


1Department of Psychiatry, 2Department of Dermatology, Oslo University Hospital, Rikshospitalet, and 3R&D of Mental Health, Akershus University Hospital, Loerenskog, Norway
There is increasing evidence of clinically relevant anti-inflammatory effects of monoaminergic antidepressants. PubMed and Ovid databases were searched systematically for the use and efficacy of antidepressants in association with 5 common inflammatory skin disorders: chronic urticaria, psoriasis, atopic dermatitis, other eczema, and alopecia areata. From January 1984 to June 2016, publications included a total of 1,252 dermatological patients in 28 trials or case reports. These unambiguously reported a reduced burden of dermatological symptoms in relation to treatment with antidepressants. Several randomized controlled trials of first-generation antidepressants have been published, while studies of modern antidepressants are usually open-label, yet more informative, regarding patients’ characteristics and study procedures. These overall positive findings may indicate a rationale, beyond treating comorbid psychiatric disorders, for the use of antidepressants in dermatology. Further research into modern tolerable antidepressants, including selective serotonin re-uptake inhibitors, mirtazapine and bupropion, is required.
Key words: systematic review; antidepressant; dermatological disorder; anti-depressive; anti-inflammatory.
Accepted May 16, 2017; Epub ahead of print May 17, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Shirin Eskeland, Department of Psychiatry, Oslo University Hospital, Rikshospitalet, NO-0196 Oslo, Norway. E-mail: shiesk@ous-hf.no
Antidepressants are a class of psychotropic drugs acknowledged for their antidepressive effects, which are used primarily in the treatment of depression and anxiety disorders. Anti-inflammatory or immune-modulatory effects of antidepressants have been described in rodent models of several chronic disorders, including skin contact allergy and hypersensitivity, rheumatoid arthritis, inflammatory bowel disease and multiple sclerosis (1–4). A growing body of evidence also points to immune-modulatory properties of antidepressants in humans (5). Treatment with antidepressants in depressed patients with various chronic inflammatory disorders has been linked to improvement in somatic symptoms, with a reduction in complications and the use of steroids or other medical interventions (6–10).
It is acknowledged that, to varying degrees, inflammatory skin disorders have a systemic inflammatory component (11–15). In mice, the infusion of bacterial lipopolysaccharides results in systemic inflammation, neuro-inflammation and depression-like symptoms, sometimes referred to as “sickness behaviour” (16). An equivalent in humans is the administration of interferon-α for viral hepatitis, promoting systemic inflammation and, not infrequently, depression (17, 18). Depression and anxiety are prevalent in people with common inflammatory skin disorders, e.g. chronic urticaria (CU) and psoriasis (19, 20). Therefore, in theory, inflammatory disorders of the skin, especially when accompanied by systemic inflammation, may affect the central nervous system (CNS) and adversely influence mood (21).
Inflammation is increasingly acknowledged to play a role in the pathophysiology of depression (Fig. 1). The anti-inflammatory actions of antidepressants may be relevant to their anti-depressive effects (22, Fig. 1). In both mice and humans there is compelling evidence that selective serotonin reuptake inhibitors (SSRIs) attenuate inflammatory processes, as mentioned above, also relieving the “sickness behaviour” resembling depression and anxiety symptoms (23, 24). The attenuation of inflammation in animal studies, in vitro human cell lines and patient case reports has been found to involve the modulation of cytokine levels, with a decrease in tumour necrosis factor (TNF)-α and/or an increase in interleukin (IL)-10 levels (24–28).
Fig. 1. Antidepressants counteract inflammation and hypothalamic-pituitary-adrenal (HPA) axis activation. The figure depicts the potential target points for antidepressants in a sequence of stress-induced inflammatory and neuroendocrine events. Stress, psychological or physical, increases the release of interleukin (IL)-1 and tumour necrosis factor (TNF)-α through adrenoreceptor activation of leukocytes (78). The subsequently increased secretion and circulation of pro-inflammatory substances may trigger inflammatory pathways in the brain and, possibly also, in peripheral tissues (58, 79–82). The enzyme indoleamine 2,3 dioxygenase (IDO) is activated by pro-inflammatory substances and catabolizes tryptophan into neurotoxic metabolites tryptophan catabolites along the IDO pathway (“TRYCATs”). Meanwhile, the supply of tryptophan, essential in the formation of serotonin, may be compromised (81). Antidepressants prevent or attenuate the end-points by impeding the activation of the HPA-axis (the cortisol response) and reducing the release of pro-inflammatory substances from immune cells upon stress (83, 84). CRF: corticotrophin-releasing factor/hormone.
