


1Department of Dermatology, Rush University, Chicago, 2Lewis Katz School of Medicine, 3Department of Dermatology, Temple University, Philadelphia, 4Department of Medicine, Division of Rheumatology, Thomas Jefferson University, Philadelphia, USA, 5Department of Dermatology, Royal Liverpool and Broadgreen University Hospitals NHS Trust, Liverpool, UK, 6Biostatistics Unit, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore, and 7Department of Dermatology and Itch Center, University of Miami Miller School of Medicine, 1600 NW 10th Ave, Rosenstiel Medical Science Bldg., Miami, FL 33136, USA. *E-mail: yosipog@gmail.com
Accepted May 4, 2018; Epub ahead of print May 8, 2018
Chronic itch (present for ≥ 6 weeks) is a common symptom in the systemic sclerosis (SSc) population with a reported prevalence of 42.6 % (1). Previous studies have demonstrated that chronic itch is associated with decreased quality of life and sleep in SSc patients (2, 3). However, little is known about the characteristics and pathogenesis of itch in the context of this disease.
To further elucidate features of itch in SSc patients, we conducted a cross-sectional survey. The protocol for this study was approved by the Institutional Review Board at Thomas Jefferson University. Patients presenting to the rheumatology clinic with an established diagnosis of SSc were asked if they experienced itch for ≥ 6 weeks. Those who responded affirmatively completed two validated questionnaires: The Itch Questionnaire and the itch-specific quality of life (ItchyQoL) (4, 5). Itch intensity was quantified using a numeric rating scale (NRS) (range 0–10). Skin involvement was assessed using the modified Rodnan skin score (mRSS) (range 0–51), and affected body surface area (BSA).
All analyses were performed using SPSS 24.0 with statistical significance set at p < 0.05. The differences in numerical parameters between the chronic itch and without chronic itch groups were compared using t-tests when normality and homogeneity assumptions were satisfied, otherwise Mann Whitney U tests were used. Chi-square or Fisher’s Exact tests were used to compare categorical variables between the 2 groups.
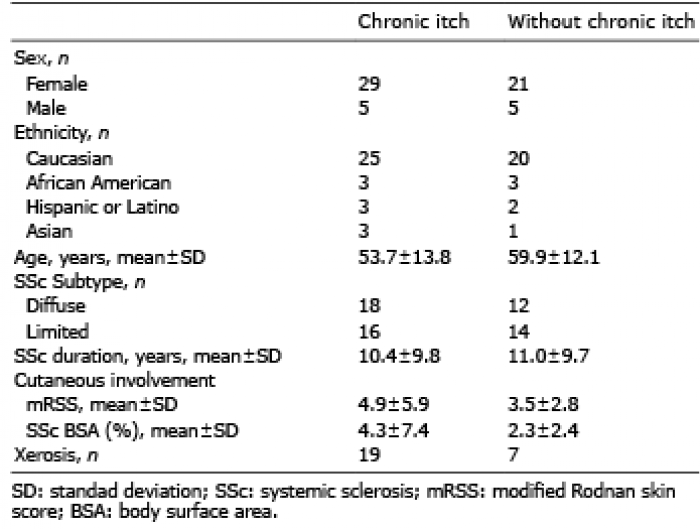
Chronic itch was present in 34 (56.7%) of 60 patients. Demographic and clinical features of our sample are presented in Table I. Characteristics of itch are presented in Table II. Chronic itch was significantly associated with xerosis (p = 0.025). The most common locations for pruritus were the back (n = 21), arms (n = 17) and scalp (n = 16). Itch was described as prickling (n = 13), painful (n = 11), burning (n = 9), and stinging (n=8). Itch was not significantly associated with the presence of autoantibodies including anti-nuclear antibodies (ANA), anti-double stranded DNA antibodies (dsDNA), anti-topoisomerase I antibodies (Scl-70), anti-centromere antibodies, anti-RNA polymerase III antibodies, and anti-U3 RNP. In addition, there were no significant relationships between itch and systemic manifestations of SSc, including interstitial lung disease, pulmonary hypertension, renal involvement, gastrointestinal involvement, or joint pain. Furthermore, there were no significant associations between itch and the use of immunosuppressive therapies including mycophenolate mofetil, methotrexate, prednisone and rituximab. The mean ItchyQoL score was 43.4 ± 15.7 out of 110. The severity of itch was correlated with affect on sleep (r = 0.424, p = 0.013), and difficulty concentrating (r = 0.362, p = 0.035).
