


1Dermatology Department, Ramon y Cajal Hospital, 2Department of Medicine and Medical Specialities, Universidad de Alcalá de Henares, Madrid, Spain, and 3Dermatology Service, Memorial Sloan-Kettering Cancer Centre, New York, USA
Treatment of actinic keratosis with 3% diclofenac sodium w/w in hyaluronic acid is associated with a concomitant improvement in signs of photodamaged skin. However this effect has not yet been examined in depth. Twenty patients with actinic keratosis and signs of photodamaged skin were studied. They received treatment with diclofenac sodium w/w in hyaluronic acid for 2 months. Clinical and reflectance confocal microscopy assessment on signs of photodamaged skin were performed. Regarding reflectance confocal microscopy, the most common descriptors were: irregular honeycomb pattern in 18/20 patients (90%), mottled pigmentation in 17/20 (85%), coarse collagen structures in all patients, and huddled collagen and curled bright structures in 16/20 (77.8%). After treatment, significant improvement in clinical parameters: irregular pigmentation and coarseness, and confocal parameters: irregular honeycomb pattern and mottled pigmentation, were noted. Reflectance confocal microscopy is a useful tool in monitoring changes in photodamaged skin after treatment. The use of diclofenac sodium w/w in hyaluronic acid is associated with an improvement in some clinical and reflectance confocal microscopy parameters of photodamaged skin.
Key words: actinic keratosis; diclofenac sodium; honeycomb pattern; mottled pigmentation; photodamaged skin; reflectance confocal microscopy.
Accepted May 29, 2018; Epub ahead of print Jun 1, 2018
Acta Derm Venereol
Corr: Gonzalo Segurado-Miravalles, Dermatology Department, Ramon y Cajal Hospital, Carretera Colmenar Viejo km 9.100, ES-28034 Madrid, Spain. E-mail: gonzalo.segurado.miravalles@gmail.com
Chronic ultraviolet exposure causes changes over keratinocytes, melanocytes and connective tissue of the skin on sun-exposed areas, including keratinocyte atypia, increased melanocyte density, increased epidermal melanin and, deposition of elastotic material in superficial dermis. This photodamage results in wrinkling, pigment irregularities, coarseness and skin neoplasms. Treatment with 3% diclofenac sodium w/w in hyaluronic acid is associated with an improvement in irregular pigmentation, coarseness, keratinocyte atypia and mottled pigmentation. Therefore, treatment with 3% diclofenac sodium associates an improvement in signs of photodamaged skin.
Chronic ultraviolet (UV) exposure leads to changes in keratinocytes, melanocytes and connective tissue of the skin on sun-exposed areas. These modifications include keratinocyte atypia, increased melanocyte density, increased epidermal melanin and deposition of elastotic material in the superficial dermis. This photodamage results in wrinkling, pigment irregularities, coarseness and skin neoplasms (1, 2).
Actinic keratosis (AK) is commonly treated with 3% diclofenac sodium w/w in hyaluronic acid (DSHA) (3). It has been proven to be an effective and safe therapy over the years (4). In addition, an improvement has been reported in the cosmetic appearance of the surrounding skin after treating AK (5). This is probably in relation to a decrease in photoaged skin signs.
In vivo reflectance confocal microscopy (RCM) is a non-invasive technique that enables real-time imaging of superficial layers of the skin at a quasi-histologic resolution. By means of RCM, the different skin structures can be visualised up to a depth of 300 µm, that usually encompasses the epidermis and superficial part of the dermis (6). Thus, we were able to assess these layers at a cellular level without performing an invasive biopsy. Confocal features of AK have been widely studied (6–10) and photodamaged skin and skin ageing have also been characterised (11–14). In addition, it has also turned out to be useful for monitoring the effectiveness of several treatments in AK (15–20) due to its non-invasive nature. Nevertheless, to the best of our knowledge, it has never been used in characterising the effect of a treatment on the signs of photodamaged skin.
The purpose of this study is to determine whether RCM is able to characterise the clinical changes induced by DSHA in photodamaged skin in patients with AK.
