


1Department of Dermatology and Skin Science, University of British Columbia, Vancouver, Canada, 2Department of Dermatology, College of Physicians and Surgeons, Columbia University, New York, USA, 3Department of Dermatology and Skin Science, Vancouver General Hospital, Vancouver, BC, Canada, 4Hospital Universitário de Taubaté Dermatologia, Universidade de Taubaté, Taubaté, Brazil, 5The Ronald O. Perelman Department of Dermatology, New York University School of Medicine, New York, USA and 6Centre for Skin Sciences, University of Bradford, Bradford, UK
The development of androgenetic alopecia is associated with a risk of developing cardiovascular diseases, but the association of alopecia areata with cardiovascular diseases in humans is largely unexplored. We measured the plasma level of two common cardiovascular disease markers, cardiac troponin I and C-reactive protein, in alopecia areata and androgenetic alopecia-affected subjects. Also, we investigated the possible presence of pro-apoptotic factors in the plasma of hair loss subjects. The mean plasma cardiac troponin I level was highest in alopecia areata subjects, moderately higher in androgenetic alopecia subjects, and lowest in subjects without hair loss (p < 0.05). Alopecia areata subjects not receiving treatments had highest levels of cardiac troponin I (p < 0.05). Alopecia areata plasma samples with high cardiac troponin I levels also induced significantly higher rates of cardiomyocyte apoptosis in cell culture assays. The results suggest the potential for increased heart remodelling. Close monitoring of cardiovascular health in alopecia areata subjects, as well as subsets of androgenetic alopecia patients, may be appropriate.
Key words: alopecia areata; androgenetic alopecia; autoimmune disease; cardiac troponin I; C-reactive protein; heart remodelling; cardiovascular disease; hair loss.
Accepted Apr 11, 2018; Epub ahead of print May 8, 2018
Acta Derm Venereol
Corr: Kevin J. McElwee. Centre for Skin Sciences, University of Bradford, Bradford, West Yorkshire, BD7 1DP, UK. E-mail: kmcelwee@mail.ubc.ca
Alopecia areata (AA) is a form of inflammatory autoimmune disease targeting hair follicles. While AA is not directly a life-threatening disease, recent studies in humans and mice suggest a potential correlation with higher risk of heart disease and stroke. We found increased levels of cardiac troponin I in blood plasma from patients with AA. Elevated levels of this factor can indicate increased heart tissue damage. The data suggest that the development of AA may involve more systemic and debilitating effects beyond the skin. A more comprehensive evaluation of AA patients’ heart health is warranted.
The association of androgenetic alopecia (AGA) with cardiovascular diseases (CVDs) has been explored by several research groups (1–6). However, the potential for links between CVD and most other forms of hair loss has not been actively investigated. Alopecia areata (AA) is an inflammatory, cell-mediated autoimmune hair loss disease that can be associated with other inflammatory and autoimmune diseases such as thyroiditis (7), and psoriasis (8). We previously identified a higher level of cardiac troponin I (cTnI) in C3H/HeJ mice affected by AA (9), possibly as a result of chronic inflammation in the skin and hair follicles. While the exact form of cardiac anomaly was not identified, AA affected mice presented with significantly larger heart mass.
Chronic inflammatory conditions and autoimmune diseases, such as psoriasis, rheumatoid arthritis (RA), and systemic lupus erythematosus (SLE), are associated with significantly higher risks of CVDs (10–12). Recent advances in AA research have revealed disease pathways that are shared between other forms of autoimmune disease including psoriasis, SLE, and RA (13). As such, AA patients may also share similar risks for other conditions. While many affected by RA experience asymptomatic, subclinical cardiac involvement, coronary artery disease is one of the most common causes of death in RA patients (14). It has been suggested that aggressive management of inflammation in these patients can reduce the risk for CVDs. Potentially, the inflammatory response in AA may also affect cardiovascular health following similar pathways or mechanisms as seen in RA.
Releasable molecules such as C-reactive protein (CRP) and cTnI have been widely used as biomarkers of cardiac infarction and heart failure (15 16). CRP is a strong predictor of new heart failure, myocardial infarction, stroke, cardiovascular cell death and also for new onset of diabetes (16). CRP has also been used as a prognostic marker for patients already diagnosed with RA and decreased levels of CRP have been used as an indication that a drug has beneficial effect (17). Significant elevation of CRP has previously been identified in males with AGA (18 19). Since CRP is a mediator of inflammation as well as an indicator of immune response, its altered expression might also play an active role in the progression of AA.
