


1Health, Medical and Neuropsychology Unit, Institute of Psychology, 2Leiden Institute for Brain and Cognition (LIBC), 3Department of Psychiatry, Leiden University Medical Center, Leiden, and 4Department of Dermatology, Radboud University Medical Center, Nijmegen, The Netherlands
Nocebo effects, i.e. reduced treatment effects due to patients’ negative expectations, play a role in itch. Recent studies have shown that nocebo effects can be induced experimentally on itch and also be minimized and even turned into the opposite direction, i.e. placebo effects. It is not known whether these effects generalize to itch-associated scratching behaviour. The aim of this study was to determine whether induction and reversal of nocebo effects on itch evoked by electrical and histamine stimuli generalized to scratching. Ninety-seven healthy participants were included in the study. The manipulation was successful, as during the nocebo learning phase, increased scratching responses were found for higher intensity compared with lower intensity itch stimuli. During the testing phase of induction or reversal of the nocebo effects, however, no significant nocebo effects or reversed nocebo effects, were found in scratching. Thus, no straightforward generalization of nocebo effects from itch to scratching was found in this laboratory setting. Further investigation into possible generalization is needed in different settings and in patients with chronic itch.
Key words: placebo; nocebo; itch; conditioning; verbal suggestion; scratching.
Accepted May 29, 2018; Epub ahead of print Jun 1, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Danielle J. P. Bartels, Health, Medical and Neuropsychology Unit, Leiden University; PO Box 9555; 2300 RB Leiden, The Netherlands. E-mail: d.bartels@fsw.leidenuniv.nl
Scratching plays an important role in skin conditions due to a vicious itch-scratch cycle. It is known that patients’ expectations regarding a treatment can influence itch in skin conditions by placebo and nocebo effects. We investigated whether induced and reversed nocebo effects regarding itch also generalize to scratching behavior. Although participants scratched more during itch stimuli of higher intensity, hardly any nocebo effects, or reversed nocebo effects, on scratching were found. Potential generalization of placebo and nocebo effects from itch to scratching should be further investigated to possibly enhance treatments for chronic itch in clinical practice.
Itch and scratching are common symptoms in skin conditions such as psoriasis and atopic dermatitis, and can cause significant impairment for patients (1). Scratching may have an important role in the maintenance and exacerbation of skin conditions due to a vicious itch-scratch circle (2, 3). Effects of pharmacological treatments are relatively limited and these treatments often have side-effects (4). Treatment effectiveness may be improved by optimizing placebo effects, while minimizing nocebo effects (5, 6).
Placebo and nocebo effects are positive and negative treatment effects, unrelated to the treatment mechanism, which are induced by patients’ expectations of improvement or worsening, respectively (7–9). Placebo and nocebo effects are known to contribute to various conditions and symptoms, and have been investigated mainly with regard to pain (7). Recent studies have demonstrated that placebo effects can reduce levels of itch in healthy participants as well as in patients with clinical itch due to chronic conditions (5, 6, 10, 11). Moreover, nocebo effects, which may play an even more important role in clinical practice (8, 12), can amplify itch, and these nocebo effects on itch can also be minimized and even turned into the opposite direction, i.e. a placebo effect (13). Overall, the combination of enhancing placebo effects on itch and reversing nocebo effects seems to be a promising target to further optimize treatment effects for itch. In addition, there are indications that placebo and nocebo effects on a specific symptom can generalize to other modalities or domains (14–19). Thus, nocebo and placebo effects associated with itch treatments may also generalize to the behavioural domain, by which patients’ scratching behaviour (14, 15) may be influenced in a negative or positive direction, respectively.
Studies on contagious itch provide some evidence that nocebo-like effects on itch are also seen on scratching behaviour. For example, when participants watched videos of people scratching compared with control videos, they not only reported higher ratings of overall itch, but also scratched more frequently, with the largest effects for patients with chronic itch (16). However, it is not known whether induced nocebo effects on itch also generalize to scratching behaviour.
