


1Department of Health Sciences, Institute of Health and Society, Medical Faculty, University of Oslo, 2Section for Climate Therapy, 3Department of Dermatology, Oslo University Hospital, Oslo, Norway, and 4Department of Dermatology, Sahlgrenska Academy at University of Gothenburg, Gothenburg, Sweden
Alexithymia, defined as difficulty in describing or recognizing emotions, has been shown to be connected with psoriasis, but its relationship with self-management of psoriasis has not been explored. The aim of this study was to assess the frequency of alexithymia and its relationship with self-management and illness perception in the context of psoriasis. A total of 163 patients participating in 3 weeks of climate heliotherapy (CHT) at Gran Canaria were assessed for alexithymia using the Toronto Alexithymia Scale (TAS-20) at baseline. Self-reported measures for self-management (Health Education Impact Questionnaire; heiQ), and disease severity and illness perception (Brief Illness Perception Questionnaire; BIPQ) were assessed twice. Of all patients, 14.1% were characterized as alexi-thymic and 22.1% scored in the intermediate range. Alexithymic patients scored significantly worse in all heiQ domains, and reported worse illness perception. However, there were no between-group differences in heiQ or BIPQ change from baseline to after CHT. In conclusion, this study shows that alexithymia indicates inferior self-management and reaffirms the associations with illness perception. Further research is required into these relationships.
Key words: psoriasis; alexithymia; self-management; illness perception.
Accepted May 22, 2017; Epub ahead of print May 24, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Marie Hamilton Larsen, Department of Health Sciences, Institute of Health and Society, University of Oslo, PO Box 1089 Blindern, NO-0317 Oslo, Norway. E-mail: m.h.larsen@medisin.uio.no
Psoriasis is a chronic inflammatory skin condition that has been recognized recently as an autoimmune-mediated disease (1). Patients with psoriasis have an increased risk of concurrent disorders, including hypertension, obesity, diabetes and cardiovascular disease (2–4). The unpredictable nature of psoriasis often has consequences for psychological well-being (5), and people affected by psoriasis have inferior health-related quality of life (QoL) compared with the general population (6). Psoriasis is also linked to psychological comorbidities, such as anxiety, depression and pathological worrying (7, 8).
Alexithymia is a personality dimension, characterized by different cognitive and emotional features, such as difficulty in describing and identifying emotions, problems communicating feelings, and limited imagination (9). As such, individuals with alexithymia have problems distinguishing somatic manifestations of emotions and tend to misinterpret their emotional arousal as signs of physical disease (10).
Studies have investigated the prevalence of alexithymia and found that it is elevated in both psoriasis (11, 12) and in other autoimmune diseases, such as systemic lupus erythematosus (SLE) and rheumatoid arthritis (13). Also, in patients with other chronic conditions, such as chronic pain (14), fibromyalgia (15) and chronic obstructive pulmonary disease (COPD) (16) studies have revealed increased prevalence of alexithymia. A recent multicentre study found that patients with alexithymia had a higher burden of psoriasis, as well as significant impairment of QoL, higher levels of depression and anxiety and impairment of work productivity, compared with patients without alexithymia. In Chinese patients with COPD male patients presented higher alexithymia scores compared with women (17).
Self-management is defined as: “The tasks that an individual must undertake to live well with one or more chronic conditions. These tasks include gaining confidence to deal with medical management, role management, and emotional management” (18). The strain of daily self-management has been described as demanding and difficult in psoriasis (5, 19), and several studies show that patients fail to adhere to both treatment and customized lifestyle (20, 21). However, self-management is a key element in the overall management of psoriasis, and identifying barriers to disease self-management may be a critical step in achieving optimal health outcomes. A study investigating the impact of alexithymia on asthma management, found that higher alexithymia scores were associated with worse asthma control (22). This may also indicate a possible relationship between alexithymia and impaired self-management in other chronic conditions that involve extensive management responsibilities for the patients. In psoriasis there has been no previous research on this possible relationship.
Illness perceptions are the organized cognitive representations or beliefs that patients have about their illness (23). A variety of psychological frameworks exist to explain patient health-related activities in response to illness (24–26). One influential framework is the Leventhal’s Common-Sense Self-Regulation Model (CS-SRM) (23). This framework advocates that individuals faced with a health threat have a tendency to form emotional and cognitive images about their condition. These representations are important determinants of the coping strategies and behaviours individuals adopt in response to their perceived health problem (27).
