


1Dermatology Department, Centre hospitalier Lyon Sud, Claude Bernard University, Lyon 1 – Lyon, France, 2Dermatology Department, Melanoma Unit, Hospital Clínic de Barcelona, IDIBAPS, Universitat de Barcelona, and 3Centro de Investigación Biomédica en Red en Enfermedades Raras (CIBERER), Barcelona, Spain
Early detection is a key strategy for reducing the mortality and economic burden associated with melanoma. Dermoscopy is a non-invasive and cost-effective tool for melanoma diagnosis, which has been shown to be a reliable and sensitive method for detecting early-stage skin cancer and reducing the number of unnecessary excisions. Patients at high risk of developing melanoma require long-term surveillance. Use of digital dermoscopy follow-up of these patients has led to improved outcomes. Combined follow-up programmes using total-body photography and digital dermoscopy have led to further improvements in early diagnosis and diagnostic accuracy. Dermoscopy is now widely used by dermatologists, but the public health impact of this tool is yet to be evaluated. Despite the clear advantages of dermoscopy and digital follow-up
meth-ods, dermoscopy training and access to digital dermoscopy among dermatologists and general practitioners needs to be improved.
Key words: melanoma; dermoscopy; diagnostic tool; skin imaging; dermoscopy.
Accepted May 22, 2017; Epub ahead of print Jul 3, 2017
Acta Derm Venereol 2017; Suppl 218: 14–21.
Corr: Susana Puig, Dermatology Department, Hospital Clinic, C/Villarroel 170, ES-08036 Barcelona, Spain. E-mail: susipuig@gmail.com
The incidence of skin cancer has been increasing worldwide over the past few decades (1). In particular, the incidence of malignant melanoma has increased exponentially over time in populations with European ancestry and skin types I–III (2), with 132,000 melanomas currently reported worldwide each year (1). How-ever, with the development of primary and secondary melanoma prevention measures, the US 5-year survival rate in type I–III individuals has risen significantly, from 40% in the 1940s and 68% in the 1970s to 93% in 2002 (p < 0.05) (3). The estimated 10-year survival rate in France is approaching 95% (4). Of all secondary prevention measures, earlier detection of early-stage melanoma is the most likely cause of improved survival among this most-at-risk white population (5). Although the first steps of progression to melanoma are well known and no one should die from this disease (6), melanoma is still underdiagnosed in dermatological practice. In 2003, melanoma was the second most common cause of lawsuits for malpractice in the USA and in 70% of cases the claims were for false-negative diagnoses (7), although the number of claims has declined significantly in recent years (8). The greatest issue is that differential diagnosis between a benign lesion and melanoma is difficult to ascertain: the chance of a small black mole, among numerous similar moles on the back of a patient being melanoma is very low (approximately 1 in 2 million (9)) and most often melanoma and benign naevi look too similar to be distinguished, even by an expert eye. One way to differentiate these 2 lesions with certainty is pathological analysis of a biopsy specimen; however, this is not feasible in individuals with multiple naevi, where every excisional biopsy leaves undesirable scars and because there is a high prevalence of benign moles. It is therefore important to recognize the early stages of melanoma and to develop tools for diagnosis to avoid unnecessary excision of moles that have a strong chance of being benign. In patients with a personal or familial history of melanoma or those with numerous naevi who are at high risk of developing melanoma, follow-up of patients is a key strategy for early diagnosis and further improving survival. We describe here how the use of dermoscopy and digital follow-up are leading to earlier detection of melanoma and a reduction in the number of excisions, even for lesions with atypical pigmentation patterns and in high-risk populations.
Dermoscopy is a non-invasive diagnostic method based on microscopy of the skin surface that allows better visualization of the internal structures of lesions, underneath the stratum corneum. Two systems have been developed: immersion dermoscopy using fluid (such as mineral oil) to improve contact between the lens and the skin and decrease light reflection by the stratum corneum, and polarized light dermoscopy using a filter to block reflected light. Dual-mode dermoscopy incorporates both systems and can be used in various mode combinations (immersion dermoscopy ± polarized light and polarized light dermoscopy ± immersion), to allow either optimal visualization of superficial structures closer to the skin surface with the immersion dermoscopy mode, or examination of deeper skin components by switching to the polarized light mode.