Table I. Demographic and clinical characteristics
Table II. Chronic itch characteristics
Our findings suggest that xerosis may be a prominent cause of itch in SSc patients. Itch was most severe during the winter and most commonly exacerbated by dry skin, lending further support to this observation. However, the etiology of itch in these patients is likely to be multifactorial. Interestingly, the body areas most affected by itch were the back, scalp and arms. Similar findings regarding the distribution of itch were also reported in a French SSc population (2). This distribution suggests that there could be an underlying neuropathic mechanism of itch in SSc patients. Indeed, a prior study using quantitative sensory testing revealed the presence of peripheral sensory neuropathy in SSc patients, which may contribute to pruritus (6).
Notably, there was a lack of association between itch and duration of disease. However, the patients who comprised our cohort were considered to have stable disease, and it is possible that outcomes may differ in those with rapidly progressive SSc.
Our findings raise interesting questions regarding the treatment of itch in SSc patients. Immunosuppressive agents including methotrexate and mycophenolate mofetil have demonstrated antipruritic effects in several inflammatory diseases (7). However, itch was present in many of our subjects receiving these therapies. It would be of interest to assess whether neuroactive medications such as gabapentin or pregabalin, which are commonly used to treat neuropathic itch, would provide greater relief to these patients (7).
Conflicts of interest: Drs Stull, Weaver, Valdes-Rodriguez, Naramala, Chan and Mendoza have no conflicts of interest to disclose. Dr. Yosipovitch serves as a consultant for Trevi, Menlo, Sienna, OPKO, Galderma, Sanofi, Eli Lilly, Novartis and Pfizer, and receives grant support from Sun pharma and Pfizer.


 Click to show fullsize
Click to show fullsize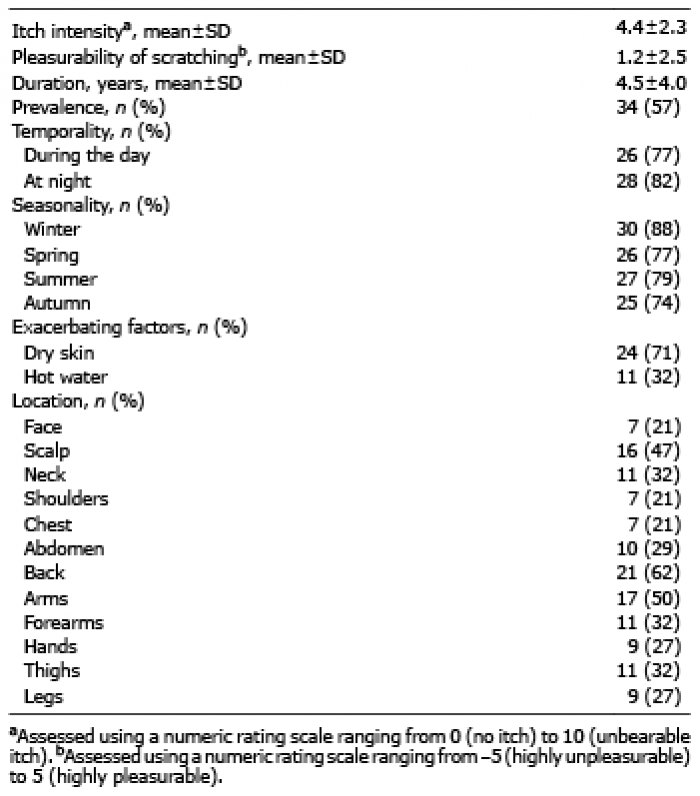 Click to show fullsize
Click to show fullsize