Alexithymia may impact on the psychosocial responses of patients towards their psoriasis. Alexithymia may also influence responsiveness to change in clinical encounters or impact on the effects of self-management interventions. Exploring the relationships between patient’s illness perceptions, self-management and the influence of alexithymia may therefore be of crucial importance for good clinical care. A significant proportion of patients with chronic diseases do not respond to self-management interventions (28). This may suggest that “one size” interventions do not fit all and that additional tailored interventions are needed. To compose more individualized strategies, we may need to increase our understanding of characteristics associated with patient activation for self-management.
The main aims of the present study were to investigate alexithymia and its relationships with self-management and illness perception in patients with psoriasis undergoing climate heliotherapy (CHT). Determining these relationships may contribute to a more comprehensive understanding of psoriasis, its impact on patients’ daily lifestyles, and patients’ perception and management of the disease. To our knowledge this is the first study to assess the inter-relationships between alexithymia, illness perception and self-management in this group of patients.
The study consists of 163 Norwegian patients with psoriasis participating in CHT in Gran Canaria. Patients were recruited to the study when they arrived at the treatment site and completed a battery of questionnaires at arrival and after 3 weeks of treatment. The sample used in this study is all pre-randomization assessments from a randomized controlled trial (RCT) investigating the effect of a telephone-based motivational interviewing intervention (29, 30) that took place in the 12-week period after CHT. The patients were all diagnosed with psoriasis with Psoriasis Area Severity Index (PASI) score > 7.0 when applying for CHT, age range 20–70 years, and able to answer questionnaires in Norwegian.
Throughout the study, the principles outlined in the Declaration of Helsinki (31) were followed. The study was approved by the research director and the Centre for Privacy and Information Security at Oslo University Hospital and also by the Regional Committee for Medical Research Ethics for Southern Norway (ID: 2011/1019) and registered at: http://www.clinicaltrials.gov (ID: NCT 01352780).
A socio-demographic questionnaire was designed to collect information on the patients’ age, educational level, sex, family income and working status. All patients were assessed by an experienced dermatologist at arrival and after 3 weeks of CHT for PASI score. A self-administered battery of existing, reliable and validated questionnaires was used to measure the outcome variables described below.
Alexithymia was assessed at baseline using the Norwegian translation of the Toronto Alexithymia Scale (TAS-20). The TAS-20 is considered the gold standard for the assessment of alexithymia and has been repeatedly and widely used in various clinical and research settings (32, 33). The scale has good psychometric features of factor stability, reliability and validity (10). The TAS-20 consists of 3 subscales that measure difficulty in describing feelings (DDF), difficulty in identifying feelings (DIF) and externally-oriented thinking (EOT), respectively.
Alexithymia can be described using both continuous data and categorical scoring methods. In categorical approaches the suggested cut-off (11) often indicates that a score above 61 indicates alexithymia, a score between 51 and 60 (both scores included) suggests intermediate or borderline alexithymia, and a total score below 51 indicates absence of alexithymia. For the purpose of statistical comparisons, 2 extreme groups were created, with the cut-off value of 61 to dichotomize patients with psoriasis into alexithymic and non-alexithymic individuals. Consequently, borderline patients were analysed in the non-alexithymic group. Cronbach’s alpha was 0.85 with all items and for the 3 subscales αdif=0.83, αddf=0.75, which delineates good internal consistency of these subscales, and αeot=0.60, indicating borderline consistency.
Self-management was assessed before and after CHT with the Health Education Impact Questionnaire (heiQ), which is constructed to measure proximal outcomes for patient education and self-management interventions, among patients with chronic conditions (34). The questionnaire comprises 40 items across 8 independent scales. The domains are: positive and active engagement in life, emotional well-being, self-monitoring and insight, constructive attitudes and approaches, skill and technique acquisition, social integration, and support and health service navigation (34, 35). A higher score indicates better self-management related to the specific scale, and a lower score indicates inferior self-management, except for the emotional distress scale, which is reversed. Cronbach’s alpha for the heiQ domains ranged from 0.65 to 0.89.
The Dermatological Life Quality Index (DLQI-N) is the most frequently used QoL instrument related to dermatology (36). Higher scores indicate greater impairment of a patient’s QoL. The reliability and validity of the DLQI is well established (37). Due to the questions related to the home environment DLQI was only measured at baseline. Cronbach’s alpha for this study was 0.90.
