices have advantageous effects from the perspective of efficacy and potential side effects for the treatment of acne scarring. In this study, we aimed to evaluate whether the sequential application of NAF and FMR has a synergistic effect on the efficacy and safety of atrophic acne scar treatments, as compared with conventional NAF alone during 3 consecutive sessions through a prospective, randomized split-face comparison study.
This study was conducted based on a 16-week, prospective, randomized split-face protocol that compared clinical and histological aspects between two facial sides either receiving sequential application of NAF and FMR or NAF alone for atrophic acne scar. It was carried out in accordance with the Declaration of Helsinki and approved by the Institutional Review Board. Informed consents were acquired from all subjects prior to enrollment. Treatments of each side were scheduled to receive 3 consecutive sessions at 4-week intervals, with a follow-up visit 8 weeks after the final third treatment. Twenty-eight Korean subjects (15 men and 13 women, aged 21–38 years, 15 Fitzpatrick skin type III and 13 type IV) with atrophic and/or hypertrophic acne scars were enrolled. Participants whose échelle d’évaluation clinique des cicatrices d’acné (ECCA) score was higher than 50 were eligible for inclusion (13). A simple random allocation sequence was created using computer-based random number generators to assign the treatment modality of each side. Randomization codes were secured in a safe until all data analyses were finished. Two dermatologists evaluating the scar improvement were blinded to the assignment. Patients were excluded from the study if they had active acne under treatment, or if they had received any other treatments for acne scars for 3 months prior to the first treatment. None of the patients underwent other treatments including chemical, mechanical or laser resurfacing during the study period. At patients’ each visit, photo-graphic assessments by dermatologists, and patients’ subjective assessments were performed. Skin biopsies were also conducted at both baseline and post-treatment evaluation.
According to the randomly assigned allocation, one half of the face was treated with both FMR device (Secret™, Ilooda, Suwon, Republic of Korea) and 1,550 nm erbium-glass fractional laser (Fraxel SR 1500, Reliant Technologies Inc., Mountain View, CA, USA) and the other half was treated with 1,550 nm erbium-glass fractional laser only. As microneedling can induce minor bleeding which can impede the subsequent procedure, the erbium-glass fractional laser was performed firstly in the combination treatment. Prior to the treatment, patient’s entire face was completely cleansed with a skin cleanser, and then an anesthetic ointment containing 4% lidocaine was applied to the face for 30 min. The treatment settings were as follows; 1.5- to 2.5-mm microneedle penetrating depth, 20 to 50 intensity, and 50- to 100-ms duration with 2-3 passes in FMR device and 25 to 35 J/cm2 at level 6 with 4 passes in 1,550 nm erbium-glass fractional laser.
Standardized digital photograph was taken at every visit using same camera settings (EOS 600D, Canon, Tokyo, Japan) and tangential lighting at fixed positions. Efficacy of scar improvement was assessed by investigator’s global assessment (IGA) and ECCA scores. IGA was evaluated using a 5-point scale associated with the degree of improvement (grade 0 = no improvement, 1 = 1–25% improvement, 2 = 26–50% improvement, 3 = 51–75% improvement, 4 = 76–100% improvement). Moreover, acne scar was categorized and evaluated by specific subtypes (icepick, boxcar, and rolling scar). Two dermatologists who were not involved in treatments rated the IGA and ECCA scores based on the photographs taken at baseline and every follow-up visit. Patients’ subjective assessments of satisfaction score and mean duration of downtime were also surveyed. The subjective satisfaction score was evaluated using a 5-point scale (0 = no improvement, 1 = slight improvement, 2 = moderate improvement, 3 = good improvement, 4 = excellent improvement). Subjects also recorded the durations of post-treatment changes including erythema, edema, and dryness. The related side effects and changes (hyperpigmentation or hypopigmentation, acne eruption, secondary scarring, and infection) were documented during treatment sessions in detail. The overall duration of subjective downtime was also recorded from each patient.
Skin biopsies were performed from atrophic scars on the cheeks with a 2-mm punch from 6 patients. Tissues acquired at typical atrophic scar lesions of the cheek areas at the baseline and final visit were stained with both Hematoxylin & eosin (H&E), and Masson’s trichrome (MT). To investigate molecular changes after treatments, the samples were processed for immunohistochemical (IHC) staining for collagen-1, collagen-3, and transforming growth factor (TGF)-β1 (Abcam, Cambridge, UK). The relative intensity of staining of samples was assessed by an image analysis program (Leica QWin version 3.5.1, Leica Microsystems, Wetzlar, Germany).