The aim of this experimental study was to investigate, for the first time, whether induced nocebo effects on itch (electrically induced) generalize to scratching behaviour in healthy participants. As described previously in our article focusing on the levels of itch experienced within the same experiment (13), participants first learned negative expectations about electrical itch stimuli by coupling (through conditioning and verbal suggestions) a certain cue with increased intensities of itch. Next, participants were randomized to either the experimental group in which the cue was coupled with lowered itch intensities (positive expectation induction) or one of the control groups in which either negative expectation induction with the increased intensities of itch continued, or no expectations were induced and only itch stimuli of medium intensity were applied (extinction) (13).
The current study focuses on the behavioural outcome of scratching. It was hypothesized: (i) that itch amplification by nocebo effects would generalize to enhanced scratching, and (ii) that subsequent reversion of the nocebo effects on itch into placebo effects would generalize to decreased scratching. In addition, this study exploratively investigated whether reversion of the nocebo effects on itch also generalized to scratching associated with an additional itch stimulus (histamine iontophoresis). Frequency of localized scratching was the primary outcome measure, in line with a previous study on evoked itch (17). Frequency of total-body scratching was the secondary outcome measure (16, 18–20). Exploratory, we also analyzed duration of localized and total-body scratching.
The design and methods have been described in full previously, in our article focusing on reversing nocebo effects in self-reported itch (13). A brief summary is given below.
A total of 129 healthy participants were included in the study (mean ± standard deviation (SD) age 20.3 ± 2.5 years; 78.7% women). Inclusion criteria were: age range 18–35 years, and fluency in the Dutch language. Exclusion criteria were: severe physical morbidity (e.g. skin disease, diabetes mellitus, multiple sclerosis), psychiatric disorders, chronic itch or pain, diagnosis of histamine hypersensitivity, regular use of medication in the last 3 months, use of a pacemaker, colour blindness, and pregnancy. The study was approved by the medical ethics committee of the Leiden University Medical Center in Leiden, the Netherlands (Commissie Medische Ethiek). All participants provided written informed consent and were reimbursed for their participation.
The study followed a balanced (1:1:1) randomized controlled, multi-arm parallel-group, double-blind design comprising 3 experimental parts (see Fig. 1 for an overview of the experimental study parts). In Part 1, negative expectations were induced regarding electrical itch stimuli (induction of nocebo effect). In Part 2, participants were randomized over 3 groups in which they received either a positive expectation induction (induction of placebo effect; group 1; n = 33), a continued negative expectation induction (induction of nocebo effect; group 2; n = 34), or an extinction procedure (extinction; group 3; n = 30) with regard to electrical itch stimuli. Both Parts 1 and 2 comprised a learning phase and a testing phase, in which itch stimuli were accompanied by visual cues on a computer screen, i.e. purple and yellow coloured circles. By randomization it was determined whether the conditioned cue was purple or yellow and the neutral cue, consequently, yellow or purple. The following assumes that the conditioned cue is purple and the neutral cue is yellow. In the learning phase of Parts 1 and 2, participants were told that a purple cue would indicate the activation of the third (sham) electrode that increased (nocebo groups) or decreased (placebo groups) the intensity of the itch stimulus. They were also told that the yellow cue would indicate deactivation of the third electrode so the itch stimulus would remain at medium intensity. Conditioning was achieved by applying high (nocebo groups) or low (placebo group) itch stimulus intensities, along with the purple cue (i.e. conditioned trials; 10 stimuli) and medium itch stimulus intensities along with the yellow cue (i.e. neutral trials; 6 stimuli). During the testing phases of Part 1 and 2, all stimuli were given at medium intensity (8 stimuli), while displaying either the purple or yellow cue (both 50% of the trials). In the third part histamine was applied along with the same cue as was used for conditioning in Part 2 (see Fig. 1).