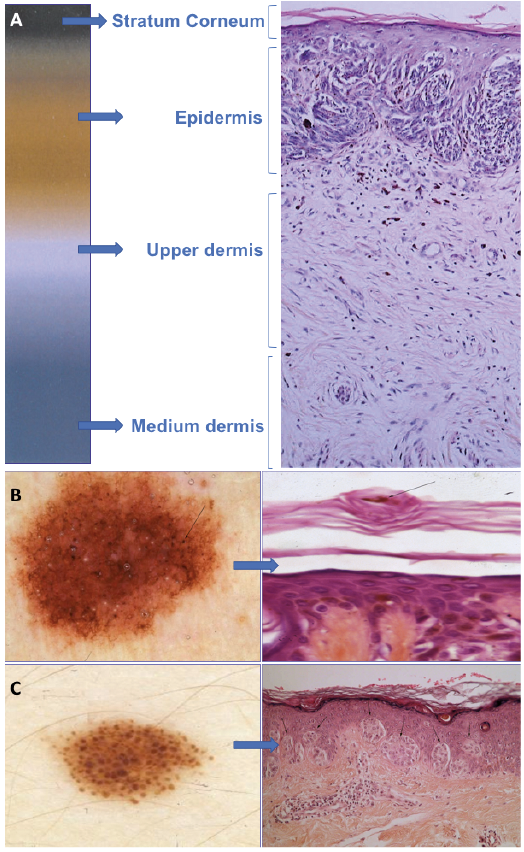
The main principles of dermoscopy are based on colour and structure (10, 11). Colour is used to evaluate the depth of pigmentation in the dermis, ranging from dark (black) when the pigmentation is in the corneum layer to lighter (blue) when the pigment is deeper in the dermis (Fig. 1A). The pigmented structures viewed by dermoscopy reflect the anatomy of the lesion, e.g. reticulation reflects the shape of the dermal–epidermal junction, dark spots correspond to pigment in the stratum corneum (Fig. 1B), globules correspond to pigment at the dermal-epidermal junction or inside the dermis in nested naevi (Fig. 1C). However, extensive training is required, as dermoscopic features vary greatly between lesions from different sites, with certain localizations (e.g. face, palms and soles, nails, mucous membranes, scar tissue) giving rise to unique pigmentation patterns. Experts in dermoscopy usually use a heuristic approach, but a more analytical method is required during dermoscopy training and in difficult cases. The analytical approach uses positive and negative criteria, key features, pitfalls and algorithms to aid the diagnosis. The Asymmetry, Border, Color and Differential Structures (ABCD) rule devised by Stolz et al. in 1994 (12) allows semiquantitative analytical interpretation of dermoscopic images. Using this system each criterion is accorded a score that is then used to calculate the Total Dermal Score (TDS). Lesions with a TDS > 5.45 are considered to be highly suggestive of melanoma. This scoring system is useful as a dermo-scopy training tool and in difficult-to-diagnose cases. However, the ABCD rule cannot be applied to the analysis of lesions with atypical pigmentation patterns or those arising in certain locations. Studies of large series of patients have allowed lesion-specific dermoscopic criteria to be defined for the detection and differential diagnosis of some of these lesions, such as facial lentigo maligna melanoma (13, 14), pigmented and non-pigmented acral lentiginous melanoma (ALM) occurring on palmoplantar skin and in the nail apparatus (15, 16), and even amelanotic and hypomelanotic melanoma (17) (Table I).
Fig. 1. Colours and structures viewed by dermoscopy. (A) Colour scale of dermoscopy images depending on the depth of pigment in the dermis. (B) Dark dots viewed by dermoscopy corresponding to pigment in the stratum corneum (arrow). (C) Globules (arrows) viewed by dermoscopy corresponding to pigment at the dermal-epidermal junction or in the dermis in nested naevi.