The paired t-test or Wilcoxon signed-rank test and the McNemar test were used to compare the differences between before and after treatment and those between combination and NAF treatment sides (SPSS version 19.0, SPSS Inc., Chicago, IL, USA). A p-value < 0.05 was considered as statistically significant.
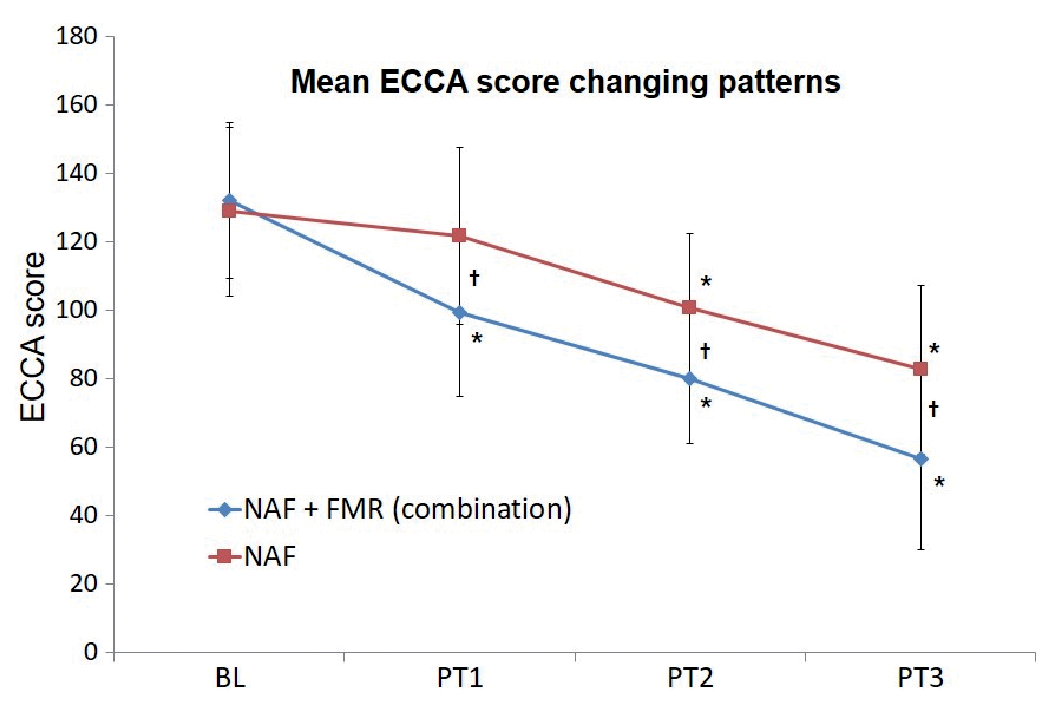
Of the 28 patients who were initially enrolled, 26 (14 men and 12 women, aged 21–38 years; 13 Fitzpatrick skin type III and 13 type IV) patients completed the study; two patients withdrew for personal reasons. No patient withdrew secondary to treatment-related adverse events. There was no significant difference in mean ECCA score at baseline between one facial side and the other (Fig. 1).
Fig. 1. Mean ECCA score changing pattern of each side evaluated from baseline to the final observation after 3rd treatment session. *p < 0.05 compared with baseline, †p < 0.05 compared between two sides. BL: baseline, PT: post-treatment. ECCA: échelle d’évaluation clinique des cicatrices d’acné; NAF: non-ablative fractional laser; FMR: fractional micro-needling radiofrequency.
While both sides demonstrated significant improvement in ECCA score 8 weeks after the third session of each treatment, facial sides treated with the combination regimen demonstrated superior efficacy regarding degree and onset time, as compared with the NAF side. Specifically, the ECCA score was significantly decreased at the final visit compared with baseline at both sides (combination: 131.9 ± 22.6 ƒ 56.3 ± 26.7, p < 0.01; NAF: 128.7 ± 24.6 ƒ 82.5 ± 24.7, p < 0.01), corresponding to a reduction of 57.3% and 38.9%, respectively (Fig. 1). The difference between the two regimens was significant regarding mean ECCA score at the final visit (p < 0.01), and differences had been evident since 4 weeks after the first treatment session. A meaningful reduction in the ECCA score compared with baseline was achieved 4 weeks after the first session in the combination regimen side and 4 weeks after the second session in the NAF side. The IGA score results were consistent with the ECCA score results. Twenty of the 26 facial sides treated with the combination regimen improved more than 2 grades on the IGA score, but only 11 of the NAF-treated sides did. Distribution patterns for the two regimens were different (p < 0.05) (Fig. 2). Representative figures of each facial side after treatment are shown in Fig. 3 and Fig. S1.