To avoid confusion with non-medical (e.g. herbal) anti-depressive remedies, antidepressant drugs are sometimes referred to as monoaminergic antidepressants due to their effects on the body’s monoamine levels. First-generation antidepressants, the tricyclic antidepressants (TCA), have a history as a second-line or adjuvant treatment for CU and pruritus of various origins (29–31). Mirtazapine, a second-generation noradrenergic antidepressant, is thought to have the same benefits, while avoiding the cardiotoxicity seen with TCAs (32). For dermatological disorders the relevance of TCAs and mirtazapine has primarily been viewed in relation to their anti-histamine properties (33). However, most second-generation or newer antidepressants have minimal histamine H1- and H2-blocking effects, but nevertheless, portray anti-pruritus properties (34–36).
The aim of this study is to investigate the anti-inflammatory potential of antidepressants. Specific questions examined are: (i) Is treatment with an antidepressant useful in inflammatory dermatological disorders? (ii) How may treatment with antidepressants affect the skin? (iii) Are there reasons to consider treatment with antidepressants for dermatological disorders regardless of psychiatric comorbidity?
This study is a literature review of the use of antidepressants in 5 common inflammatory skin disorders primarily regarded as non-psychogenic in origin. PubMed, Web of Science and Ovid databases (MEDLINE, Embase, PsycINFO, AMED and Ovid Books) were searched from January 1984 to 26 June 2016 for the use of antidepressants in CU/urticaria, plaque psoriasis/psoriasis, atopic dermatitis/eczema (AD), other eczema/dermatitis and alopecia areata (AA). CU refers to both the older term chronic idiopathic and the newer term chronic spontaneous urticaria. When referring to the inducible types of CU, this will always be stated clearly.
Use of antidepressants was studied both in the context of comorbid anxiety or depression, and as a supplement to other traditional and established dermatological treatments for the skin disorders under review. The skin disorders that are the focus of this review are commonly regarded as inflammatory and are accompanied by inflammation of the skin. We remind the reader that although there is no objective inflammation in alopecic hair-less patches; hair loss in AA stems from inflammatory processes at the level of the hair follicle.
We did not investigate the use of antidepressants in primary psycho-cutaneous disorders or pruritus, since inflammation is not an essential feature of such conditions. The review includes any route of administration of an antidepressant, which was oral, or, in the case of the TCA doxepin for eczema, topical. Any mode of drug administration is regarded as relevant since we are interested in locally mediated as well as systemically mediated effects.
The largest studies of first-generation antidepressants in dermatology were performed in the late 1980s. For practical reasons, since older research papers were difficult to access and review comprehensively, we restricted our search to start from January 1984. The literature review was primarily performed by searching for any publication on trials, case reports and reviews with the following word combinations either in the title or abstract “antidepressants agent/drug AND (psoriasis OR urticaria OR eczema OR dermatitis OR alopecia areata)”. The titles, abstracts and, sometimes also, the full article were read to establish if the publication was eligible for the review. Supplementary searches were performed for different classes of antidepressants in combination with any of the researched skin disorders in PubMed. A few relevant publications were found through other eligible papers.
The structured database search of PubMed and the Ovid databases yielded a total of 478 hits. Searching Web of Science did not provide any further relevant hits. Twenty-nine papers complying with selection criteria were primarily retrieved from the structured searches. A few papers, less than a handful, were retrieved from other supplementary searches. Eligible papers reported treatment or co-treatment with antidepressants in plaque psoriasis/psoriasis, CU/urticaria, atopic dermatitis/eczema, other eczema/dermatitis and AA. The review also includes an epidemiological cohort study of SSRI use in patients with psoriasis. The results are shown in Table I.
Table I. Studies of antidepressants in 5 common dermatological disorders
The TCA doxepin has been investigated in the treatment of CU, with the total of nearly 100 patients enrolled in 4 controlled and blinded trials (37). Maximum response was reached within a few days to a few weeks in CU, and even in hours in the case of the inducible urticaria. Dosages of 5 and 25 mg doxepin, 2–3 times daily, have proven equal or superior to the first-generation anti-histamines mequitazine (5 mg bid) and diphenhydramine (25 mg tid), respectively, in the treatment of CU (29, 38). In the study by Greene et al. (29) 50 patients with CU received either doxepin 10 mg tid or diphenhydramine 25 mg tid for 14 days, followed by a placebo washout of 3 days and then 14 days of doxepin/diphenhydramine in randomized sequence with a double-blinded cross-over. Therapeutic response was assessed by patient symptom diary scores of daily itching and frequency, number, size and duration of hives on a 4-point scale (1–4). Total clearing of hives was reported in 43% of the patients receiving doxepin compared with 5% of patients on diphenhydramine (p > 0.001). While doxepin induced markedly less sedation (22%) than diphenhydramine (46%) (p < 0.05), complaints of dry mouth were more common with doxepin (42%) than diphenhydramine (16%) (p > 0.05).