Fig. 1. Experimental design. In part 1, negative expectations were induced: participants were told that the purple cue (conditioned cue) indicated an increase in the itch stimulus, and that the yellow cue (neutral cue) indicated no change in the itch stimulus. In accordance, the purple and yellow cues were repeatedly paired with high and medium electrical itch stimulus intensities, respectively. In part 2, participants were randomized over the 3 groups in which: (i) positive expectations were induced; (ii) continued negative expectations were induced; or (iii) an extinction procedure was applied. In the learning phases verbal suggestion and conditioning procedures depended on the experimental group. In the testing phases the verbal suggestion corresponded to the verbal suggestion provided in the learning phase, while all participants received electrical itch stimuli of medium intensity. In part 3, for all participants, histamine iontophoresis was applied at the same intensity. The verbal suggestions corresponded with those provided in Part 2, and the purple cue (conditioned cue) was displayed during the histamine application. Note that for half of the participants the conditioned cue was a purple cue and the neutral cue a yellow cue (like in this example); for the other half of the participants the conditioned cue was yellow and the neutral purple.
Electrical itch induction. A constant current stimulator (Isolated Bipolar Constant Current Stimulator DS5, Digitimer, Welwyn Garden City, UK) was used to induce itch to the inner side of the non-dominant wrist through 2 surface electrodes. A third (sham) electrode functioned as placebo. Three intensities of itch were individually determined (i.e. low, medium, and high). For the exact procedure see (10). Previous research indicated that itch was the predominant sensation with this induction, and significantly higher than pain (21).
Histamine iontophoresis. Using disposable iontophoresis electrodes (Iogel, Chattanooga, Hixson, TN, USA), 0.6% histamine (as diphosphate) (22) solution (in which histamine content is comparable to 1% histamine dihydrochloride) was delivered with a dose controller (Chattanooga Ionto, Chattanooga) for 2.5 min at a current level of 0.4 mA to the dominant forearm (for the exact procedure see (10)).The same sham electrode used during electrical stimulation served as placebo.
A video-camera (Panasonic HC-V700, Panasonic Corporation, Osaka, Japan) was located left front of the participant in order to record participants’ scratching behaviour. A mirror was located at the right side of the participant to capture an image of the entire body. An event logging software program (The Observer XT 12, Noldus Information Technology bv, Wageningen, The Netherlands) was used to code the scratching responses (see “Coding of scratching behaviour”, below).
Potential participants were screened for eligibility using online self-report screening questionnaires (Qualtrics, Provo, USA) on demographic variables, and physical and psychological conditions (see (13)). In advance of the laboratory visit, participants were asked to refrain from taking any medication, alcohol, and drugs for at least 24 h before the testing, and from smoking cigarettes or drinking coffee, tea, cola, or energy drinks at least 2 h before testing. At the laboratory visit, the procedures were explained to the participant and informed consent was obtained. Participants were informed that they were being videotaped, although they were given the cover story that the recordings were used for training purposes. Baseline itch, pain, and fatigue were obtained using numerical ratings scales (NRSs) ranging from 0.0 (no itch/pain/fatigue at all) to 10.0 (most itch/ pain/fatigue ever experienced). After this, the 3 intensities for electrical itch stimulation (i.e. low, medium, and high) were individually determined (see “Electrical itch induction”).
In Part 1, negative expectations regarding electrical itch stimuli were induced (induction of nocebo effect, see also Fig. 1). In Part 2, participants were allocated randomly to 1 of 3 groups (see Fig. 1). In the positive expectation induction group (induction of placebo effect; group 1), expectations of low and medium levels of itch were raised in the participants. Thus the meaning of the colour of the conditioned cue was reversed compared with Part 1. In the negative expectation induction group (induction of nocebo effect; group 2), exactly the same nocebo procedure was applied as in Part 1. In the extinction group (extinction; group 3) all stimuli were applied at medium intensity and no verbal suggestion was provided. Participants were merely told that several stimuli would be applied again, accompanied by purple or yellow cues, without being given further details. In Part 3, for all participants, histamine iontophoresis was applied at the same intensity. The verbal suggestions corresponded with those provided in Part 2. Between the stimuli there were standardized inter-stimulus intervals and during the experimental session several standard breaks (13).