Fig. 2. Evaluation of scar improvement based on investigator’s global assessment at the final visit. NAF: non-ablative fractional laser. Combination: NAF+micro-needling radiofrequency.
Fig. 3. Clinical photographs revealed the improvement of acne scars by both therapeutic modalities. (A, B) combination regimen-treated side of the face. (C, D) non-ablative fractional laser (NAF)-treated side of the face. (A, C) Before treatment. (B, D) Eight weeks after 3 sessions of treatment. Though some improvement was observed in NAF-treated side, a more prominent improvement in acne scars was noted on the combination regimen-treated side of the face.
Then, subgroup analyses were performed using ECCA scores. A reduction in ECCA score was analyzed according to the type of atrophic acne scar. U-shaped atrophic scars (boxcar scars) demonstrated significant reductions on both sides, and the reductions became evident after the first treatment. V-shaped atrophic scars (ice-pick scars) achieved the smallest reduction on both sides, with a significant reduction demonstrated after the second treatment only on the side treated with the combination regimen. M-shaped atrophic scars (rolling scars) achieved a significant reduction after the first treatment on the combined treatment side and after the second treatment on the NAF side (Table I).
Table I. ECCA after consecutive treatments for 3 major subtypes of ECCA grading scale (V, U and M)
In addition, the degree of percent improvement on each side was compared based on the baseline scar severity levels. For both therapeutic regimens, the degree of improvement was noticeable in those with moderate to high baseline severity (ECCA ≥ 130), as compared with those with mild baseline severity (ECCA < 130). Furthermore, from a direct comparison of both regimens, the combination regimen was superior to the NAF regimen only in those patients with moderate to high baseline severity (p < 0.05) (Table II).
Table II. Degrees of improvement measured by mean percent change in the ECCA score in two groups designated by baseline scar severity
Patient self-assessments of the degree of improvement paralleled the physicians’ evaluations. Patients’ mean scores evaluated at the final visit were 3.0 ± 0.8 on the combination treatment side and 2.1 ± 0.6 on the NAF treat-ment side. The proportion of patients whose subjective self-ratings indicated ‘excellent improvement’ or ‘good improvement’ was 76.9% (20/26) on the combined treatment side and 34.6% (9/26) on the NAF side (Fig. 4).
Fig. 4. Evaluation of scar improvement based on patients’ subjective satisfaction at the final visit. NAF: non-ablative fractional laser.
Various treatment-related side effects were thoroughly compared between the two sides of each patient. For treatment-related side effects including erythema, edema, and dryness, there was no significant difference in the severity or duration between the two sides. No difference was observed in long-term side effects including pigmentary changes, acne eruption, and secondary scar formation. As for the patients’ subjective assessment regarding the meaningful impact the treatment had on their quality of life, the average duration of downtime was 2.6 ± 1.1 days for the combination treatment side and 2.3 ± 1.3 days for the NAF only side, which showed no significant difference.
A comparative investigation of histological changes induced by each treatment was performed. In H&E and MT, both treatment regimens demonstrated increased collagen fiber deposition at the final visit, as compared with baseline, but denser dermal interstitial fiber accumulation was induced on the side treated with the combined regimen. IHC staining for type I and III collagen further supported the above-mentioned findings. The intensity of TGF-β1 staining was also increased after successive treatments on both sides, but was much higher on the combination side (Fig. S2).
Patients undergoing acne scar treatment are usually concerned with subsequent side effects or posttreatment recovery time as well as efficacy. In this context, non-ablative fractionated devices based on laser or RF technology have opened new horizons from the perspective of safety and minimal downtime. However, an optimized therapeutic regimen has not yet been established. This study demonstrated that the combination of NAF and FMR has synergistic efficacies with no accumulated downtime for acne scar treatment, suggesting that this novel regimen may help overcome a major weakness of non-ablative procedures involving their relatively limited efficacy, as compared with ablative ones (5).