As far as we know no comparisons of a second- or third-generation antihistamine with an antidepressant for CU have been performed. Modern antihistamines are not necessarily more efficient in the treatment of CU than older types, but are usually preferred due to markedly less sedation and anticholinergic side-effects. Antihistamines when used optimally, which may require recommended daily dosages taken several times per day, provide satisfactory control of symptoms in a mean of 50–60% of CU cases, although the results are poorer for inducible types of CU (39, 40). It is therefore interesting that a controlled study found that 8 out of 9 patients with inducible cold urticaria preferred doxepin 10 mg tid over hydroxyzine 10 mg tid, even though doxepin was not significantly better than hydroxyzine at suppressing and shortening the wheal response in a standardized ice cube test (41).
To our knowledge, there are no studies of newer antidepressants for CU of either idiopathic/spontaneous or inducible types and evidence is limited to 8 case reports from 5 publications (42–46). Bigata et al. (42) reported remission from severe CU after 7 days of treatment with mirtazapine. There was a relapse within one week of discontinuation of mirtazapine; however, there was an excellent response on reintroduction of the drug. CU in conjunction with panic disorder has been reported by Gupta & Gupta (43) to respond to sertraline in one case and to fluoxetine in another case, effects lasting throughout the treatment period of 12 and 18 months, respectively.
Two controlled double-blind trials of monoamine oxidase inhibitors (MAOIs) have reported significantly better improvement in Psoriasis Area Severity Index (PASI) scores on treatment with MAOIs compared with placebo (47, 48). In the study by Di Prima & De Pasquale (48) tranylcypromine 5 mg od was given in monotherapy to 13 patients with moderate to severe psoriasis. The patients received 8 weeks of active agent and 8 weeks of placebo in a double-blinded cross-over design. Alpsoy et al. (47), on the other hand, investigated a strategy of augmenting standard topical corticosteroids with the MAOI moclobemide (300 mg morning and 150 mg evening) in patients with moderate or less severe psoriasis. The intervention group of this RCT was 22 patients with 20 control patients. At 6 weeks of treatment the authors report a significantly (p = 0.025) better outcome from the supplement of moclobemide compared with solely topical corticosteroids. Alpsoy et al. performed assessments with a range of psychometric instruments at study baseline and post-treatment, while Di Prima et al. did not perform any such assessments of patients. Alpsoy et al. found that reductions in several depression and anxiety scores were significant. However, the authors do not state if patients met a diagnosis of depression at study entry or if there was remission from depression in any of the patients.
An open-label study of the newer anti-depressive drug bupropion, a noradrenaline and dopamine reuptake inhibitor, in monotherapy showed a significant mean reduction of 50% in psoriasis-affected skin surface in 8 out of 10 patients at 6 weeks of treatment (49). In 3 responders a decrease in psoriasis extension of more than 75% was reported. It was also noted that 3 weeks after the cessation of bupropion there was a deterioration toward the baseline condition of the skin. The untraditional method of assessing the extension of psoriasis and not the intensity or thickness of lesions may be related to this study’s dual focus; investigating effectiveness of bupropion in both psoriasis and atopic dermatitis. However, the authors have stated that; “in all cases, decreases in affected surface area were associated with subjective reports of improvement in disease coverage, intensity, irritation and pruritus”.
A retrospective Swedish population cohort study examining the period 1997 to 2006 found that patients with psoriasis who had undergone treatment with an SSRI were less often switched to systemic treatment in the following years (50). A total of 69,830 patients with plaque psoriasis were identified in the National Swedish Patient Register. Whether study subjects were exposed to SSRIs was identified through a Prescribed Drug Register. The SSRI-exposed subjects (n = 1,282) had a prescription for SSRIs dispensed twice during 6 months at a Swedish pharmacy during a 2-year interval, with a wash-out period of one year or longer. In SSRI-exposed patients with mild psoriasis, defined by the use of non-systemic treatment prior to study inclusion, switching to systemic treatment in the following years occurred in less than half as many (n = 29) as in the equally large matched reference group (n = 64) odds ratio (OR) 0.44, 95% confidence interval (95% CI) 0.28–0.68. Possible benefits of SSRI treatment were also noted for severe psoriasis defined by the use of systemic treatment prior to study inclusion, with significantly more patients in the SSRI group tapering systemic treatment in the follow-up.