Participants were informed 4 times that they were allowed to scratch their itch freely at any time: 3 times during the session with electrical itch stimulation (before determining the individual itch thresholds; before the start of Part 1; and before the start of Part 2) and once before the start of histamine iontophoresis.
At the end of the experiment, participants rated the levels of pain that were induced overall by the electrical itch stimuli on an NRS from 0.0 to 10.0 with a mean ± SD of 1.0 ± 1.2. Finally, saliva was collected for DNA analysis (the results will be reported elsewhere) and participants were asked about their impression of the goal of the study. Almost all participants did not know the true goal of the study.
Spontaneous scratching was coded using the video-recordings by an independent rater who was unaware of the participant’s allocation to 1 of 3 groups and the colour of the conditioned and neutral cue. Scratching was defined as any skin contact movement that could reduce itch, e.g. typical scratching using the fingernails, picking with fingernails, or rubbing, while not taking into account touching (16, 20). Regarding the electrical itch stimuli, scratching behaviour was coded from the start of an itch stimulus up to the next trial (up to 2 min) for the learning and testing phases separately. For the histamine stimulus, scratching behaviour was coded for the 2.5-min duration of the stimulus. Scratching responses were mapped spatially: (i) strictly localized (up to 5 cm around the electrodes); (ii) extended localized on the stimulated arm, excluding strictly localized areas; (iii) extended other arm; (iv) extended head/face/neck; (v) extended torso; and (vi) extended legs. For the preparation of the variables for the analyses, a distinction was made between localized (areas 1 and 2 together) (17) and total-body scratching (areas 1–6 together) (16, 18, 19, 20). Using The Observer software program (The Observer XT 1), frequency (primary outcome) and duration (explorative outcome) of scratching were calculated separately for the different cues and the testing and learning phases.
Of the 129 participants tested, data for 97 could be included in the analyses, as 32 were excluded from data analysis on the basis of several pre-determined criteria (see (13)). Specifically, for 8 participants data collection had failed and 24 participants were excluded (with the permission of the local ethics committee) because they experienced no or too little itch after repeated electrical itch induction (for details see (13)). However, sensitivity analyses were also carried out for all 121 participants, including those in whom levels of evoked itch were low but scratching data were available.
In line with the main aims, for all outcomes, frequency of localized scratching was regarded as the primary outcome, frequency of total-body scratching was regarded as the secondary outcome and duration of localized and total-body scratching was analysed exploratively. Means of scratching were calculated for both conditioned (i.e. with the supposed activation of the third electrode) and neutral trials (i.e. without the supposed activation of the third electrode) for the learning and testing phases. The nocebo effect on scratching was defined as the difference between scratching episodes associated with the conditioned trials and neutral trials. The higher the score the higher was the nocebo effect.
To explore the efficacy of the nocebo expectation induction procedure during the learning phase in Part 1, scratching episodes associated with the conditioned and neutral trials were compared in paired samples t-tests. Also, to test the hypothesis that there was a nocebo effect on scratching in the testing phase of Part 1, paired samples t-tests were performed.
The efficacy of the expectation induction procedure in the learning phase of Part 2 was assessed exploratively by univariate analyses of variance (ANOVA) with group as between-subject factor and scratching as dependent variable. Similar ANOVAs were performed for the testing phase of Part 2 when testing the hypothesis that the positive expectation induction group would display a significantly smaller nocebo effect with regard to scratching than the control groups (negative expectation induction group and extinction group). A similar approach was taken to exploratively assess generalization of the reversion of nocebo effects on itch to scratching during the histamine stimulus, whilst including the scratching scores during histamine iontophoresis.
Where the assumptions of the statistical tests (e.g. of normality) were violated, sensitivity analyses were conducted by calculating bias-corrected 95% confidence intervals (95% CIs) around the relevant parameter using 1,000 bootstrapping samples (23). This was the case for the duration of localized scratching in the testing phase of Part 1, as well as the frequency and duration of localized scratching behaviour in the testing phase of Part 2. Since bootstrapped confidence intervals around the parameters provided results similar to those reported without bootstrapping, we reported the non-bootstrapped analyses.