Our combination regimen demonstrated greater efficacy and faster onset of action in improving acne scars, as compared with NAF alone based on both subjective satisfaction and objective evaluations. Synergistic effects were relatively more significant in moderate to severe degrees of acne scarring, as compared with mild degrees, suggesting that this regimen could replace ablative lasers for this indication. In addition, the co-application of other chemical or physical treatments including dot peeling or subcision with this combination regimen may be helpful for the treatment of V-shaped scars (14). As for safety issues, the incidence of commonly observed, treatment-related side effects was not notably increased, as compared with NAF alone. FMR leads to only slight changes in epidermal barrier functions, resulting in shorter downtime (15). Severe side effects including secondary scarring and pigmentary changes were not observed in the current study. Furthermore, the mean downtime was not different between the two sides.
An analysis of therapeutic mechanisms involving these two devices would help elucidate these synergistic effects. Each of them acts in a different way to improve acne scars. The 1,550-nm erbium-doped fractional laser induces thermally coagulated microscopic columns of dermal tissue in regularly spaced arrays over a fraction of the skin surface, leading to the upregulation of new collagen production with no ablative effect on the epidermis (16). Leaving intact tissue bridges between minute cores of coagulation necrosis within the dermis results in faster healing, as healing originates not only from the skin adnexa but also from these skin bridges. However, it seems that many sessions of treatment must be delivered to achieve a satisfactory level of clinical improvement (5, 17).
However, FMR delivers bipolar RF directly to the dermis with minimal epidermal damage owing to finely designed microneedles. RF can induce electric current, which results in dermal heating. While lasers generate heat by delivering energy to chromophores through selective photothermolysis, the heat produced by the RF device originates from electron movement and conductivity of the target tissue (18, 19). As RF is originally not ablative, it rarely results in a transient interruption of epidermal integrity that is usually seen in ablative lasers (20, 21). In addition, microneedles have been reported to stimulate the migration and proliferation of keratinocytes and fibroblasts by inducing the release of several growth factors (22, 23). With these completely different action mechanisms, FMR seems to deliver high volumetric heating and deeper heat diffusion for profound neoelastogenesis and neocollagenesis, consolidating the effects of dermal remodeling if combining microthermal treatment zones with NAF (22).
Our histological analysis in support of these mechanistic insights demonstrated that the combination regimen induces greater increases in the extent and thickness of interstitial fibers throughout the whole dermis, as compared with NAF alone. The expression levels of both collagen fibers were also significantly higher on the combination side. The greater expression of TGF-β1 would be responsible for the accumulation and thickening of interstitial fibers in the dermis. TGF-β1 plays important roles in optimal wound healing during the early phase of laser or RF treatment, leading to the stimulation of fibroblasts in a dose-dependent manner (24, 25). These findings strongly suggest that the superior reproduction of dermal fibers at a histological level would explain the clinical benefits of the combination regimen.
There were some limitations in this study. First, all enrolled patients had a similar ethnic background. Second, additional studies would be needed to determine the most efficacious treatment parameters including energy level, depth of needling, the number of passes or treatment sessions, and interval between treatments. Finally, this study did not measure the efficacy of FMR alone for acne scars. However, a previous study reported that NAF is more effective for acne scars than FMR (15). Because our present study showed that the combination of NAF and FMR is superior to NAF alone, we can speculate that the combined treatment would also be more effective than FMR alone.