D’Erme et al. (51) investigated the outcome of augmenting a biopharmaceutical with an SSRI. Nineteen out of 38 patients receiving TNF-α inhibitors for their psoriasis were given the supplement of escitalopram 10 mg od. At 6 months there was a significant reduction in visual analogue scale (VAS)-pruritus scores, but no objective benefit or significant change in PASI for the skin was noted. However, remission of long-lasting psoriasis has been reported in 2 patients in relation to SSRI treatment (paroxetine) of comorbid major depression; remission lasting for a period of 12–18 months (52).
There are good indications that topical doxepin is effective in relieving pruritus secondary to atopic dermatitis (AD) and eczematous dermatitis (53, 54). A double-blind controlled trial by Drake et al. (54) showed significant improvement of AD with daily applications of topical doxepin 5% compared with placebo ointment at 7 days of treatment. On the other hand, there are, as far as we know, no studies of per orally administered TCAs or SSRIs for AD or other dermatitis, at least not in the time-period 1984 to 2016. However, the antidepressant bupropion has been investigated for AD in an open-label study by Modell et al. (49). In this study 6 weeks of treatment with the antidepressant bupropion was accompanied by a mean reduction of 50% in AD extension in 6 of 10 patients with AD; 3 weeks after bupropion discontinuation, affected areas increased and reached the pre-study condition in 3 responders.
Beneficial effects from antidepressants in the treatment of AA have been described in 3 controlled trials (55–57). However, only 2 of these trials were blinded. Patients withAA included in these studies presented with the comorbidity of either anxiety or a depressive disorder. In the study by Abedini et al. (56), 60 cases of recent onset AA were treated with triamcinolone injections in alopecic patches, with half of the patients (n = 30) randomized to also receive the open-label supplement of citalopram 20 mg p.o. At 6 months of treatment there was significantly more hair regrowth, as measured by reduced mean diameter of the alopecic patch, in the citalopram patients compared with the triamcinolone injection only patients (56). Citalopram was discontinued at 6 months, and patients were reassessed after another 6 months. Relapse of AA was noted in 20% of patients who had received the supplement of citalopram compared with 66.7% of patients who had only received triamcinolone injections.
Perini et al. (55) conducted a small placebo-controlled study with imipramine 75 mg od (TCA) in monotherapy for AA. At 6 months, hair regrowth was reported in 5 out of 7 patients treated with imipramine, with no regrowth noted in the placebo group of 6 patients. Similarly, a small RCT by Cipriani et al. (57) with a total of 13 patients with AA randomized to receive either paroxetine 20 mg (8 patients) or placebo (5 patients) reported a better outcome with paroxetine than placebo. Unlike other studies this study also includes more severe and resistant types of AA: alopecia totalis in 3 patients and alopecia universalis in one patient. Paroxetine was given for 3 months, with a follow-up at 4 and 6 months after treatment was discontinued. Complete regrowth of hair was observed in 2 patients treated with paroxetine, while 4 patients showed partial regrowth, which was not further defined. In comparison only one patient from the placebo group had an almost complete regrowth of hair. Unfortunately the authors do not state if patients with more severe types of AA were among those who improved.
All the studies in this review found that treatment with antidepressants, either in mono-therapy or as an adjuvant, relieved symptoms of the skin disorder, with 26/29 papers reporting improvement in skin lesions. Other beneficial outcomes were reduced pruritus, and a cohort study pointed to reduced need for systemic treatment in psoriasis. Overall, the results from the reviewed trials, and case reports indicate that antidepressants may be useful in the treatment of CU, psoriasis, AD, other dermatitis and AA. Benefits of per orally administered antidepressants emerged from within hours to a few weeks for CU, within 3–6 weeks for psoriasis and AD, and, in the case of AA, within 3–6 months.
