


1Department of Dermatology, Rambam Health Care Campus, 2Biobank and Unit of Epidemiology, Rambam Health Care Campus, School of Public Health, Faculty of Social Welfare and Health Sciences, University of Haifa, and 3Rappaport Faculty of Medicine, Technion-Israel Institute of Technology, Haifa, Israel
There is little consensus regarding mortality data in bullous pemphigoid (BP). The aim of this study was to evaluate mortality among a relatively large cohort of Israeli patients with BP and to perform a meta-analysis synthesizing existing data on 1-year mortality rates of patients with BP. This retrospective cohort study of 287 patients diagnosed with BP between 2000 and 2015 compared the mortality of patients with BP with age- and sex-matched control subjects in the general population. The results showed 1-, 5- and 10-year mortality rates of 26.9%, 56.9% and 69.5%, respectively, and a 3.4-fold higher risk of death. A systematic review and meta-analysis were then performed using a random effects model. Including the current study, 25 studies comprising 4,594 patients met the eligibility criteria. The pooled estimate of 1-year mortality rate was 23.5% (95% confidence interval 20.2–26.8; I2=81%; p < 0.001). The pooled 1-year mortality rate of European cohorts was prominently higher relative to the pooled rates of cohorts from the USA and Asia.
Key words: bullous pemphigoid; mortality; survival; prognosis; meta-analysis; systematic review.
Accepted Mar 27, 2018; Epub ahead of print Mar 27, 2018
Acta Derm Venereol 2018; XX: XX–XX
Corr: Khalaf Kridin, Department of Dermatology, Rambam Health Care Campus, POB 9602, Haifa 31096, Israel. E-mail: dr_kridin@hotmail.com
Mortality data in BP are highly inconsistent. By this retrospective cohort study, a 3.4-fold increased mortality and 27% 1-year mortality rate were recognized among Israeli patients with BP. Performing a systematic review and meta-analysis led to the conclusion that the pooled estimate of 1-year mortality rate in BP patients is 23.5% worldwide. The stratified pooled estimate is higher in European cohorts as compared to American and Asian ones. These data allow patients to be aware of prognosis and to make informed decisions, and provide clinicians with an indicator of the success of treatment.
Bullous pemphigoid (BP) is the most common type of autoimmune blistering diseases (1). It is characterized by the presence of circulating IgG autoantibodies to BP180 and BP230, which are components of junctional adhesion complexes called hemidesmosomes that promote dermoepidermal cohesion (1, 2). BP180 autoantibodies have been demonstrated to be directly pathogenic by triggering an inflammatory cascade that leads to tissue damage and, ultimately, to subepidermal blister formation (3, 4). The disease is characterized by severe pruritus, tense bullae and urticarial plaques, and usually occurs in elderly patients (5).
BP has a chronic relapsing evolution, with spontaneous exacerbations and remissions (6). It is associated with a high rate of fatality, with 1-year mortality rates ranging from 6% to 41% (7, 8). The mortality of patients with BP is estimated to be 2–7-fold higher than age- and sex-matched controls. The calculated mortality rates vary significantly from region to region, and particularly between cohorts originating from Europe and the USA. Studies regarding the prognosis of BP in the Middle-East are lacking.
The objective of this study was to determine the overall mortality of patients with BP relative to an age- and sex-matched population in Israel, tracking a relatively large immunopathologically validated cohort. Due to the controversies concerning the mortality rates of BP, a systematic review and meta-analysis of published data were performed with the aim of providing an accurate overview of true mortality in patients with BP.
Study population and inclusion criteria. This population-based retrospective cohort study comprised all consecutive patients who received a new diagnosis of BP between 1 January 2000 and 31 December 2015, in Rambam Health Care Campus, Haifa, Israel.
BP was diagnosed as a blistering disease of the skin with suggestive clinical features (9), in conjunction with typical histopa-thology, i.e. a subepidermal blister with an inflammatory infiltrate usually containing eosinophils in the superficial dermis, alongside at least one of the following immunopathological features: (i) linear deposits of IgG and/or C3 along the basement membrane zone by direct immunofluorescence (IF); (ii) circulating IgG autoantibodies binding to the basement membrane, as demonstrated by the use of monkey esophagus, and a standard indirect IF technique; (iii) the presence of circulating IgG antibodies against BP180 using enzyme-linked immunosorbent assay (ELISA) (10).