All analyses were performed using SPSS 23.0 for Windows (IBM SPSS Statistics, Chicago, IL, USA) and the level of statistical significance was set at p < 0.05 (2-sided). Unless displayed otherwise, results are displayed as means ± SD.
In Part 1 (induction of nocebo effect), negative expectations were induced in all participants. In Part 2 (reversal of nocebo effect), randomization of the participants across the 3 groups resulted in a total of 33 participants in the positive expectation induction group, 34 participants in the negative expectation induction group, and 30 participants in the extinction group. The groups did not differ significantly on baseline characteristics (Table I).
Table I. Participant characteristics
Learning phase. During the learning phase of Part 1 (Table II), in which negative expectations were induced for all participants by both verbal suggestion and conditioning, as expected, the paired samples t-tests revealed that means for the conditioned trials were significantly higher than for the neutral trials for the frequency of localized scratching (t(96) = 3.89, p < 0.001, d = 0.395), duration of localized scratching (t(96) = 4.13, p < 0.001, d = 0.420), and duration of total-body scratching (t(96) = 3.07, p < 0.01, d = 0.312). The frequency of total-body scratching was marginally significantly higher for the conditioned vs. neutral trials (t(96) = 1.94 p = 0.056, d = 0.196).
Table II. Mean frequency and duration of scratching episodes in the learning and testing phase in Part 1 (induction of negative expectations)
Testing phase. When testing whether there was a nocebo effect during the testing phase of Part 1 (Table II), in which all stimuli were applied at medium intensity, the paired samples t-test revealed that means for the conditioned trials were marginally significantly higher than for the neutral trials for frequency of localized scratching (t(96) = 1.77, p = 0.081, d = 0.179) and duration of localized scratching (t(96) = 1.77, p = 0.079, d = 0.180). No significant nocebo effect was found for total-body scratching regarding the frequency (t(96) = 0.63, p = 0.53, d = 0.064) and duration (t(96) = 1.46, p = 0.15, d = 0.148).
Learning phase. Table III displays the mean ± SD frequency and duration of the scratching episodes evoked by the itch stimuli associated with the conditioned and neutral trials during the learning phases for each group, in which depending on the group, positive (group 1) or negative (group 2) expectations were induced or an extinction procedure (group 3) was applied. When testing whether the mean change score (conditioned trials minus neutral trials) of scratching episodes was smaller in the positive expectation induction group (group 1) than in the control groups (groups 2 and 3), ANOVAs did not reveal a significant group difference for any of the outcome measures: frequency of localized scratching (F(2,96) = 1.37, p = 0.259 ηp2 = 0.028), frequency of total-body scratching (F(2,96) = 2.09, p = 0.130, ηp2 = 0.042), duration of localized scratching (F(2,96) = 1.43, p = 0.244 ηp2 = 0.030) and duration of total-body scratching (F(2,96) = 0.95, p = 0.391, ηp2 = 0.020).
Table III. Mean frequency and duration (s) of scratching episodes in the learning phase in Part 2
Testing phase. Table IV displays the mean ± SD frequency and duration of the scratching episodes evoked by the itch stimuli associated with the conditioned and neutral trials during the testing phase for each group, in which all stimuli were applied at medium intensity. When testing the hypothesis that the nocebo effect on frequency of localized scratching was smaller in the positive expectation induction group than in the control groups, univariate ANOVA showed no significant difference in the magnitude of the nocebo effect (F(2,96) = 0.36, p = 0.697 ηp2 = 0.008). Also, for the frequency of total-body scratching (secondary outcome) no significant difference between the groups was observed (F(2,96) = 0.90, p = 0.409 ηp2 = 0.019). Furthermore, also regarding duration of scratching episodes, no significant difference in localized scratching (F(2,96) = 0.78, p = 0.463 ηp2 = 0.016) or total-body scratching (F(2,96) = 1.30, p = 0.279 ηp2 = 0.027) was found between the groups.