In more than half of the reviewed papers psychiatric comorbidity was either not assessed or dismissed. We take the lack of psychiatric evaluation to reflect the common perception that TCAs are useful in CU for their anti-histaminergic properties. The awareness of psychiatric comorbidity in AA, on the other hand, may be related to the historic tendency to regard AA as a psychosomatic condition. Interestingly, most studies portray a more rapid alleviation of skin symptoms than depressive symptoms on treatment with antidepressants. The anti-depressive effects of antidepressants usually emerge with a delay of 1–3 weeks. These findings, and the increasing knowledge of anti-inflammatory potential in antidepressants may indicate that improvement in skin symptoms is not secondary and does not rely on improvement in mood or anxiety.
This review comprises 29 papers, of which 11 report results from double-blind, placebo-controlled trials or randomized controlled trials (RCT). RCTs of per orally administered antidepressants have been performed in CU, psoriasis and AA. RCT evidence is, however, limited mainly to antidepressants pertaining to the TCAs and the MAOIs. As far as we know there has only been one RCT of an SSRI performed in the context of a common skin disorder, namely AA.
Treatment with traditional MAOIs demands a strict diet, with serious cardiovascular risks of ingesting fermented foods high in tyramine. Most TCAs have prominent sedative properties due to anti-cholinergic and anti-histaminergic effects. Even in the studies of topical doxepin approximately 20% of the patients receiving active ointment reported drowsiness. These side-effects question the feasibility and credibility of blinding and placebo control groups in studies of TCAs and MAOIs.
The highest quality evidence, the RCTs, have several other weaknesses, and are not in accordance with current CONSORT (Consolidated Standards Of Reporting Trials) guidelines. Apart from the larger trials of topical doxepin in atopic and eczematous dermatitis, randomization procedures are not usually clarified and patient flow charts are often not supplied. The use of different outcome measures makes comparison of the study outcomes difficult. Given the inclusion of several different skin disorders in this review different outcome measures cannot be avoided altogether. However, even for specific skin disorders the authors assess the skin lesions and symptoms differently. While Greene et al. (29) use a 4-point scale for patient daily assessment of symptom severity in CU, assessments in Harto et al.’s study (38) involve a 3-point scale. And, even in the case of psoriasis, not all studies assess improvement with the PASI score.
Another evident weakness in the studies of per orally administered antidepressants is the small sample sizes, ranging from 9 to 60 patients, with a mean of 27 patients, enrolled in 11 studies. Studies with small sample sizes may especially be subjected to publication bias: it is difficult to publish a study with negative results, especially if the study is small. Small sample sizes also make it difficult to generalize about the findings even when these are statistically significant. Unfortunately, even the larger studies in this review fail to convey whether significant findings constitute clinically meaningful improvements in psoriasis, eczema or the other skin disorders.
Traditional antidepressants involve the enhancement or modulation of monoamines, mainly noradrenaline and serotonin, but also dopamine and melatonin, at the synaptic level. Monoamines are involved in the regulation of endocrine and immunological responses, and the autonomic nerve system (58). After release into the synaptic cleft, monoamine neurotransmitter action is ended by reuptake into the presynaptic terminal. The SSRIs selectively inhibit the reuptake of serotonin. The MAOI antidepressants inhibit the enzyme monoamine oxidase (MAO), causing an increase in monoamine levels in the synaptic cleft by blocking their break-down. Anti-depressive effects of monoaminergic antidepressants usually occur with a delay of 1–3 weeks and are commonly thought to rely on alterations in neurotransmission secondary to changes in levels of serotonin and noradrenaline and dopamine in the synaptic cleft. However, monoamines and monoamine receptors are not limited to the brain and nervous system, and antidepressants exert actions beyond the manipulation of neurotransmission (59, Fig. 1).
Most of the body’s supply of serotonin (5-hydroxytryptamine; 5-HT) is produced in the gut and stored in platelets, and 5-HT is an important regulator of gut mobility and vascular tonus. Furthermore, serotonin and monoamine receptors have an important role in immune signalling (60, 61). The immune system and the brain communicate through both neural and humoral mechanisms that involve serotonin. In the skin, increased expression of the serotonin transporter receptor (SERT) on dendritic mononuclear cells has been linked to psoriatic inflammation (62). There are several indications that serotonergic mechanisms are involved in contact allergic responses (63). One recent study points to altered and increased expression of certain SERTs in AD lesional skin compared with unaffected skin (64). In addition, it has been proposed that serotonin and/or SERT may play a role related to the cell adhesion molecule P-selectin in delayed pressure urticaria (45).