The Brief Illness Perception Questionnaire (BIPQ) was applied twice. It comprises 8 items, each assessing one dimension of illness perception (consequences, timeline, personal control, treatment control, descriptions of the condition and symptoms, coherence and concern and emotions) (36). The overall summed score for BIPQ was computed as described on the BIPQ website (http://www.uib.no/ipq/index.html). The maximum score is 80, where higher scores reflect a more negative perception of psoriasis. In this study, Cronbach’s alpha was 0.70.
CHT includes a 3-week programme in Gran Canaria. The main helio-treatment is individualized sun exposure in increasing doses, dependent on skin type and current ultraviolet (UV) index. The good therapeutic response to CHT is accomplished through sun-induced reduction of the inflammatory infiltrate in the skin and normalization of keratopoesis (38). The CHT programme also emphasizes daily physical training, tailored education, group discussions and individual consultations and supervision by nurse, physiotherapist and dermatologist. Thus, the 3 weeks of CHT include scheduled sun treatment, patient education on topics, such as treatment options, skin care and healthy behaviours (i.e. exercise and stress management). Previous research has shown positive effects of CHT on several outcomes, such as disease severity, measured by PASI and Self-Administered Psoriasis Area and Severity Index (SAPASI) (30, 39), QoL (29) and psoriasis literacy (40). A further description of the impact of the CHT programme on illness perception and self-management has been described in previous studies (30, 39, 41).
SPSS statistical package version 22 (SPSS Inc., Chicago, IL, USA) was used to perform the analyses. Baseline characteristics were examined using descriptive statistics. Continuous data are presented as means and standard deviations (SD) and 95% confidence intervals (95% CI), or median and min–max values. PASI score was dichotomized as “medium severity psoriasis”(PASI < 10) and severe psoriasis (PASI 10.1 or above) at arrival. Educational level was dichotomized as “low” (below 12 years’ primary school level) and “high” (above 12 years’ of primary school). Two-sided p-values < 0.05 were considered statistically significant. For analysis of continual nature the independent sample t-test for observations with normal distribution was used. The Mann–Whitney U test was performed if the continual observations did not show normal distribution. For categorical data the Pearson’s χ2 test/Fisher’s exact test was used. To assess possible relationships between the different measures the Pearson’s correlation coefficient statistics (r) was used for continuous variables, which were normally distributed, whilst the Spearman’s rho statistic (q) was used for ordinal or non-normally distributed variables. To determine whether participation in CHT (from baseline (T1) to after CHT (T2)) give different results for subjects with alexithymia compared with the non-alexithymic group, analysis of covariance (ANCOVA) was used, controlling for the T1 values (General Linear Model procedure in SPSS). ANCOVA analysis was also used to control for age and sex, as these factors have previously been shown to differ in alexithymic subjects (32, 42).
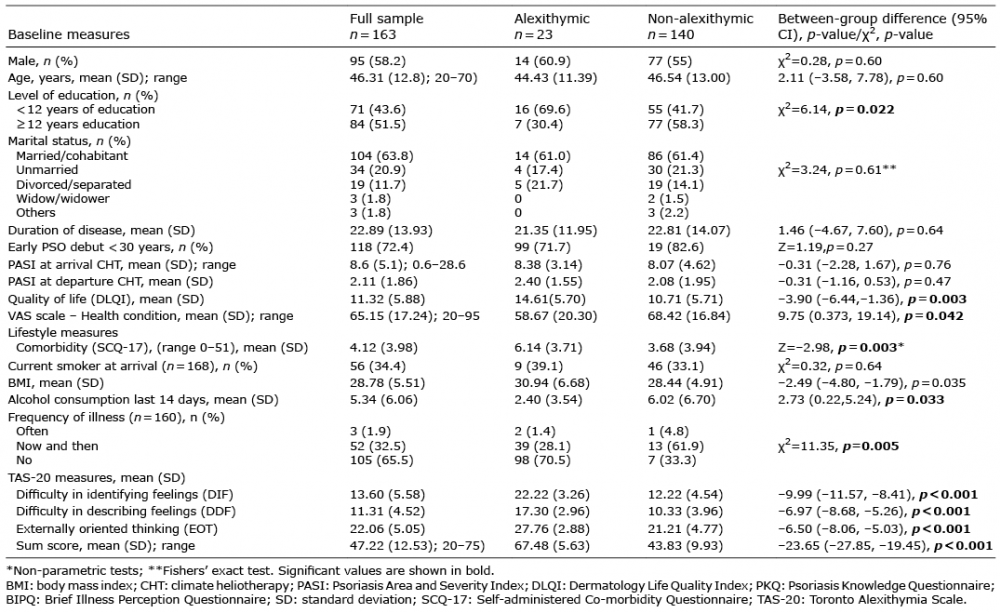
Sample demographics, patient-reported outcomes and psoriasis severity are summarized in Table I. In total, 95 men (58.2%) and 68 women (41.7%) participated in the study. Participants had a mean (SD) age of 46 (12.8) years and 43.6% had less than 12 years of education.