This single-centre prospective study enrolled patients with at least one clinical and dermoscopically diagnosed AK on the forehead or bald scalp and clinical signs of photodamage surrounding AK (irregular pigmentation, fine surface lines or coarseness). The study was conducted from June 2016 to October 2016. The Clinical Research Ethics Committee at Ramón y Cajal University Hospital approved this study prior to patient recruitment (Protocol Number 027/16). Written informed consent was obtained from each patient before evaluation. Exclusion criteria were contraindications for treat-ment, previous history of nonsteroidal anti-inflammatory drugs or salicylates hypersensitivity. Epidemiological data concerning sex, age, skin phototype and history of previous skin cancer were recorded for all recruited subjects.
DSHA was applied twice a day for 2 months – minimum treatment duration to obtain response – to AK and adjacent photodamaged areas. Patients were reevaluated one month after completing treatment to avoid disturbance from possible inflammation following treatment.
All patients were clinically and dermoscopically examined for the presence of AK and signs of photodamage. Clinical photographs (Canon G15, Canon, Tokyo, Japan) of the skin being treated were taken before and after treatment. Photodamage change was clinically assessed by the following signs: irregular pigmentation, fine surface lines and coarseness (19). They were graded from 0 (absence) to 3 (severe) before and after treatment. The assessment was independently performed retrospectively by two evaluators (NJG and GSM). Images before and after treatment were comparatively assessed. In case of disagreement, images were jointly assessed to come to an agreement. An overall assessment was performed, without defining an exact clinical area to assess.
RCM was evaluated with a commercially available RCM device (VivaScope 1500, MAVIG GmbH, Munich, Germany). RCM images were acquired in photodamaged skin on the forehead or bald scalp. Two evaluations on the same site were done, one prior to treatment and another one month after treatment was completed. The presence of AK in the evaluated area was ruled out clinically and dermoscopically. Four VivaBlock (image mosaic) of 6 mm X 6 mm were performed (Stratum corneum, stratum spinosum, dermo–epidermal junction and dermis); one VivaStack (images taken following a column downwards) with a step of 3.05 µm up to 121.92 µm in depth was taken from the centre of the field, to determine epidermal thickness.
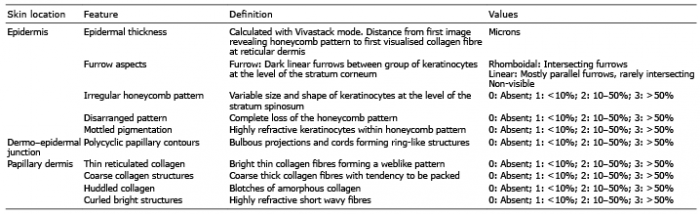
Assessment was carried out by mean of the following parameters, most of them previously used by Wurm et al. (11) and Longo et al. (12) for skin ageing. Epidermal thickness, furrows aspect, irregular honeycomb pattern and mottled pigmentation were evaluated at the epidermis. Polycyclic papillary contours were assessed at the dermo–epidermal junction level. At the papillary dermis, the morpho-logy of collagen bundles was evaluated. These parameters, their definition and values are summarised in Table I. The assessment was independently carried out retrospectively by two different evaluators (NJG and GSM). Images before and after treatment were comparatively assessed. In case of disagreement, images were jointly assessed to reach an agreement. Mean epidermal thickness value between both observers was calculated for the first and second consultations.
Table I. Confocal parameters measured, definition and possible values
Statistical analysis was performed using a statistical software package (SPSS version 24.0.0.0, SPSS Inc., Chicago, IL, USA). Cohen kappa statistics were assessed using Cohen kappa statistics and 95% confidence interval to evaluate interobserver concordance regarding clinical and confocal parameters. For this purpose, categorical variables with distributed values in more than 2 categories were summarized in only 2 categories. As for clinical descriptors, the values “absence and mild” and “moderate and severe” were respectively considered as a single category. Regarding confocal descriptors, they were adjusted as “Extension affecting less than 10%” and “Extension affecting more than 10%”.
Mean and standard deviation (SD) were measured for epidermal thickness. Statistically significant differences between measurements before and after treatment were calculated using marginal homogeneity test for categorical variables with more than 2 categories and Wilcoxon signed-rank test for continuous variables. p < 0.05 was considered statistically significant. In the case of the item “disarranged pattern”, there were insufficient valid cases to perform a statistical test. Regarding the item “coarse collagen structures”, as the values were distributed between two categories, a McNemar test was also performed.