Myocardium expresses cTnI which plays an important role in regulating the calcium mediated interaction between actin and myosin (20). The plasma level of cTnI is greatly increased following myocardial infarction due to cardiac cell death and tissue restructuring, making it an important marker of cardiomyocyte injury (15). However, it can also be elevated in advance of ischemia in patients who subsequently suffer heart failure (16). It has been shown that cTnI level is elevated in RA patients even without the presence of heart failure; indicating subclinical myocardial injury (21). In general, subjects with common subclinical CVDs usually have greater than 0.01 µg/ml of plasma cTnI (22).
In this study, we investigated the plasma levels of cTnI and CRP in patients with AA and AGA compared to individuals with no hair loss (NHL). Subsequently, we examined the potential for blood plasma from AA and AGA patients to have an adverse effect on cultured cardiomyocytes.
AA-affected, AGA-affected, and control subjects with NHL were recruited with informed consent from the Skin Care Centre, and Clinical Research Unit, at Vancouver General Hospital according to University of British Columbia Clinical Research Ethics Board approved protocols. A questionnaire incorporating National Alopecia Areata Foundation guidelines (23) was completed at the time of blood collection by the interviewing doctor/nurse for each study participant regarding their hair loss and background information. The extent of hair loss in male AGA affected subjects was classified using the Norwood scale, while female AGA subjects were classified using the Ludwig scale. None of the study subjects had CVDs based on their known medical background. Plasma was isolated from whole blood (20 ml) and frozen at –80 °C until use. A total of 89 AA subjects, 72 AGA subjects, and 34 subjects with NHL before matching for age and sex, were included in the study (Table SI).
AA subjects ranged from those with less than 25%, patchy hair loss to subjects with alopecia totalis (AT) and/or alopecia universalis (AU). Non-AA subjects were screened to exclude those with inflammatory hair loss such as cicatricial alopecia and comprised individuals with either NHL or androgenetic alopecia (AGA). Sex-matching was performed by separating the sexes into individual groups for AA, AGA and NHL. Age matching was performed by grouping age groups into 18–35 years, 36–50 years and > 51 years.
Human cTn I (Calbiotech, Spring Valley, CA) and Human C-Reactive Protein (eBioscience, San Diego, CA) standard sandwich ELISA assays were used to measure plasma levels of cTnI and CRP in the study subjects. Average absorbance optical density (OD) of the samples was measured by a spectrophotometer, a higher concentration of cTnI or CRP would absorb more light, resulting in higher OD. Statistical significance was calculated by one-way ANOVA with multiple comparisons using GraphPad Prism software (La Jolla, CA). Comparisons between two groups were performed with Student’s t-test.
Primary HCMs (Applied Biological Materials Inc, Richmond, BC) were cultured in T25 BioCoat Collagen I Coated Vented Flasks (BD Bioscience, Mississauga, ON) at 200,000 cells/ml in PriGrow I medium (ABM Inc) supplemented with 10% FBS and 100 μg/ml Streptomycin with 100 U/ml Penicillin (Invitrogen, Grand Island, NY). Half of the culture medium was removed every 3 days and replenished with fresh complete medium. HCMs were subcultured into 24-well BioCoat Collagen I Coated Plates (BD Bioscience) at 60,000 cells/500 µl and rested for 2 days before switching to PriGrow medium supplemented with human plasma.
Separate cultures with PriGrow medium were supplemented with 10% plasma from 3 different AA or AGA subjects identified with the highest levels of plasma cTnI, 3 AA or AGA subjects with lowest plasma cTnI, and 3 NHL subjects. The cultures with human plasma were maintained for 10 days with fresh media replenished every 2 days. The positive controls for apoptosis were wells with PriGrow media without any serum and RPMI 1640 (Invitrogen) without any serum. The negative controls received FBS-supplemented PriGrow media as above. At the end of 10 days, the HCMs were collected after trypsinization for flow cytometry.
HCMs were labelled with Annexin V (eBioscience, San Diego, CA), and Propidium Iodide (PI) (eBioscience) was added into the cell suspensions 15 min before flow cytometry analysis. Flow cytometry analysis was performed on a BD FACSCanto II flow cytometer (BD Bioscience). Statistical significance was calculated by one-way ANOVA with multiple comparison followed by Fisher’s Least Significant Difference test using GraphPad Prism software.