Table I. Key lesion-specific dermoscopy findings indicating the presence of melanoma
Several meta-analyses have shown conclusively that dermoscopy improves the accuracy of diagnosis of pigmented lesions when performed by experienced examiners (18–20). Dermoscopy also reduces the number of unnecessary excisions, with a recent study showing that the number of excisions of naevi has decreased in specialized centres over the 10-year period from 1998 to 2007, whilst the number of melanomas excised at these centres has increased (LT: unpublished observation, (21)). Use of dermoscopy is therefore essential in all difficult to diagnose lesions, which may include cases of seborrhoeic keratosis, dermatofibroma, basal cell carcinoma, angioma, naevi, melanoma and unpigmented lesions.
A study in France has shown that dermoscopy is now used by nearly 95% of private practice dermatologists nationwide, with the majority of these physicians receiving training for more than 5 years (60%), through meetings and books (89% and 76%, respectively) (22). Globally, the dermatologists participating in this study were in agreement that dermoscopy increases early detection of melanoma, reduces the number of unnecessary excisions and reduces patient anxiety, but approximately 30% did not find that dermoscopy reduces anxiety among physicians (22). This finding may reflect a lack of confidence among dermatologists in their ability to achieve a correct diagnosis using this technique. Several factors influence the level of use of dermoscopy among physicians: sex (female dermatologists are more likely to use dermo-scopy than males (96% vs. 92%, p = 0.002) and age (dermatologists below the age of 45 years are more likely to use dermoscopy than physicians > 63 years of age (97% vs. 89%, p = 0.013) (22). A similar study conducted in French hospitals also revealed that physicians working in hospital dermatology units recognize the advantages of dermoscopy in the diagnosis of melanoma, and although dermoscopy was widely used, training was viewed as too time-consuming (23). This hospital study also identified a similar trend in increased use of dermoscopy among younger physicians, as well as those in lower hierarchical positions (23). These trends in dermoscopy use were also observed in several US studies (24–26). A recent pan-European survey of registered dermatologists found that, although dermoscopy use across Europe was high (89% of participants), improved access to facilities in public healthcare settings and increased training during hospital residency would lead to further improvements in use for a range of skin diseases (27). Despite the widespread use of dermoscopy and availability of online training tools (http://www.dermoscopy-ids.org/index.php/education/podcasts) and training courses in France and elsewhere in Europe, these studies highlight the fact that interpretation of dermoscopy findings is complex and training methods and terminology may need to be updated to improve confidence among dermatologists. Although training is time-consuming and often difficult (23), improving expertise is essential, as dermoscopy has been shown to improve the accuracy of clinical diagnosis of melanoma, but only when conducted by experienced examiners (18–20, 28). For a trained dermatologist, a complete skin examination with dermoscopy increases the time spent on one patient by only 4 min (29). When the benefits of dermoscopy over naked-eye examinations are considered, this extra time appears worthwhile (29).
Epidemiological studies suggest that melanoma constitutes a family of tumours with different growth rates and propensities for metastasis (30, 31). Slow-growing melanomas are well-documented and require long-term follow-up for accurate diagnosis (30). However, rapidly evolving melanomas have also been reported (31). These lesions are generally large enough at diagnosis for metastasis to have already occurred, resulting in a poor prognosis. Studies aiming to correlate reflectance-mode confocal microscopy findings with histopathological and dermoscopy investigations of melanoma subtypes, together with new insights into melanoma development from stem cell-derived cancer models, suggest that some forms of rapidly growing melanoma arise from the dermis (32, 33). The deep location of these lesions and their generally symmetrical nature could render dermoscopy ineffective for the early diagnosis of these forms of melanoma. However, so far, the only form of melanoma that has been shown conclusively to occur in the dermis is melanoma arising in large congenital naevi. Interestingly, epidemiological studies show that, whilst the incidence of melanoma is increasing (2), mortality rates are stable (30, 31). This lack of a decline in mortality has led to the suggestion that early detection programmes do not reduce melanoma mortality (34–36). Results of a French national health institute (Institut de veille sanitaire (37)) study of the incidence and mortality of cancer from 1980 to 2012 suggest that this may be the case for male patients: out of all cancers studied, melanoma showed the second highest annual percentage increase in incidence in males over the time period studied and showed the ninth highest rate of mortality in 2012. It is now the leading cancer in terms of annual percentage increase in mortality in males in France. In contrast, this is not the case in females, indicating that women adhere better to the early detection programmes. Thus, the suggestion that early detection programmes do not reduce mortality is no longer true in most occidental countries, with success rates depending on numerous factors, including patient compliance.