Outcomes. Survival status and date of death among patients with BP were ascertained by linking the study cohort with the National Registry of Deaths Database of Haifa district. All patients were followed-up from the onset of BP until 31 December 2016, exiting the study earlier if they died during the observation period. The ethnicity of the study participants was defined in accordance with the formal registration of the Ministry of Interior; the computerized database of our institution is cross-linked with that of the Ministry of Interior, enabling the extraction of demographic characteristics of patients. The study had approval from the institutional ethics committee of our medical centre.
Statistical analysis. The observed survival curve from the onset BP was estimated using the Kaplan–Meier method. The expected survival curve of the study cohort was computed according to Hakulinen’s method (11), using sex-, age- (1-year classes), and calendar year-specific (1-year classes) mortality rates for the population of Israel (Israel Central Bureau of Statistics). To compare the observed and expected survival rates, we calculated standardized mortality ratios (SMRs), the ratio of the observed to the expected number of deaths, with 95% Poisson confidence intervals (CI). The expected number of deaths was calculated by multiplying person-years of each sex-, age (1-year classes)-, and calendar-year-specific stratum of the study cohort by the corresponding mortality rate of the population of Israel, and then summed across all strata. All analyses were performed using STATA statistical software version 8.2 (StataCorp, College Station, TX, USA).
Search strategy. The literature for this review was comprehensively searched using PubMed, Embase and Cochrane Library to identify eligible studies. Publications up to March 2017 were searched independently and crosschecked by 2 researchers. The keywords used in this search consisted of “bullous pemphigoid” or “pemphigoid” combined with “mortality”. A comprehensive search of reference lists of all the review articles and original studies retrieved by this method was performed to identify additional reports.
The inclusion criteria were peer-reviewed full-length original articles related to the search terms and indexed in the database above. Reviews, single case reports, and articles not related to both BP and mortality were excluded. Studies were excluded if they reported mortality data only as part of trials for a drug, or when the 1-year mortality rate was not reported explicitly. When 2 papers reviewed mortality of the same cohort at different times, the later publication was used.
Statistical analysis. The overall pooled estimate and 95% CI of 1-year mortality were obtained using either a fixed or random effects meta-analysis model as appropriate, depending on a test for heterogeneity using a 10% significance level (12). χ2 heterogeneity tests were used to test for gross statistical heterogeneity across studies (13). Heterogeneity was additionally explored in a subgroup analysis for the region and the settings of the study. If heterogeneity was significant, a random effects model was used to synthesize effect size. All analyses were performed using STATA statistical software version 8.2 (StataCorp).
The study cohort comprised 287 patients with BP, including 119 (41.5%) men and 168 (58.5%) women. Mean age at diagnosis was 77.6 ± 12.1 years (range 22–99; median 80 years). No significant difference was observed in the age of presentation between males and females (77.8 ± 12.8 vs. 77.5 ± 11.5 years, respectively, p = 0.840), whereas Arabs were significantly younger than Jews (69.5 ± 15.3 vs. 78.7 ± 11.1 years, respectively, p = 0.002). The majority of patients were of Ashkenazi Jewish origin (n = 175, 61.0%), followed by Sephardic Jews (n = 79, 27.5%) and Arabs (n = 33, 11.5%). The diagnostic methods utilized for establishing the diagnosis of BP in these patients are fully elucidated in another study performed by our group (14).
Overall, 287 patients were followed, contributing 1,107.9 person-years. The mean length of follow-up was 4.0 ± 4.1 years (median 2.3 years). Median duration of follow-up for those alive at the end of the analysis was 4.9 years (range 0.2–15.9 years).
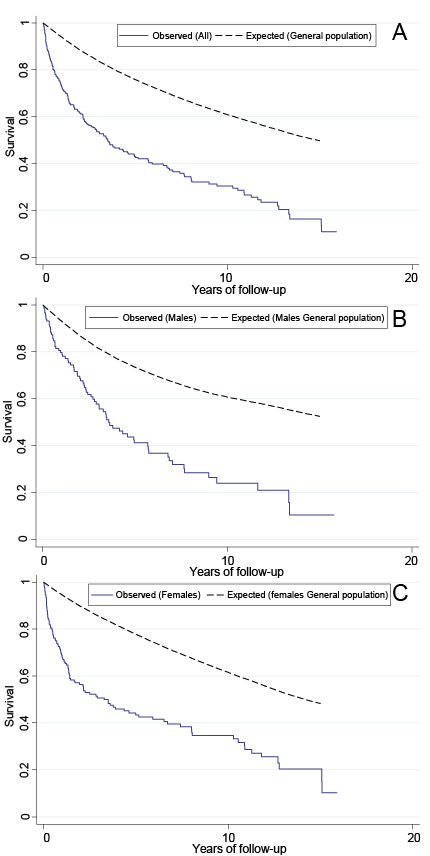
In all, 181 (63.1%) patients died during the study period, both in the inpatient and outpatient settings, of whom 74 (40.9%) were men, and 107 (59.1%) were women. The 1-, 3-, 5-, 7-, and 10-year overall survival rates were 73.1%, 53.6%, 43.1%, 37.3% and 30.5%, respectively.