Twenty patients were enrolled in the study, 18 men and 2 women, with a mean age of 78.4 years (range 69–87 years). Phototype II was the most common among participants (65%), followed by phototype III (20%) and I (15%). As for history of previous skin cancer, 11 patients (55%) had at least one prior episode of skin cancer. All of them (55%) had basal cell carcinoma (BCC), 3 patients (15%) malignant melanoma (MM) and 2 patients (10%) squamous cell carcinoma (SCC).
Eighteen patients completed the treatment protocol. Two patients (10%) stopped using DSHA due to a local reaction after application, consisting of moderate itching and redness when applied. In one of them symptoms arose from the first day and it was only used for 5 days. In the other patient irritation appeared after several days of treatment, and it was discontinued after two weeks. Symptoms resolved in less than a week after treatment stopped.
Regarding the clinical assessment of photoaging signs: irregular pigmentation, fine surface lines and coarseness, Table II shows the basal and post-treatment distribution of each feature including in patients who completed the treatment, and the p-value for each item.
Table II. Confocal values and p-value before and after treatment for every confocal descriptor, and interobserver agreement (K-value) for each confocal parameter and its p-value
A substantial improvement in irregular pigmentation and coarseness after treatment can be observed. For the fine surface lines item, no difference after treatment was found. The differences in irregular pigmentation and coarseness were statistically significant (p = 0.002 and 0.014 respectively). Concerning the item fine surface lines no statistically significant difference was detected (Fig. 1).
Fig. 1. Patients before (a and c) and after treatment (b and d). We may appreciate a clinical improvement due to reduction in irregular pigmentation and coarseness. Circles correspond to the areas assessed by means of reflectance confocal microscopy.
Reproducibility was tested by comparing concordance between both observers. Concordance was “good” (K = 0.61–0.80) for irregular pigmentation (K = 0.70) and fine surface lines (K = 0.66). It was “moderate” (K = 0.41–0.60) for the parameter coarseness (K = 0.58). p-value was statistically significant for all clinical items.
Regarding confocal descriptors Table II depicts the distribution of each confocal parameter before and after treatment in patients who completed the protocol. The differences before and after treatment were statistically significant for the following parameters: irregular honeycomb pattern (p = 0.001) (Fig. 2) and mottled pigmentation (p = 0.008) (Fig. 3). No statistically significant differences in the other parameters were found.
Fig. 2. Irregular honeycomb pattern before (a: 1.5 mm x 1 mm and c: 1.2 mm x 0.75 mm) and after treatment (b: 1.6 mm x 1 mm and d: –1.7 mm x 0.75 mm). A remarkable improvement after treatment may be seen. White lines correspond to 500 μm.
Fig. 3. Mottled pigmentation (red asterisks) before (a: 2 mm x 1.5 mm and c: –0.7 mm x 0.5 mm-) and after treatment (b: 2 mm x 1.5 mm and d: 0.7 mm x 0.5 mm). A reduction in pigmented keratinocytes (refractile cells) may be observed. White lines correspond to 500 μm.
Regarding concordance between observers in confocal features, it was “very good” (K = 0.81–1.00) for irregular honeycomb pattern (K = 0.82), polycyclic papillary contours (K = 0.87) and curled bright structures (K = 0.89). Reproducibility was “good” (K = 0.61–0.80) for the items mottled pigmentation (K = 0.68) and disarranged pattern (K = 0.77). Agreement was “moderate” (K = 0.41–0.60) for furrow aspect (K = 0.59), thin reticulated collagen (K = 0.50) and huddled collagen (K = 0.49). Finally, we observed “poor” (0.21–0.40) concordance in coarse collagen structures (K = 0.38).
The use of RCM as a non-invasive tool for monitoring treatment efficacy is not new. Due to its non-invasive nature, RCM enables the clinician to follow up changes in the same skin over time. In this field RCM is useful for monitoring AK (15–20) and BCC (21, 22) treatment. However, to the best of our knowledge, the dynamic changes in confocal parameters of skin photodamage after therapeutic intervention have never been reported.