The majority of deaths from facial or acral melanomas occur in patients with a long-term history of horizontal growth phase melanoma with recent evolution, rather than from aggressive fast-growing melanomas (LT; unpublished observation). In these cases, early detection offers interesting perspectives for reducing mortality. Al-though both under- and over-diagnosis have been reported for many cancers (38, 39), making an early diagnosis is highly important for patients with skin cancer. In addition, the benefits of dermoscopy outweigh the financial cost of performing the examination, with dermoscopy remaining a relatively low-cost method of cancer screening, with the cost in France estimated at 45.18 Euros per examination per patient (LT; unpublished observation).
Follow-up of patients in melanoma is essential for several reasons. Early diagnosis is the only way to reduce mortality from melanoma; however, accurate diagnosis can be problematic as early melanomas mimic naevi and systematic excision of all pigmented lesions is costly and inefficient. In addition, excision of all naevi is unfeasible in patients with numerous naevi, whilst these patients have a significantly higher risk of developing melanoma and require long-term surveillance.
Although dermoscopy significantly increases diagnostic accuracy among trained observers, the sensitivity of this method is not 100%. Like most cancers, melanoma changes over time. Addition of an E (for enlargement) criterion to the ABCD rule for dermoscopy has led to optimization of the sensitivity and specificity of dermoscopy diagnosis (40). Digital dermoscopy (DD) is particularly useful for the follow-up of lesions over time; comparisons of good quality images provide additional opportunities to make an accurate diagnosis of an initially featureless melanoma. The use of digital dermoscopy follow-up (DDFU) in daily practice has been shown to allow early detection of melanoma and to result in large reductions in the number of unnecessary excisions compared with use of dermoscopy alone (41). A comparison of melanomas diagnosed as part of a surveillance programme using DDFU and those diagnosed following referral to a melanoma unit revealed that the DDFU programme led to a large increase in the diagnosis of in situ melanomas and low-grade non-metastatic invasive melanomas (Table II) (42). The advantages of DDFU have been confirmed by meta-analyses, showing that follow-up by DD leads to increased detection of thin and in situ melanomas (43). Despite these advantages, the use of DD remains low in some countries, with only 8% of private practice dermatologists in France having access to a digital dermoscope (22).
Table II. Comparison of key characteristics of melanomas diagnosed with and without digital follow-up. From refs 41 and 42
The main indications for DDFU are a large number of naevi, a personal or familial history of melanoma, a predisposition to melanoma (i.e. patients with xeroderma pigmentosum) (44) and patients with lesions where excision would lead to disfiguring scars, (LT; unpublished observation). DDFU has been shown to be highly efficient when used in a targeted population of high-risk patients with familial atypical mole and multiple melanoma (FAMMM) syndrome, atypical mole syndrome (AMS) or a history of melanoma, but is not beneficial for patients with multiple naevi and no additional risk factors for melanoma (44). Only lesions showing signs of suspicion (slight asymmetry, thickening of the pigment network, signs of growth at the periphery, etc.) require monitoring for changes. Atypical Clark naevi require DDFU to assess for deviations from well-established dermoscopic patterns. If suspicious dermoscopic criteria are identified in one lesion, other lesions in the patient should be examined, as this will allow for a comparative approach to determining if these criteria are specific for melanoma in this individual case. DDFU is not indicated for lesions that are palpable, nodular or showing signs of regression. It is also not appropriate to initiate DDFU for lesions showing clear criteria of melanoma; in this case the lesions should be excised after the initial visit. Similarly, DDFU is not indicated for lesions showing clear characteristics of benign naevi (SP; unpublished observation). Successful follow-up requires compliance of the patients (45); if a patient does not adhere to the follow-up strategy the decision to not excise the lesion after the initial examination carries a greater risk of missing an early melanoma diagnosis.