We performed a multiplex screening of cytokines in the plasma samples used in the apoptosis assay. A Cytokine Human 25-Plex Panel for Luminex (Invitrogen) was performed following manufacturer’s protocols. The plasma cytokine profiles were determined by the manufacturer as part of the service. Comparison of cytokine expression profiles was expressed as a heat map generated by GENE-E (Broad Institute, Cambridge, MA, USA).
Age and sex-matched AA male and female subjects showed significantly higher plasma levels of cTnI (Fig 1a, b) compared to controls (AGA and NHL subjects). Comparison of CRP levels showed similar trends (Fig 1c, d), but statistical significance was not achieved.
Fig. 1. Alopecia areata (AA) and androgenetic alopecia (AGA). AA subject plasma samples had significantly higher levels of cardiac troponin I (cTnI) compared to the control group. Both male and female AA subjects had significantly higher levels of cTnI compared to the control group (a, b). The plasma levels of C-reactive protein (CRP) showed similar trend, but statistical significance was not achieved. The comparison was performed using age and sex-matched subgroups. Statistical significance was determined with Student’s t-test, *denotes p < 0.05.
Without correcting for sex and age, males with AA exhibited significantly higher levels of cTnI compared to NHL and AGA males (Fig. 2a). Higher levels of cTnI were also observed in younger age groups (18–35) for both AA and AGA (Fig. 2c). Conversely, the levels of CRP showed an overall higher trend in all female groups compared to males (Fig. 2b). AA and AGA subjects in older age groups revealed higher CRP levels and significance was observed in AGA subjects over 50 years old (Fig. 2d).
Fig. 2. Alopecia areata (AA) and androgenetic alopecia (AGA). The level of cardiac troponin I (cTnI) was higher in males with AA and younger age groups while C-reactive protein (CRP) was higher in females and older age groups. AA affected males had significantly higher levels of cTnI compared to males in other subject groups, but not with females within the same group (a). The level of CRP was higher in females from all subject groups, and was higher in AA and AGA groups (b). In both AA and AGA groups, the level of cTnI was highest in those who were between the age of 18 and 35, but statistical significance was only observed in AGA subjects (c). CRP levels did not show a consistent trend for AA subjects, but increased linearly as age increased in AGA patients (d). Statistical significance was determined with one-way ANOVA where * denotes p < 0.05.
AGA subjects who were receiving treatments (finasteride and/or minoxidil) showed no difference in plasma cTnI levels compared to the no treatment AGA group (Fig. 3a). AA subjects who were receiving treatment had higher levels of CRP compared to non-treated AA subjects, but the difference was not significant. AGA subjects also showed no difference in CRP levels regardless of receiving treatment or not (Fig. 3b). However, in AA subjects that received diphenylcyclopropenone (DPCP) immunotherapy only, the level of cTnI was significantly lower compared to subjects not receiving any treatment (Fig. 3c). No significant difference was observed in the level of CRP with either minoxidil only or DPCP only treatment, albeit the level was highest in subjects who received DPCP (Fig. 3d).
Fig. 3. Alopecia areata (AA) and androgenetic alopecia (AGA). AA subjects not currently receiving treatments exhibited higher levels of cardiac troponin I (cTnI). AA subjects who were not receiving any treatments for hair loss showed significantly higher levels of cTnI compared to those who were receiving treatments (a). However, the release of C-reactive protein (CRP) was not significantly correlated to treatments (b). AA patients who received diphenylcyclopropenone (DPCP) showed significantly lower levels of cTnI compared to the no treatment group (c) but highest levels of CRP (d). Statistical significance was determined with one-way ANOVA where * denotes p < 0.05.
Cell culture media supplemented with AA subject plasma samples with higher levels of cTnI were able to induce significantly higher expression of early stage apoptosis marker Annexin V, as well as late stage apoptosis marker PI, in HCM compared to media supplemented with AA subjects’ plasma exhibiting low cTnI levels. No statistically significant increases in apoptosis were observed with AGA subject and NHL subject plasma samples regardless of cTnI levels (Fig. 4a, b). Media supplemented with plasma from NHL subjects resulted in close to baseline levels of apoptosis in HCM.