Kaplan–Meier survival curves for the BP cohort were lower than expected in the age-matched general populations, in both sexes throughout the whole duration of follow-up (Fig. 1). Relative to the expected age- and sex-specific overall death rates in the general population in Israel, there was more than 3-fold excess of mortality among patients with BP, with an SMR of 3.4 (95% CI 2.9–3.9). In the sex-specific analysis, the SMRs for patients with BP were significantly higher for both men (SMR 3.0; 95% CI 2.4–3.8) and women (SMR 3.7; 95% CI 3.1–4.5). In the ethnicity-specific analysis, the risk of death was increased in both of the major ethnic populations in Israel. However, the SMR of Arab patients with BP (SMR 6.9; 95% CI 4.4–10.8) was prominently higher than that of Jewish patients with BP (SMR 3.1; 95% CI 2.7–3.7).
Fig. 1. (A) Survival among all patients diagnosed with bullous pemphigoid (BP) throughout 2000 to 2015 compared with expected survival. (B and C) Survival stratified by sex.
Table I presents the results of calculated SMRs further stratified by sex and age group at diagnosis. Most of the deaths and the highest mortality rates (246.5 and 269.1/1,000 person-years for men and women, respectively) were observed amongst patients with BP onset at 75 years and older. Nonetheless, when compared with the expected deaths in the general population, the highest SMRs were found in patients whose BP onset was younger than 65 years of age, with a value of 6.8 (95% CI 3.1–15.3) for men and 6.3 (95% CI 2.6–15.0) for women.
Table I. Observed and expected deaths and standard mortality ratios in patients with bullous pemphigoid stratified by sex and age at diagnosis
An initial 473 papers published before March 2017 were identified. After the critical screening of titles, abstracts, and full text, 24 studies suitable for analysis were selected (Fig. 2). Our current retrospective cohort study met the eligibility criteria and was therefore included in the quantitative synthesis. The 25 eligible studies comprised 4,594 patients with BP. The mean age of patients with BP in the different study cohorts ranged between 64 (15) and 83 (16) years, and their 1-year mortality rates ranged between 6% (7) and 41% (8) (Table II).
Fig. 2. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement flow diagram summarizing trial identification and selection. The current study is included in the meta-analysis.
Table II. Mortality data of patients with bullous pemphigoid (BP) from previously published studies divided by continent: review of the literature
The overall random-effects pooled 1-year mortality rate was 23.5% (95% CI 20.2–26.8) with a high level of heterogeneity (I2 = 81%; p < 0.001). In order to examine potential sources of heterogeneity, estimates were pooled according to geography; studies from Europe reported higher 1-year mortality rates (26.7%; 95% CI 22.2–31.2; I2 = 87%; p < 0.001) compared with studies from the USA (15.1%; 95% CI 7.9–22.3; I2 = 71%; p < 0.001) and Asia (20.5%; 95% CI 13.8–27.3; I2 = 81%; p < 0.001). A stratified analysis was performed separating studies according to their settings. No significant difference was observed between the pooled estimate of population-based and nationwide studies (22.2%; 95% CI 17.0–28.4; I2 = 79.4%; p < 0.001) and that of monocentre and multicentre studies (24.3%; 95% CI 20.9–28.0; I2 = 80.4%; p < 0.001).
This population-based study is a primary study of mortality in patients with BP in a Middle Eastern population. Interestingly, the 1-year mortality rate in the study cohort (26.9%) is in line with the combined estimate calculated for European studies (26.7%). Similar to the European populations with unconstrained access to modern health services, Israeli citizens have a universal healthcare system with mandatory participation in a medical insurance plan. Thus, the current study is less susceptible to selection bias that may arise from the inclusion of healthier patients with better access to health insurance coverage.