Two strategies have been developed for DDFU. The first is the long-interval follow-up strategy, with follow-up examinations after 6–12 months (28, 45–48). Some of the changes viewed by dermoscopy at the follow-up examinations are significant and signal the presence of malignant melanoma, whilst others are non-significant (Table III). The second method is the short-interval follow-up strategy, with examination at 2–3 months (49). Using this second method, all changes occurring during the short-interval follow-up are considered as significant indicators of the presence of melanoma, with the exception of sun-induced colour changes and a change in the number of milia-like cysts (49). The most effective follow-up strategy is to combine the 2 methods, with an initial follow-up examination after 2–3 months and a second examination after 6–12 months. A major issue for follow-up strategies is the question of when to release patients from surveillance programmes, particularly as the majority of patients are concerned about the risk of developing melanoma and are therefore keen to continue with follow-up. Meta-analysis of DDFU studies revealed that the likelihood of detecting melanoma during follow-up increased with the length of the surveillance period, with each additional month of follow-up leading to detection of one additional melanoma (43). Thus, current evidence suggests that follow-up needs to be maintained throughout life in high-risk patients.
Table III. Significant and non-significant changes in lesions under surveillance with digital dermoscopy (DD) using the long-term follow-up strategy. From Kittler et al. 2000 (47)
The 2-step follow-up programme combining surveillance by total-body photography (TBP) and DD was established at the Early Diagnosis Unit of Cutaneous Melanoma, Hospital Clinic of Barcelona to monitor patients at high risk of developing malignant melanoma (50). In the early stages of the programme, a mean of 24 TBP images were required per patient, but improvements in camera resolution now mean that mapping with TBP can be completed with only 12 images per patient (SP; unpublished observation). Studies are ongoing to determine the optimal number of DD images required for patient follow-up; however, when this technique is used in combination with TBP the mean number of lesions monitored by DD is 18.44 per patient. The 2-step examination generally requires approximately 20 min, but can be much longer in patients with some conditions; for example more than 1 h in those with xeroderma pigmentosum. A combination of the short- and long-interval follow-up strategies is required for optimal surveillance, with examinations after approximately 3 months and then every 6–12 months.
When the 2-step strategy was applied to the follow-up of a targeted high-risk population (i.e. patients with atypical mole syndrome, a personal or familial history of melanoma, or a genetic predisposition to melanoma) this method was shown to allow early detection of melanoma with a low rate of excisions (44, 51). During the 10-year period since the start of the programme (1998–2008), patients were monitored for a mean of 96 months with a median of 10 visits per patient. Approximately 75% of included patients had between 50 and 200 naevi, and had familial or personal history of melanoma (29% and 44%, respectively). Over the study period, more than 11,000 lesions were monitored (18.44 lesions/patient) but only 1,152 lesions required excision (1.86 lesions/patient). Of the excised lesions, 8.5% were melanoma (51). The majority of the excised lesions (70%) were selected because of changes visible by DD, whilst the remaining 30% were excised as a result of changes observed by TBP (51).
No differences in melanoma subtype or Breslow thickness were found between melanomas identified by DD and those identified by TBP (52), confirming that TBP can be used as an alternative tool to detect in situ and thin melanomas. Focal changes in pigmentation and structure were the most commonly detected dermoscopic changes occurring in malignant melanomas, whilst no significant differences in asymmetrical enlargement, regression and changes in pigmentation were found between lesions that were confirmed as melanoma and those that were naevi (52). In this study 53 lesions were excised that showed symmetrical enlargement. Although symmetrical growth would be considered as non-significant in long-interval DDFU, histological analysis revealed that one of these lesions was melanoma with a Breslow thickness of 0.5 mm in an elderly patient. This finding highlights the need for excision to be considered for all atypical lesions with substantial changes in high-risk patients and that the age of the patient also needs to be taken into consideration (52).
Many slow-growing melanomas were detected by the 2-step surveillance programme, 50% of the melanomas excised required more than 2 years of follow-up to identify the changes, and 75% of these melanomas were still in the in situ phase when removed (52). Further analysis of this melanoma subgroup has revealed characteristics such as a reticular pattern, asymmetry and some focal hyperpigmentation (30). Thus, long-term follow-up is essential to rule out melanoma, particularly as in some cases these slow-growing lesions have been found to transform over time into fast-growing, life-threatening thick melanomas (SP; unpublished observation). Al-though compliance with the 2-step follow-up system is good, with 84.1% of patients continuing surveillance after 10 years, a mortality rate of 2.2% was observed during the study period, mainly (85% of cases) as a result of a previous melanoma developed before inclusion in the programme (51). This observation again highlights the fact that patients with multiple melanomas are still at risk of dying from a previous malignant melanoma despite regular follow-up.