Fig. 4. Alopecia areata (AA) and androgenetic alopecia (AGA). AA subject plasma samples with high levels of cardiac troponin I (cTnI) induced apoptosis in primary human cardiomyocytes (HCM) compared to samples with low levels of cTnI and AGA groups. AA plasma samples with higher levels of cTnI induced significantly higher levels of Annexin V expression in primary HCM compared to their low cTnI level counterparts (a). Significant difference was also observed between AA subjects with high cTnI and AGA and NHL subject groups. AA plasma with high cTnI also induced significantly higher PI expression in HCM compared to low cTnI (b). Significance was determined using ANOVA followed by Fisher’s Least Significant Difference (LSD) test where *denotes p < 0.05.
Most of the cytokines measured by multiplex assay showed no significant differences between samples. However, several cytokines such as IL-12, IL-13 and sIL-2R showed the highest level in AA and AGA patients, regardless of whether the subjects had high or low plasma cTnI. Other common inflammatory cytokines like IFNα and IL-1RA were also elevated in AA and AGA patients to a lesser extent.
The association between AGA and various CVDs have been suggested by multiple epidemiological studies and meta-analyses (1-3, 5, 24–27). Several epidemiological studies have reported a potential link between hair loss and CVDs in males, though these observations were made as part of larger studies which may have confounding factors or missing information (25–27). Subsequent meta-analyses were limited by the high variability in the way observations were made in different reports, but these studies provided valuable first hints of potential association (1–3). More recent controlled studies with larger cohorts implied associations between early AGA onset and CVDs, especially in males with Type III vertex hair loss (5). To our knowledge, only one small cohort study has focused on female AGA and CVDs (24).
In our previous study with the C3H/HeJ mouse model for AA, we observed enlargement of the heart and heart blood vessels, somewhat similar to dilated cardiomyopathy and/or atrial fibrillation (AF). Mice with AA exhibited significantly elevated cTnI levels in heart tissue extracts, and a trend for elevation in blood plasma, relative to littermates with no hair loss (9). We also found expression of IL18 and IL18r1 limited to the atrial tissues of AA mice. In humans, both dilated cardiomyopathy and AF are associated with increased cTnI release (28, 29). Elevated IL-18 is associated with AF and other CVDs, and has been shown to promote significant heart remodelling (30, 31).
Arrhythmias, including AF, can develop in the absence of overt structural heart disease (32). The presence of AF can increase the risk for, and severity of, stroke (33), and elevated plasma cTnI levels in AF patients are a prognostic indicator for stroke risk (34). Stroke occurs due to a lack of blood supply to the brain and body, and AF increases the risk of blood clotting in the atria (30, 35). A retrospective study indicated no significant difference in AA patients’ risk for myocardial infarction and stroke (36). However, a recent study which involved a 3-year follow-up of AA patients and non-AA subjects, reported a significant increase in the rate of stroke in AA patients (37). Unlike psoriasis and RA, any link between AA and CVDs is less clear, but the observations of cardiac remodelling in the AA mouse model, a small but significant increase in cTnI release in AA patients, and a possible increased risk of stroke in AA patients, circumstantially suggests a relationship.
In sex- and age-matched humans, both male and female subjects affected by AA exhibited significantly higher plasma cTnI levels on average compared to AGA and NHL subjects (Fig. 1). While plasma C-reactive protein levels showed similar trends, statistical significance was not achieved (Fig. 1b, d). Compared to CRP, the level of cTnI has a more direct relationship with the heart since it is a specific muscle regulatory protein produced by cardiac muscle cells (15 16). While cTnI is a strong predictor for heart failure in advance of myocardial ischemia (16), the levels of cTnI detected here for all 3 subject groups were below what is classified as positive for clinical heart disease (usually >10 ng/ml) (22). Therefore, the results indicate that AA subjects may be experiencing higher levels of cardiac remodelling, but in the absence of overt CVDs. Similar observations have been made in RA patients where higher cTnI levels may be an indication of subclinical cardiac injury (21).
Normal physiological differences in cTnI production between males and females are likely reflected in our results. The plasma level of cTnI is higher in the general male population even without the presence of CVDs (38), though whether this is an indication of higher susceptibility to subsequent CVD development is unknown. Young age of AGA onset is known to be associated with increased risk of CVDs later in life (2, 5, 6). In a study that followed RA patients for 5 years, it was found that young adults had the highest CVD risk (39). We showed increased plasma cTnI was generally observed in younger male populations (18–35) with either AA or AGA (Fig. 2c); in addition, male AA patients expressed significantly higher amounts of cTnI than AGA and NHL males (Fig. 2a). Given the apparent relationship between CVD risk and young age at AGA or RA onset in males, it may be appropriate to more closely evaluate young male AA patients for cardiovascular health.