Age- and sex-adjusted mortality was higher in patients with BP compared with the general population. The SMR for all age groups was higher than 1, indicating that the rate of observed deaths was greater than that expected in the general population. The SMR was highest for patients younger than 65 years at presentation because the background mortality in this age group in the general population is low. Thus, mortality can more easily be attributed to BP and its associated comorbidities in younger patients. Interestingly, the SMR of Arab patients was more than twice as high as the SMR of Jewish patents (6.9 vs. 3.1, respectively). Similarly, this substantial increase in mortality is most likely attributable to the younger age of Arab patients relative to their Jewish counterparts (69.5 vs. 78.7 years, respectively; p = 0.002).
Concerning strengths and limitations of the current study, a relatively large cohort of patients with immunopathologically-verified BP was tracked for an extended duration of time. The representative nature of our cohort lowered the susceptibility to selection bias. In addition, the status of death/survival was known for each patient at the end of the study period, without any attrition or loss to follow-up. This further reinforces the validity of our findings. However, our study is limited by its retrospective nature and the fact that it was based at a single institution.
A substantial controversy surrounds the mortality and survival rates of patients with BP. Although the survival status is a clear-cut measure, current literature varies so much in its results. Combination of the results of various studies in a meta-analysis increases statistical power and provides sufficient information to show the accurate mortality rates reliably. To the best of our knowledge, this is the first meta-analysis summarizing the mortality data of patients with BP.
This meta-analysis yielded a combined estimate of 23.5% mortality rate in the first year following the diagnosis of BP. In subgroup analysis differentiating studies according to the continent they were performed in, the pooled estimate for 1-year mortality rates was prominently higher in studies originating from Europe (26.7%) compared with studies from Asia (20.5%), and the USA (15.1%).
Several possibilities were offered to interpret the differences between the findings observed in Europe and the USA. The therapeutic approach of treating patients with BP is different, in that the majority of patients reported from Europe are hospitalized for treatment, whereas hospitalization for BP is the exception in the USA (17). Death due to sepsis, which is more frequent in hospitalized elderly patients, had been proposed as a cause of the increased mortality in Europe (18). This suspicion was refuted by a Spanish study, in which only 2 of 11 patients died from sepsis within the follow-up period, and neither death was within 6 weeks of initial hospitalization (19).
Age variations also do not seem to provide a reasonable explanation for the higher mortality reported in Europe, as the mean age of patients in 2 European (19, 20) and 1 American (18) study was identical (77 years). Nonetheless, mortality was still 3–4 times higher in the European studies. Ethnic differences as the cause of higher mortality in Europe is also unlikely, as the studies conducted in European countries (England, France, Germany, Scotland, Switzerland, Spain, Poland, and Finland) and the USA (Boston, Cincinnati/Detroit, New York, Milwaukee, Georgia, Ohio, and Minnesota) spanned a wide range of nationalities and ethnicities (Table II).
The most likely explanation is that studies from the USA may be biased due to the inclusion of patients with a better condition of general health and/or higher access to medical care related to health insurance coverage (17). This may be because patients in the USA with more severe disease or comorbidities are not treated in tertiary medical centres (21) or, conversely, because such patients in Europe are preferentially referred to tertiary centres. Thus, mortality rates would appear higher in Europe than in the USA because it is based on a subset of BP patients with more comorbidities. Given that the majority of the reports were hospital-based, this bias may explain the discrepancy observed between these studies.
Four recent retrospective studies originating from Eastern Asia had demonstrated 1-year mortality rates ranging from 12.9% to 26.7% (15, 22–24), with a combined estimate of 20.5%. This is lower than that of Europe. Both Li et al. (15) and Lee & Kim (23) had attributed their lower mortality rates to the substantially younger mean age of their Asian patients relative to European patients. Unlike studies from the USA, the lower mortality rates in these cohorts were not attributed to selection bias (15, 23).
It is noteworthy that a meta-regression model did not reveal notable differences between nationwide and hospital-based studies in the pooled 1-year mortality rates.
The main limitation of the meta-analysis lies in pooling studies with different inclusion/exclusion criteria, sample sizes, sampling approaches, and regions. The high level of heterogeneity among eligible studies and the limited number of high-quality prospective studies may also interfere with the validity of the findings of the current meta-analysis.