In conclusion, combined use of NAF and FMR demonstrated definitive synergistic effects compared with NAF for acne scars, with reasonable safety profiles. Therefore, a few sessions of this combination regimen could be a viable option with satisfactory efficacy, especially for Asian patients more frequently concerned with posttreatment side effects or downtime.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize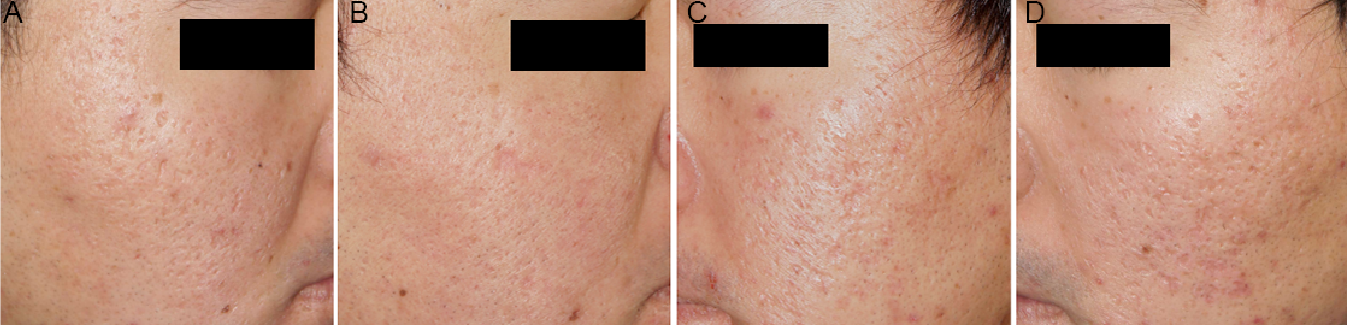 Click to show fullsize
Click to show fullsize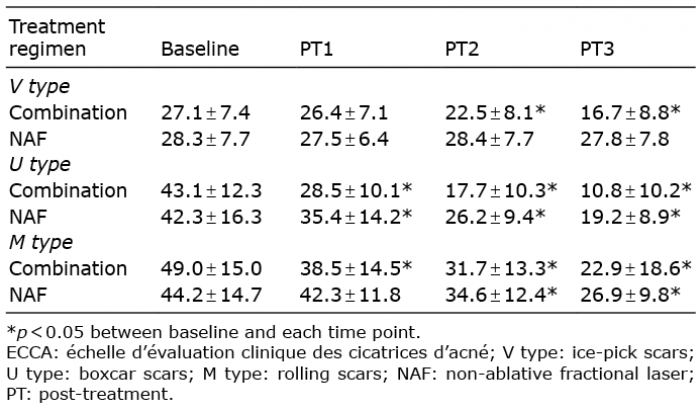 Click to show fullsize
Click to show fullsize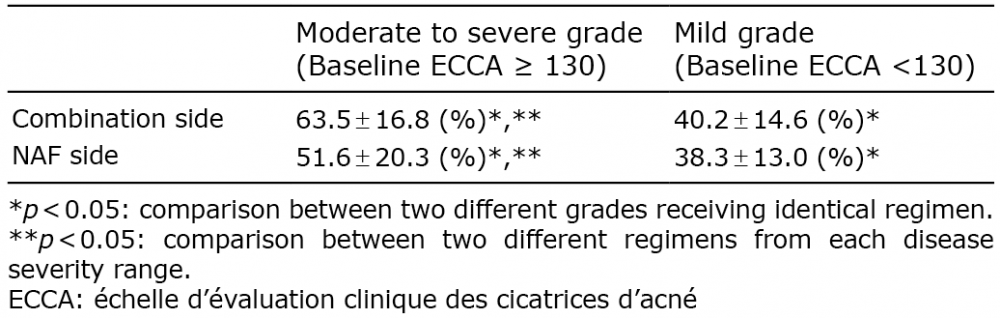 Click to show fullsize
Click to show fullsize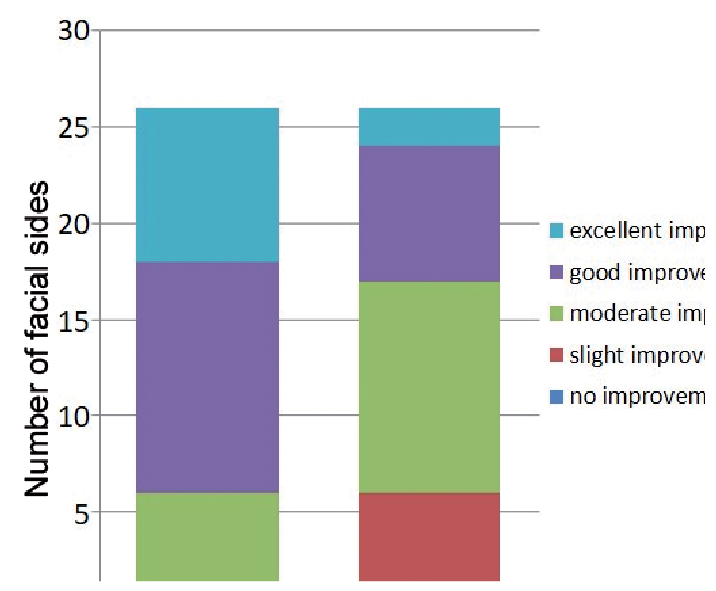 Click to show fullsize
Click to show fullsize