Table IV. Mean frequency and duration (s) of scratching episodes in the testing phase in Part 2
When exploring scratching behaviour during the histamine stimulus (Table V), ANOVAs showed no significant effect of group regarding the frequency of localized scratching (F(2,96) = 0.62, p = 0.54, ηp2 = 0.013), frequency of total-body scratching episodes (F(2,96) = 0.56, p = 0.57, ηp2 = 0.012), duration of localized scratching episodes (F(2,96) = 0.32, p = 0.73, ηp2 = 0.007), or duration of total-body scratching episodes (F(2,96) = 0.25, p = 0.77, ηp2 = 0.005).
Table V. Mean frequency and duration (s) of scratching episodes during application of histamine
When exploring the influence of excluding the data of the 24 participants who experienced little to no itch after repeated electrical itch induction (<1 itch on NRS), sensitivity analysis with all 121 participants for whom scratching data were available generally obtained results similar to those for the 97 participants, with some exceptions. Specifically, in the testing phase of Part 1, instead of a marginally significant difference, results revealed a significantly higher mean ± SD frequency of localized scratching episodes for the conditioned trials (0.3 ± 0.4) than for the neutral trials ( 0.2 ± 0.3) (t(120) = 2.36 p < 0.05, d = 0.214), and a longer mean duration of localized scratching episodes for the conditioned trials (1.0 ± 1.8) than for the neutral trials (0.8 ± 1.5) (t(120) = 2.27, p < 0.05, d = 0.206). In the testing phase of Part 2, instead of a non-significant difference, there was a tendency towards significance in the magnitude of the nocebo effect of duration of total-body scratching between the positive expectation induction group and the control groups (F(2, 120) = 2.78, p = 0.066, ηp2 = 0.045).
The present study investigated, for the first time, the generalizability of induced nocebo effects on itch to scratching behaviour. First, results showed that, while manipulating the itch intensity during the nocebo learning phase, participants scratched more often and for a longer duration when itch stimuli of a higher intensity were applied than when itch stimuli of medium intensity were applied. However, this did not lead to subsequent significant nocebo effects on scratching behaviour in the testing phase, apart from some marginal significant effects. Secondly, reversing nocebo effects on itch by positive expectation induction, did not lead to reversed or reduced nocebo effects on scratching behaviour. Sensitivity analysis in a larger group of participants did show some significant nocebo effects on scratching and a tendency for reduced nocebo effects on scratching. We can conclude that, although higher itch intensity is associated with more scratching, no conclusive evidence for generalization of nocebo effects on itch to scratching was found.
Exposing participants to itch stimuli of high intensity (in the learning phase of nocebo induction) resulted in significantly more frequent scratching, and scratching for a longer duration, around the specific area of the forearm where itch was induced compared with itch stimuli of medium intensity. When we assessed scratching behaviour all over the body, similar findings were obtained, with significant results for duration and marginally significant results for frequency of scratching behaviour. Thus, when itch stimuli of higher intensity are applied compared with itch stimuli of lower intensity, participants not only experienced more itch (13), they mostly also displayed increased scratching behaviour, indicating a correspondence between self-report outcomes and observable behaviour (3, 18). This further supports that scratching behaviour can objectively be measured and is related to the intensity of itch (16, 18, 19).