In conclusion, this first meta-analysis of mortality rates in patients with BP demonstrates that the combined estimate for 1-year mortality is as high as 23.5% (95% CI 20.2–26.8%). The findings of our retrospective cohort study indicate that the risk of all-cause mortality among Israeli patients with BP is 3 times greater than expected for the general population, with a 27% probability of death within the first year following the diagnosis. These observations align with the subgroup estimate of the European studies.
The authors would like to thank Mrs Wesal Shihade for her substantial assistance in performing the retrospective cohort study. Mrs Shihade had full access to all of the data in the study and took part in designing the study and performing data analysis.
The authors have no conflicts of interests to declare.


 Click to show fullsize
Click to show fullsize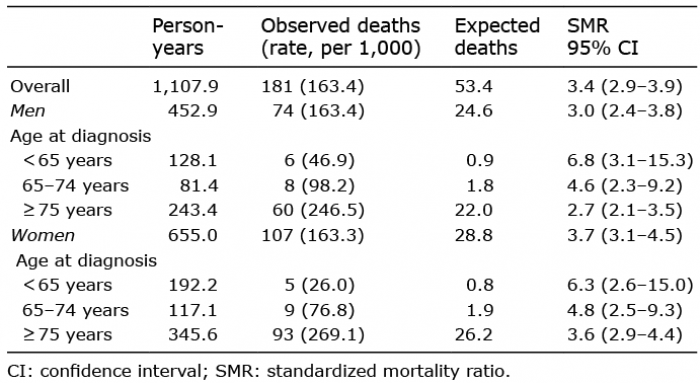 Click to show fullsize
Click to show fullsize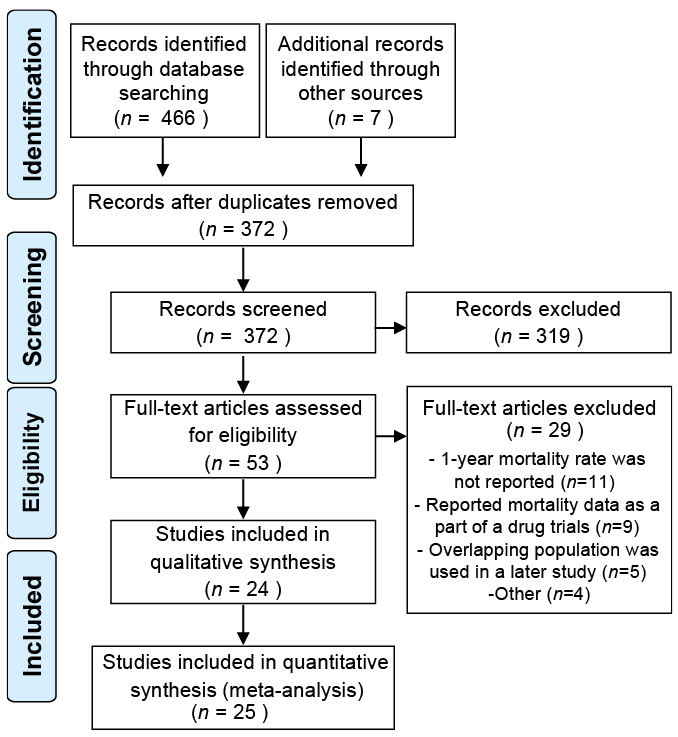 Click to show fullsize
Click to show fullsize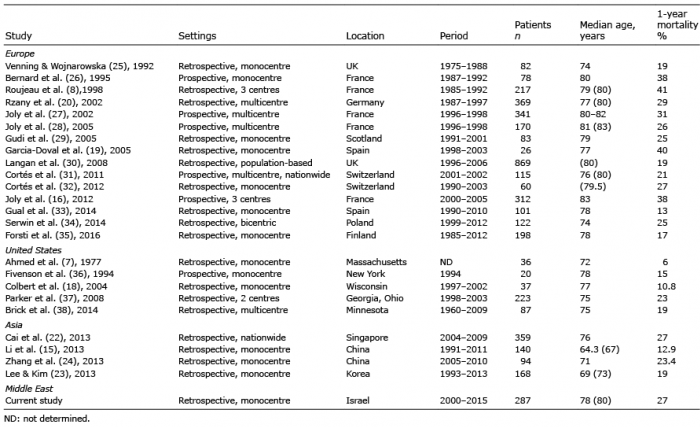 Click to show fullsize
Click to show fullsize