Table I. Sample demographics and psoriasis severity: difference between alexithymic and non-alexithymic patients
Most patients were married or cohabitant (63.8%) and had a mean (SD) disease duration of 22.9 (3.9) years. A total of 34.4% were smokers on arrival in Gran Canaria and 74.5% had a body mass index (BMI) above 25. They had a mean (SD) PASI of 8.6 (5.1) on arrival and a disease-specific QoL (DLQI) of 11.2 (5.9), indicating a strong negative impact on their QoL.
The mean (SD) score on the TAS-20 was 47.2 (12.5). Scores ranged from 20 to 75 across the sample. 14.1% (n = 23) showed alexithymia, 22.1% (n = 36) had borderline alexithymia, while 63.8% (n = 104) had no alexithymia. The mean (SD) TAS score for the alexithymic patients was 67.83 (5.63) and 43.83 (9.93) for the non-alexithymic group. Neither the TAS-20 total score, DIF score, DDF score nor EOT score, showed significant sex differences (results not shown). The alexithymic patients reported fewer years of education (χ2=6.14, p = 0.022) and a higher BMI (p = 0.033). However, there were no differences related to early or late psoriasis debut (Table I).
There were no significant differences in PASI score at baseline between the 2 groups. There were no correlations between PASI at baseline and TAS-20 sum score or EOT score. A small positive correlation significant at the 0.05 level was found between PASI and the subscales DDT and DIF. Regarding the possible effect of psoriasis severity on alexithymia, no significant differences of alexithymia and its dimensions between patients with severe (PASI>10) and less severe psoriasis were found.
However, outcomes related to illness and health showed that the alexithymic patients scored significantly higher on the self-assessed Comorbidity scale –2.46 (–4.24, –0.68), p = 0.007 and reported elevated frequency of illness; (χ2 = 11.35, p = 0.005) compared with the non-alexithymic patients. The alexithymic patients also had significantly poorer disease-related QoL at the start of the climate treatment measured by DLQI; –3.90 (–6.44, –1.36), p = 0.003.
Higher alexithymia scores were associated with lower reports of self-management in all 8 heiQ domains, with medium-sized correlations, significant at the 0.01-level. The reversed heiQ scale “Emotional wellbeing” had a positive strong correlation with the DIF score (Difficulty Identifying Feelings) in TAS-20 (r = 0.55, p = 0.01), showing that a lower level of wellbeing is associated with higher difficulties identifying emotions.
In order to explore the relationship between alexithymia and illness perception, correlations between TAS-20 sum score and BIPQ were examined, showing a borderline strong positive correlation (r = 0.49, p = 0.01). A medium correlation was found between BIPQ and the 3 TAS-20 subscales; difficulty in describing feelings, (r = 0.45, p = 0.001), difficulty in identifying feelings (r = 0.49, p = 0.01), and externally-oriented thinking (r = 0.21, p = 0.01). Hence, inferior illness perception is related to higher alexithymia scores.
At baseline and after 3 weeks of CHT, the persons with alexithymia (TAS > 61) scored significantly lower on 7 of the heiQ domains measuring outcomes of self-management and patient educational interventions compared with the non-alexithymia persons (TAS 20 ≤ 60). In the last domain, measuring “Emotional wellbeing”, the alexithymic patients also scored worse, as this scale is reversed (Table II). Also, when comparing the patients with borderline alexithymic with non-alexithymic patients, we found significant differences in 5 of the 8 domains (results not shown).
Table II. Self-management outcomes for alexithymic and non-alexithymic patients with psoriasis (n = 162)
At baseline, alexithymic persons scored significantly worse in 4 of the 8 illness perception dimensions representing “Consequences”, “Illness concern” and” Emotional representation”, (all p < 0.001), and “Coherence” (p = 0.049). After 3 weeks of CHT there were still significant differences related to “Consequences”, “Emotional representation” and “Illness concern” (p < 0.05). The BIPQ sum score also showed significant differences both at baseline and after CHT (Table III). There were also significant differences between borderline alexithymic patients and non-alexithymic patients for both the total BIPQ score and the same 4 dimensions at baseline.