Our hypothesis that nocebo effects on itch generalize to scratching could not be confirmed. Negative expectation induction for high levels of itch regarding stimuli of medium intensity (in the testing phase of part 1) did not result in significant nocebo effects on scratching. Also positive expectation induction for low levels of itch regarding stimuli of medium intensity (in the testing phase of part 2) did not result in significantly smaller nocebo effects on scratching for both the electrical and histamine stimuli compared with the control groups. These findings are unexpected, since our study did show significant nocebo effects on self-reported itch after negative expectation induction, and significantly reduced nocebo effects on itch after positive expectation induction when electrical or histamine itch stimuli were applied (13). A possible explanation for the non-significant results on scratching might be that, in our study, no verbal suggestions were provided for scratching, but only for itch, which is a pure way to assess generalizability of the nocebo effects on itch. Similar results were obtained in a recent study on itch perception modulated by verbal suggestion in healthy participants (24). This study demonstrated an increase in itch perception in a nocebo-like condition, but no increase in the desire to scratch. Actual scratching behaviour was not measured (24). Furthermore, in studies regarding contagious itch, i.e. itch evoked by audio-visual stimuli, inductions of expectation often indirectly address itch and especially scratching, e.g. by showing participants videos of people scratching (16–18, 20). This is, for example, confirmed by a study by Lloyd et al. (19) demonstrating that pictures of itch-relevant stimuli, e.g. insects crawling on skin, resulted in increased itch in healthy subjects than did pictures of people scratching, whereas pictures of people scratching led to more scratching behaviour than the itch-relevant pictures (19). Previous studies investigating generalizability of placebo or nocebo effects on symptoms other than itch all included verbal suggestions for the second modality. For example, a study on pain showed that conditioned nocebo effects in pain tolerance can be transferred to motor endurance; however, verbal suggestions for decreased motor endurance were also provided (25). Other studies on pain that demonstrated transferable placebo effects from pain to emotion have also provided verbal suggestions regarding alleviation of negative emotions (26–28). It is likely that the generalized placebo and nocebo effects are partly explained by additional verbal suggestions for the second modality. Another possible explanation for the lack of generalized nocebo effects on scratching in the current study could be that the levels of itch did not always reach the threshold at which participants felt the urge to scratch (15). Future research should investigate whether directly targeting scratching behaviour by induction of expectation is required to induce and reverse nocebo effects on scratching.
When comparing healthy participants with patients with chronic itch conditions, several studies have shown that patients scratch more frequently than healthy participants when an experimental itch stimulus is applied (17, 20), even when stimulus intensity and self-reported itch do not significantly differ for both patients and healthy participants (20). This is underlined by neuroimaging studies that demonstrate that different brain areas are activated in patients with chronic itch and healthy participants when itch stimuli are applied (29–31). For example, a study in patients with atopic dermatitis (AD) showed that, even though there were no significant differences in perceived itch, brain activation in areas that are assumed to correspond to scratching differed between the patients and healthy participants (29). Such differences may also play a role in placebo and nocebo effects on scratching and therefore placebo and nocebo effects on scratching should be investigated in patients with chronic itch.
Some possible limitations and further suggestions for future research should be discussed. First, participants might have been hindered in spontaneous scratching due to the filler tasks that were provided between the different itch stimuli. Since the electrodes were attached to the non-dominant arm, participants were not able to scratch around the itch-induced area of the forearm with the non-dominant hand, but only with their dominant hand. However, participants mainly used their dominant hand for completing the filler tasks and had to pause performing the tasks in order to scratch their itch. It is possible that this led to reduced scratching in participants. Future studies should consider inter-stimulus intervals with tasks whereby participants do not use their hand and are able to scratch without any constraints. Secondly, participants tended to report less itch as the experiment progressed (13). It could be that the decline in itch resulted in less often reaching the participants’ itch threshold (15) (especially in the testing phase of Part 1 and the learning and testing phase of Part 2), which could have influenced the scratching results. Thirdly, since we were interested mainly in whether nocebo effects on itch generalize to scratching behaviour, we did not directly compare localized and extended scratching behaviour (such as (17)). Given that, for contagious itch, people do not seem to scratch the same area as the area observed in the manipulation video (i.e. area on the body where the person in the manipulation video scratches), future research could manipulate the location of itch to determine whether nocebo effects on scratching are mainly localized or extended.