Our data suggests that treatments for AA may have a significant effect on plasma cTnI levels. DPCP is used to treat AA by inducing a mild contact dermatitis (40). Such inflammation may potentially cause an elevation of CRP as was observed here (Fig. 3b,d). In contrast, subjects who received DPCP showed relatively lower secretion of cTnI (Fig. 3c); suggesting the benefits of treating AA may extend beyond hair regrowth. Notably, AGA patients receiving finasteride and/or minoxidil did not exhibit significant changes in plasma cTnI and CRP in our study (Fig. 3c, d).
The CRP levels observed in AGA subjects seemed to be dependent on age, and were mostly opposite in trend to cTnI levels (Fig 2d). However, this difference might be attributed to the increase of low-grade inflammation as age increases (41). Female subjects showed higher CRP levels than males (Fig. 2b). It has previously been reported that females with AGA have higher levels of CRP than females without AGA and AGA males (42).
Increased CRP levels in AA subjects has previously been reported (43) and we observed similar increased expression in our cohort (Fig. 1c, d). In psoriasis it has been hypothesized that circulating inflammatory cytokines can promote heart tissue damage and development of atherosclerosis (44); CRP production is also stimulated by elevated inflammatory cytokines (45). Similar mechanisms may be involved in AA, resulting in a rise of plasma CRP. As such, whether CRP can be used as a direct indicator of cardiac tissue status in the presence of chronic inflammatory diseases is open to question.
We observed that HCMs cultured with plasma from AA subjects exhibiting high cTnI levels increased HCM apoptosis (Fig. 4). Our results circumstantially suggest that unidentified factors are present in the plasma samples of AA patients with high cTnI levels that can induce HCM apoptosis (and consequently release cTnI). The trend indicates that AA subjects with high cTnI could be at risk of increased cardiac remodelling. However, whether there is an association with CVD related risks such as hypertension (8, 46) via inflammatory cytokines, as observed in psoriasis (44), is unknown. Subjects with RA or inflammatory polyarthritis present with elevated cTnI and CRP, and these are positively correlated with CVD risk (21, 47). It is possible that the severity of inflammation in RA may be higher and more systemic than observed in AA, resulting in a higher level of harmful inflammatory cytokines. This may explain higher incidence of CVD manifestations observed in RA than in AA. Additional comparisons showed recent onset of AGA was associated with higher cTnI plasma levels, but the difference was insignificant in AA (Appendix S1; SFig. 1a). CRP level showed an overall increased trend as the duration of AA and AGA increased, but no significant difference was observed (SFig. 1b). We also stratify AA patients into groups based on their current extent of hair loss and found no clear trend between in the levels of cTnI and CRP between those with <25% to 25–75% and >75% (Appendix S1; SFig. 2 a, b). This is most likely because AA patients may experience spontaneous regrowth in one spot but losing hair in another spot, resulting in fluctuating levels of the biomarkers we tested.
Investigation of cytokine expression in the plasma samples from AA, AGA and NHL did not identify a specific relationship between cytokines and HCM apoptosis. The overall levels of IL-12, IL-13 and sIL-2R were higher in subjects experiencing hair loss, regardless of their plasma cTnI level (Fig. 5). Interestingly, previous studies have identified elevation of these cytokines in different CVDs (48–50). The activation of lymphocytes in AA patients most likely resulted in the elevation of these cytokines, however, it is unknown why AGA patients also had higher cytokine levels (albeit still lower than AA subjects). Nevertheless, the result could suggest that the levels of cTnI and CRP in hair loss patients may be independent of inflammatory cytokine expression.
Fig. 5. Alopecia areata (AA) and androgenetic alopecia (AGA). Subjects experiencing hair loss secreted higher levels inflammatory cytokines. Plasma samples from AA and AGA subjects with either highest or lowest cardiac troponin I (cTnI) levels were compared with subjects with no hair loss (NHL). Multiplex analysis of 25 inflammatory cytokines revealed overall higher expression of IFNα, IL-13, IL-1RA and IL2R in subjects with either AA or AGA regardless of the level of cTnI found in the plasma samples.