Antidepressants are lipophilic which is essential for them to cross the blood brain barrier (65). Experimental studies suggest that SSRIs interfere with calcium influx and the cAMP/PKA and JAK/STAT messenger pathways that regulate the release and transcription of pro-inflammatory cytokines from activated microglia (66, 67). The exact mechanisms involved in antidepressants’ anti-inflammatory actions, both in the CNS and in the peripheral tissues, however, have not yet been fully elucidated.
Unwanted side-effects may limit the use of TCAs and MAOIs, both in psychiatric care and dermatological practice. The newer antidepressants SSRIs, bupropion and mirtazapine have the benefit of being significantly less cardiotoxic and having fewer adverse effects than the older TCAs and the MAOIs. Some dermatologists may be wary of antidepressants due to reports of adverse events of skin rashes. However, none of the trials reviewed describe any incident of skin rash or hypersensitivity. Sensitization, however, has been recognized as a problem with topical doxepin, which has largely been abandoned. Per orally administered antidepressants, on the other hand, are widely prescribed. Side-effects are usually mild and transient, typically involving gastrointestinal and vegetative symptoms, and serious adverse reactions including hypersensitivity are relatively rare (68). Although extremely rare, the clinician should be aware that antidepressants may induce suicidal thoughts and acts of self-harm or violence, with young patients < 18 years being more vulnerable.
The findings of this review point to beneficial effects of treatment with antidepressants in common inflammatory skin disorders, which may be due to the immune-regulatory capacities of these agents. It is not clear if antidepressants have a purpose in the treatment of common dermatological disorders in the absence of psychiatric comorbidity. In our opinion, however, the literature supports the use of antidepressants in the treatment of comorbid depression and anxiety disorders in patients with psoriasis, AA, AD and other dermatitis. Based on experimental studies dosages in the upper range of current indications may be necessary to exploit the anti-inflammatory properties of antidepressants (5, 66). Doxepin may be of value in the treatment of CUs and possibly even in refractory inducible types. However, larger controlled trials are needed to provide further evidence. Based on current evidence and tolerability concerns we specifically recommend investigating newer antidepressants in the treatment of dermatological disorders.
This research was partly supported by Lovisenberg Diakonale Hospital.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize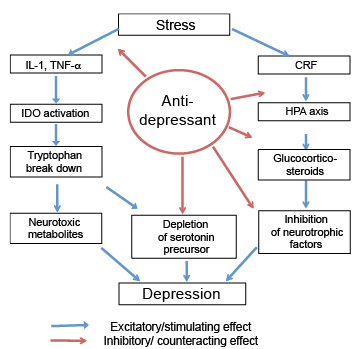 Click to show fullsize
Click to show fullsize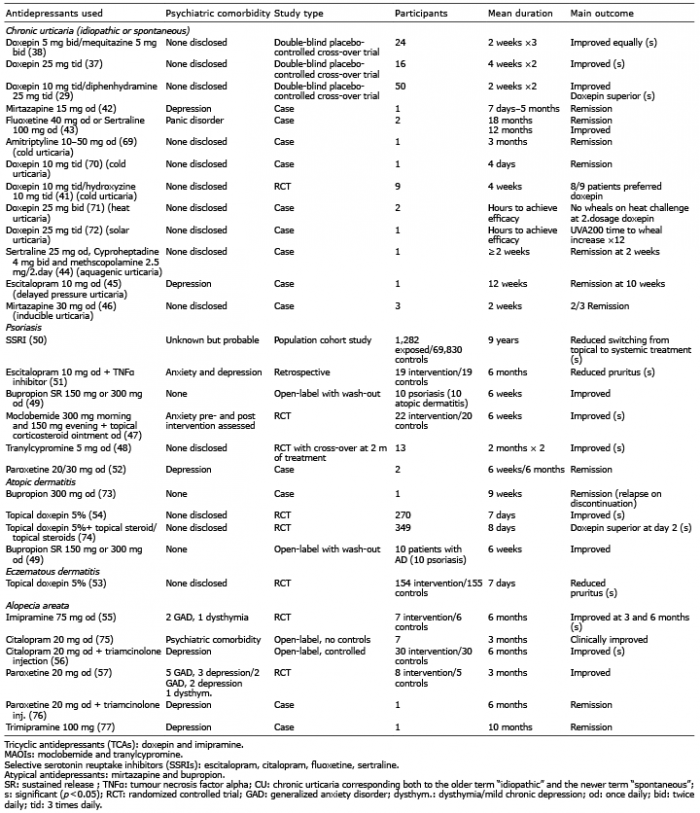 Click to show fullsize
Click to show fullsize