Over the 10-year period, new melanomas were diagnosed in 12.6% of patients studied, with the likelihood of developing a new melanoma during follow-up increasing significantly for patients with a personal history of melanoma (Fig. 2) (51). Thus, patients with multiple primary melanomas need specific follow-up because they have a high probability of developing new melanomas during the surveillance period. Age is often considered an important factor in the likelihood of developing melanoma. As expected, the efficiency of the 2-step method was highest in elderly patients. The number of lesions showing changes is typically much lower in patients over 60 years of age than in younger patients, where many lesions show changes requiring excision. As a result, the ratio of benign to malignant melanoma in patients > 60 years was 1:7.2, whereas it was 1:18.5 in patients < 20 years (SP; unpublished observation). However, these results show that the 2-step method is beneficial in the follow-up of young high-risk patients and can be used to detect melanoma in patients where many lesions undergo changes (51).
Fig. 2. Diagnosis of a new melanoma during follow-up. NPM: new primary melanoma, PM: primary melanoma. From Salerni et al., 2012 (51).
The 2-step follow-up method has also been used for surveillance of high-risk patients in Australia (53). Monitoring of patients with TBP and DD over a 5-year period in this Australian population was also found to lead to earlier detection of melanomas, with 38% being detected by TBP and 39% by DD. The risk of developing a new melanoma during the surveillance period appeared to be high in this population, with 12.7% of patients developing a new melanoma during the first 2 years of follow-up compared with approximately 12.6% over 10 years in the Spanish high-risk population (51, 53). The benefits of TBP as an additional detection method were highlighted in the Australian study by the identification of thick melanomas, 5 of which were desmoplastic melanomas. Although dermoscopic characteristics have been defined for desmoplastic melanomas (54), these types of melanoma require a clinical examination and cannot be diagnosed by dermoscopy alone. However, the appearance over time of these lesions on the TBP map of high-risk patients was a sufficient indicator for further investigation of the lesion and diagnosis of thick melanoma using the 2-step method (53).
Another subgroup of patients at high risk of developing advanced melanoma, despite participating in DDFU programmes, are patients carrying mutations in the MITF gene. These patients often have over 200 naevi and are susceptible to developing fast-growing nodular melanomas, which can grow to a thickness of 1 mm within 2 months (55). Early diagnosis of melanomas in these patients relies on patient education, with patients performing regular examinations of the skin and reporting any new lesions persisting for more than 2 weeks for further investigation.
The most important perspective in the use of dermoscopy for the diagnosis of skin cancer is telemedicine. This relatively new approach to skin cancer diagnosis is discussed in further detail by Moreno-Ramírez & Argenziano (56). Telemedicine helps to diagnose difficult cases by providing remote access to expert dermatologists and avoids the unnecessary time and costs associated with patients travelling long distances to attend specialized clinics. More advanced imaging techniques, such as reflectance confocal microscopy (57), are also now being applied to the diagnosis of skin cancer. Use of reflectance confocal microscopy has already been shown to improve the accuracy of melanoma diagnosis in equivocal lesions detected through DDFU programmes and to reduce the number of unnecessary excisions (58–60). Alternative methods, such as the use of sniffer dogs in melanoma clinics, have also been described (61, 62).
Transfer of expertise to general practitioners (GPs) is another important perspective in the field of melanoma diagnosis, particularly as the number of practicing dermatologists continues to fall in many countries. Although use of dermoscopy with a simplified 3-point checklist has been validated as a tool for melanoma diagnosis by non-experts (63), few countries in Europe currently provide training on the basic principles of dermoscopy to GPs. In contrast, in Australia, the majority of research in the field of dermoscopy is conducted by GPs rather than dermatologists, for example the work of Dr A. Cameron (School of Medicine, University of Queensland, Brisbane, Australia) and S. Menzies (Sydney Melanoma Diagnostic Centre, The University of Sydney, Australia).