Table III. Illness perception (BIPQ) scores for alexithymic and non-alexithymic patients
Analysis of covariance (ANCOVA) with the heiQ dimension after CHT (T2) as the dependent variable and the baseline heiQ value (T1) as covariate, showed no significant differences in change in any of the heiQ dimensions between the alexithymic and the non-alexithymic persons, when controlled for age, sex and educational level (Table II).
This means that the effect of CHT is the same for alexithymic and non-alexithymic patients with regard to self-management. In relation to severity of psoriasis measured by PASI, the effect of the CHT treatment was the same in the 2 groups (Table I). The same trend was also found regarding illness perception, as none of the 8 dimensions showed significant differences in change from baseline between the groups (Table III). QoL after CHT was not measured, as the DLQI has too many questions related to normal life at home, and thereby seems not suited after spending 3 weeks in Gran Canaria.
The aims of the current study were to investigate alexithymia and identify relationships between socio-demographic characteristics, self-management, illness perception and alexithymia in patients with psoriasis undergoing CHT, and, secondly, to assess to what extent being alexithymic impacts on change in self-management and illness perception after participation in 3 weeks of CHT.
Only a moderate percentage of the patients with psoriasis in our population could be considered alexithymic. Together, the alexithymic and borderline alexithymic patients make up 36.2% of the participants in the study. However, the prevalence of high TAS-20 score is lower in our study than in several other psoriasis studies (11, 12, 43). This low prevalence of alexithymia detected in the current study is somewhat surprising. However, the prevalence is higher than in the general population, where it has been found to be in the range 10–12% (44). One explanation might be that our sample entailed a before-randomization population, with psoriasis patients in a study that aimed to examine the effect of individualized motivational interviewing. Of the eligible participants in the CHT programme 38.8% declined to participate in this study (30), and it might be that patients with alexithymia are less motivated to participate in such a study. Also, we do not know whether alexithymic patients in general choose other treatment options than applying for CHT. It is possible that a 3-week treatment programme that includes personal communication and relations with the multidisciplinary healthcare team and peers might feel more intrusive to alexithymic patients who are unable to express their emotions appropriately.
No sex differences were identified in the prevalence of alexithymia. A slightly higher percentage of men scored above the cut-off for alexithymia, but this did not reach statistical significance. Studies within other chronic conditions have, however, found that a personality trait such as alexithymia is more typical in men than in women (22, 32). No relationships were identified between alexithymia and the severity of psoriasis measured by PASI score. This has also been found in other studies (43) and may indicate that alexithymia is a fairly stable trait and not a reaction to chronic illness, influenced by duration or severity. There were also no differences related to early or late debut of psoriasis (with 30 years cut-off).
Our study also found a poorer outcome in disease-related QoL measured by DLQI. Another study investigating relationships with alexithymia in psoriasis has found similar results (45). This is also in line with a previous study of a general population with the generic measure 15D (32). The alexithymic participants were also associated with increased somatization, with a higher score on the Comorbidity scale. Thus, proneness to increased symptom reporting may also be reflected in the disease-related QoL scores of alexithymic subjects.
This study indicates that higher alexithymia scores are associated with lower self-management in patients with moderate to severe psoriasis participating in CHT. This was also, to a large degree, true for the participants with borderline alexithymic scores. This association suggests that patients with higher alexithymia scores, and thereby reduced perception of their feelings, may require increased follow-up or a more tailored self-management support than other patients with psoriasis. Furthermore, poor communication between patients with psoriasis and their healthcare providers has been associated with lower adherence to symptom management (46). Poor self-management may also be associated with the influence of alexithymia on the quality of communication between patients with psoriasis and healthcare professionals. These relationships need to be examined further. Alexithymic patients tend not to use complex or nuanced emotional language, but are more prone to express themselves in bodily symptoms or deliver excessive health details (47). Hence, knowledge of a patient’s level of alexithymia may guide our understanding of their health status, clinical presentation, behaviour, and responses to treatment.
The fact that patients with alexithymia also had inferior illness perception, underscores the possible need for a more tailored follow-up. The findings of our study support the hypothesis that, in patients with psoriasis, emotion regulation style exerts a significant effect on perceived health (48). In particular, alexithymic patients reported worse perceived consequences of the disease on their lives, worse illness concern, and registered higher emotional representation of psoriasis. These results may be explained by difficulty in identifying, managing and expressing emotions, which may have led to poor self-management and QoL. However, we found no significant effect for other BIPQ scales. These results might be explained by the unpredictability and variability of manifestations of psoriasis physically, psychologically and on a social level.