In conclusion, this study confirms that scratching behaviour can be used as a measure of itch in healthy participants. No conclusive evidence was found for the generalization of nocebo effects on itch to scratching; however, sensitivity analysis in a larger group of participants showed some preliminary effects or tendencies that nocebo effects on itch can generalize to scratching. Future research should investigate generalization of (reversed) placebo and nocebo effects from itch to scratching, especially when high levels of itch are experienced, exceeding specific itch thresholds that lead to scratching, and also when involving patients with chronic itch. From the clinical viewpoint, studying how a placebo effect can generalize from one domain to another may be important to increase the effectiveness of treatments for all kinds of conditions that often comprise symptoms in different modalities. The possibility of reducing symptoms in one modality, i.e. scratching behaviour, using training in another modality, i.e. itch, could possibly be applied in dermatological conditions associated with chronic itch and scratching. Therefore, greater understanding of the generalization of placebo and nocebo effects on itch to scratching behaviour could be important to determine ways to enhance treatments for chronic itch in clinical practice.
This work is supported by an Innovation Scheme (Vidi) Grant of the Netherlands Organization for Scientific Research and by a European Research Council (ERC) Consolidator Grant from the ERC. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize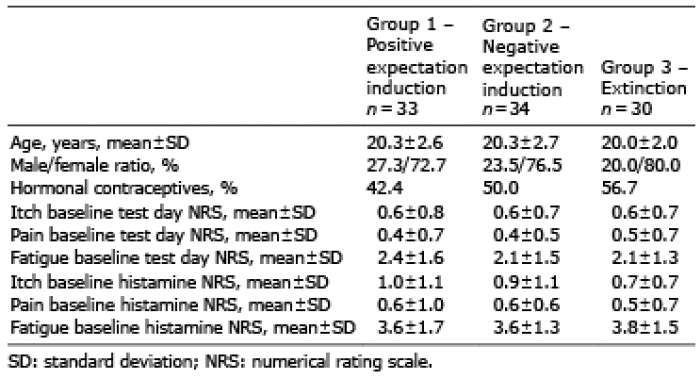 Click to show fullsize
Click to show fullsize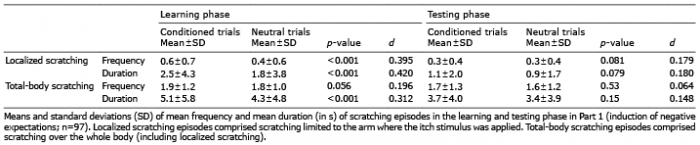 Click to show fullsize
Click to show fullsize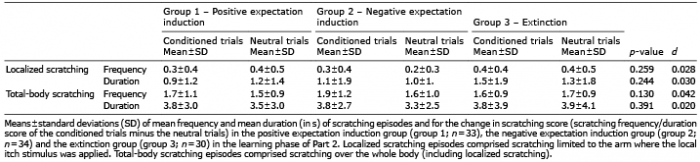 Click to show fullsize
Click to show fullsize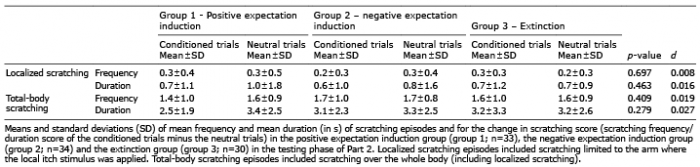 Click to show fullsize
Click to show fullsize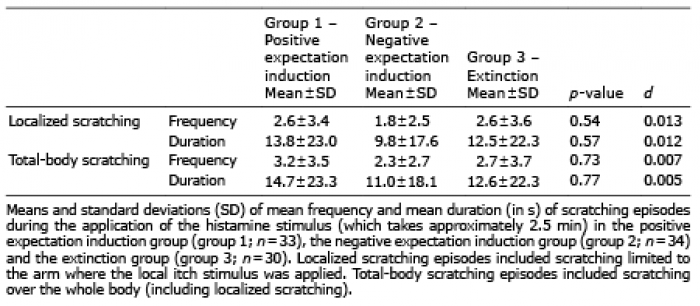 Click to show fullsize
Click to show fullsize