Dermoscopy has proven its efficiency in the differential diagnosis of pigmented tumours of the skin. However, the many exceptions in the dermoscopic analysis of skin lesions are a source of complexity and may reduce compliance among trainees, leading to the suggestion that teaching methods need to be re-evaluated. When performed by trained users on compliant patients, DDFU further increases the diagnostic accuracy of dermoscopy. Training is therefore of tremendous importance, both for dermatologists and GPs. In targeted populations with a high risk of developing melanoma, the combined use of TBP and DD (2-step method of digital follow-up) allows the detection of melanomas at early stages and significantly reduces the number of excisions. Long-term follow-up is required in these high-risk populations to allow the detection of slow-growing melanomas. Telemedicine already is, and will be, an important link between clinicians and experts. Finally, although the benefits of dermoscopy in the early diagnosis of melanoma have been confirmed in many studies, the public health impact of dermoscopy requires further study.
Emma Pilling and Marielle Romet (Santé Active Edition) provided medical writing assistance funded by Pierre Fabre Dermocosme-tique.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize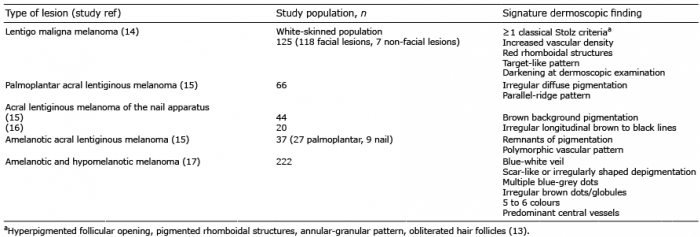 Click to show fullsize
Click to show fullsize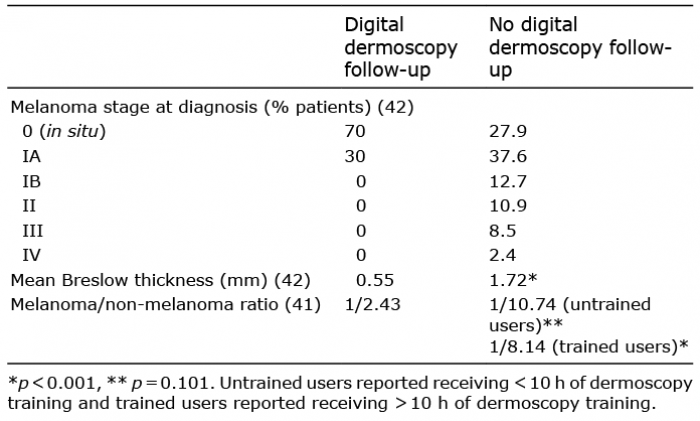 Click to show fullsize
Click to show fullsize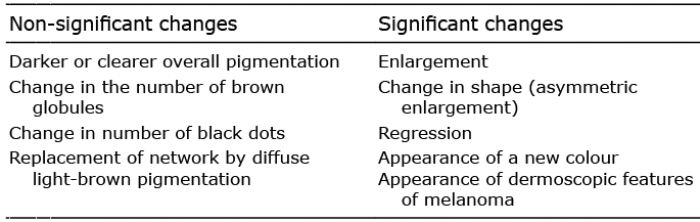 Click to show fullsize
Click to show fullsize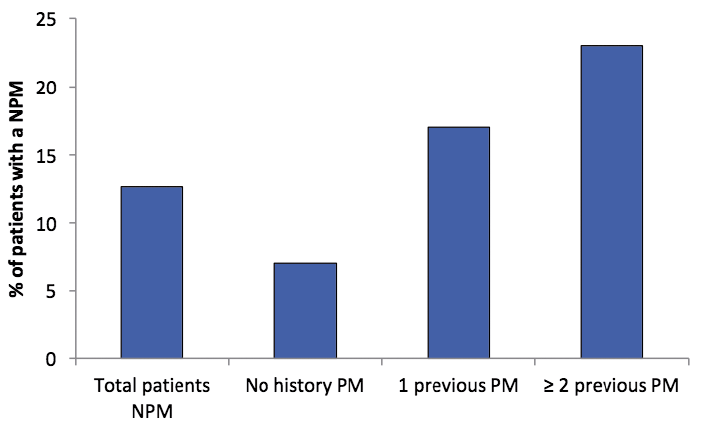 Click to show fullsize
Click to show fullsize