The study found that alexithymic patients participating in the CHT programme had just as much effect regarding self-management (heiQ), illness perception and PASI score. This may indicate that the CHT programme is mostly bio-medically focused, which alexithymic patients prefer. Conversely, the psychological and emotional focus in CHT is, to a great extent, delivered as non-mandatory sessions in addition to the obligatory programme. However, the empathetic manner in which the interdisciplinary CHT staff meets and interacts with the patients may be of extra importance for patients with alexithymia and may also contribute to the good overall results of the stay (47).
Our study was subject to several methodological limitations: first, the population studied was not randomly selected from a clinical population and several biases may have affected the willingness of the volunteers to participate in the study. The previously mentioned intervention style of motivational interviewing, which requires an interpersonal relationship between the client and the supervisor, may be one reason for selection bias. However, our aims were to test associations between physical and psychological variables rather than to study a representative sample suitable for epidemiological description.
The fact that we cannot compare our results with a control cohort that is not participating in CHT is also a limitation. This would have allowed us to investigate whether our findings were unique to the CHT population. Another limitation of this study is that we cannot compare the alexithymic score at 6 months after CHT, because some of the participants by then had received a 3-month telephone-based MI intervention that may have impact on alexithymia. In addition, we did not measure the patients’ level of depression, and this factor may also influence illness perception, QoL and, possibly, self-management. Therefore, we are not able to control for negative possible effects. Alexithymia has shown to have a close relationship to depression in the general population (49) and in psoriasis (50).
Our findings suggest that studying the role of psychological factors, such as alexithymia and illness perception, may contribute to a more comprehensive perspective of psoriasis, including the impact of these factors on the patient’s beliefs about treatment effectiveness, self-management and emotional adaptation to a chronic disease. Further research is needed to map these possible relationships. Knowledge of a patient’s alexithymia level may guide our understanding of health status, clinical presentation, behaviour, and responses to treatment.
The authors would like to thank the participants in this study and the Scandinavian nurses at the OUS Climate Therapy centre Valle Marina at Gran Canaria who contributed to the data collection. The study is funded by the University of Oslo.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize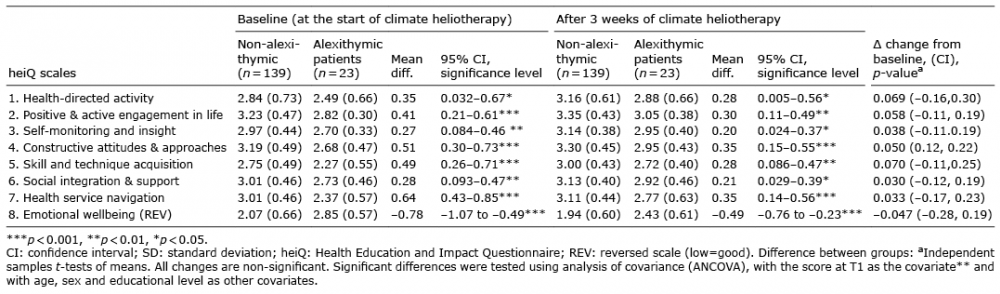 Click to show fullsize
Click to show fullsize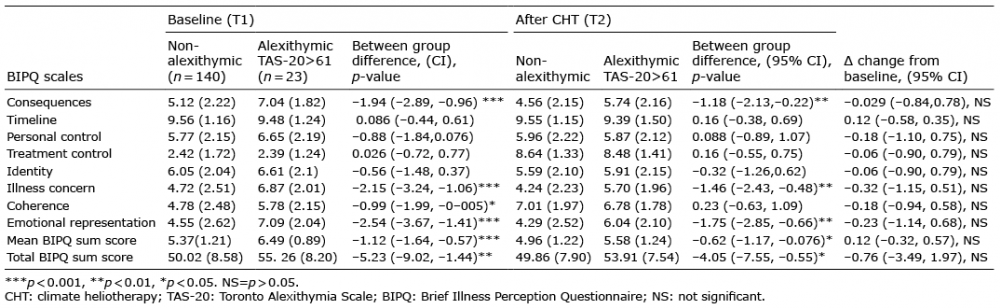 Click to show fullsize
Click to show fullsize