In conclusion, our results indicate that the development of AA may be associated with cardiac remodelling, as reflected by higher plasma cTnI levels. The study data presented here, together with the previous study in the AA mouse model, are consistent with an increased risk of cardiac-related complications, though evidence to link AA to increased CVD risk or subclinical forms of heart disease is still lacking. Our study is limited by the small population size as well as the absence of comprehensive medical background information. However, we have provided some initial evidence that heart tissue remodelling may occur at a subclinical level in AA subjects. Investigations involving a larger population with more comprehensive background information will help elucidate the association of AA, and AGA, with CVD risk.
We thank Vancouver General Hospital-Skin Care Centre and the Clinical Research Unit for the collection of blood samples and subject data. This study was supported by the Canadian Institutes of Health Research (CIHR; MOP-82927). EW is the recipient of a Banting Postdoctoral Fellowship (SAC-92845).
Conflict of interest disclosure: KM is Chief Scientific Officer and shareholder for Replicel Life Sciences Inc., JS is a Replicel Life Sciences Inc shareholder. All other authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize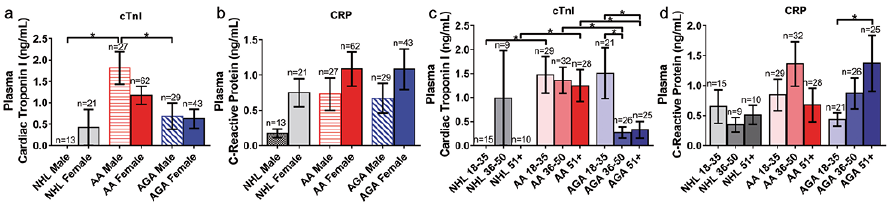 Click to show fullsize
Click to show fullsize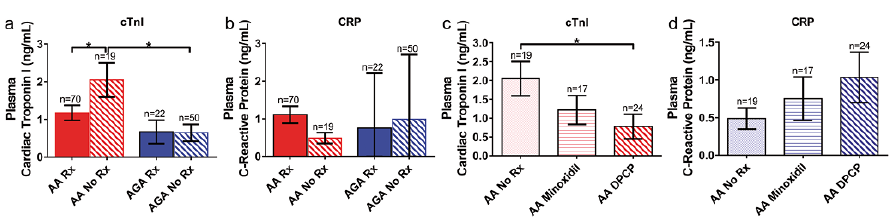 Click to show fullsize
Click to show fullsize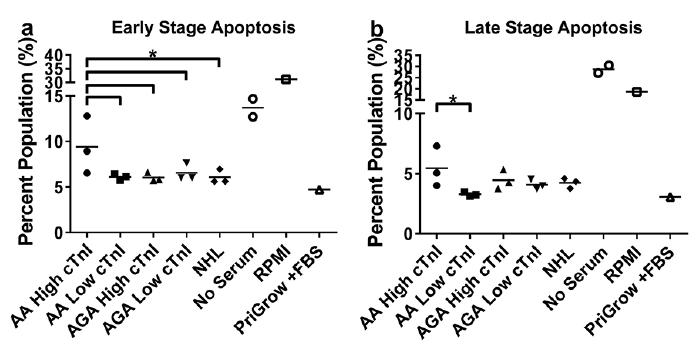 Click to show fullsize
Click to show fullsize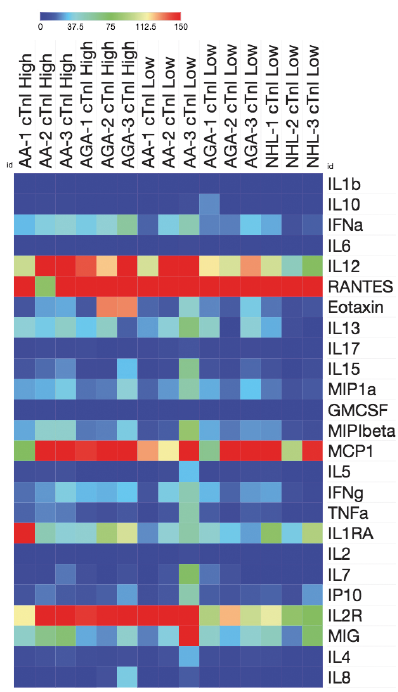 Click to show fullsize
Click to show fullsize