Overall, our basal confocal findings are in line with previous studies that report photodamage and skin ageing (11–13). Considering the mean age of our patients and the photo-exposed site chosen, our patients have probably been affected by extrinsic and intrinsic ageing (23). Nevertheless, specific confocal descriptors for each type of skin ageing have not been clearly established. Wurm et al. (11) studied differences in confocal features according to sun exposure and age. They found fewer intersecting furrows and greater width of the furrows, honeycomb pattern irregularity, mottled pigmentation, irregularity of papillary rings, loss of thin collagen fibres and development of huddled collagen as confocal parameters of intrinsic ageing aggravated by sun exposure. We also found linear furrows as the most common type and irregular honeycomb pattern and mottled pigmentation in 95% and 85% of all patients included, respectively. Thin reticulated collagen extension was less than 10% in 90% of patients and coarse and huddled collagen were the most frequent types. Longo et al. (12) reported confocal changes on the cheek skin in different age groups. All our patients would be encompassed in age group V (> 65 years) of their study, which included 10 patients. Overall, our confocal features are in line with their findings, al-though in our 20 patients we detected a higher percentage of mottled pigmentation affecting more than 10% of the area (40% vs. 20%) and polycyclic papillary contours (55% vs. 30%) and a lower amount of curled bright fibres (80% vs. 100%). These differences could be accounted for by the small sample size in both groups, different body site of the studies or epidemiological differences between groups, since our group was mainly comprised of men (90%) and their group was constituted by women.
We appreciated a reduction in concordance between observers in relation to thin reticulated collagen, coarse collagen structures and huddled collagen. As Longo et al. (12) outlined, dermal collagen gradually degenerates over a continuum spectrum from thin reticulated collagen to coarse collagen structures and huddled collagen. Therefore, there may be some cases in photodamaged skin in which it is difficult to specify the extension of each type of collagen as they may overlap.
Global cosmetic improvement after DSHA has previously been reported (5). In line with these findings, we also noted a marked clinical improvement in irregular pigmentation, probably in accordance with the significant improvement in mottled pigmentation observed by RCM. The mechanism of action of DSHA is not fully understood; it blocks cyclo-oxygenase 2 (COX-2) reducing angiogenesis and inducing apoptosis (24). It is also known that keratinocytes release prostaglandins (PG) through PAR-2 (protease-activated receptor 2), promoting melanocyte dendricity and transfer of melanosomes to keratinocytes (25). COX has also been implicated in the PAR-2 pathway (26). We hypothesise that COX inhibition of DSHA (24) over keratinocytes would reduce PG release mediated through PAR-2, thus decreasing PG-induced melanocyte dendricity and, consequently, reducing transfer of melanin to keratinocytes, which would decrease mottled pigmentation in RCM exploration corresponding to a decreased pigmentation of epidermal keratinocytes. However, further studies are needed to confirm this hypothesis.
The improvement in the coarseness of the skin may be accounted for by the active substance (DSHA) or by the hydration associated with the medicine vehicle (hyaluronic acid). Studies comparing drug and vehicle would be needed to elucidate this.
Concerning the significant reduction in honeycomb irregularity, Malvehy et al (16) previously reported a significant decrease in atypia of the honeycomb pattern in clinical and subclinical AK following DSHA treatment. They also reported an improvement in dermal collagen in terms of replacement of huddles of collagen and curled fibres by aligned thinner fibres secondary to DSHA that we have not observed. This could be accounted for by the shorter duration of treatment in our study, since changes in dermal collagen may take longer. Confocal differences between subclinical AK (cancerisation field) and photodamaged skin is moot. For some authors (15, 16), subclinical AK is defined as the finding of confocal features of AK, mainly atypical honeycomb pattern, without visible clinical lesion. In both studies (15, 16) subclinical AK was found surrounding AK. However, atypical honeycomb pattern and even epidermal disarray have been reported in a considerable percentage of patients in photodamaged and aged skin by other authors (11–14). According to the subclinical AK definition (15, 16), one could argue that in our study we have dealt with subclinical AK instead of photodamaged skin, as irregular honeycomb pattern was observed in most of our patients. However, we have also appreciated other accompanying confocal features, such as linear furrow pattern, mottled pigmentation and polycyclic papillary contours, which are more defining features of photodamaged and aged skin rather than AK. According to the literature (11–16), we propose to take other confocal parameters into account such as furrow aspect, mottled pigmentation and irregularity of papillary rings, in addition to irregular honeycomb pattern when considering classification of normally appearing skin with irregular honeycomb pattern as photodamaged or subclinical AK.
Limitations of our study are the small sample size, the absence of a control group, the inability of RCM to assess changes in the reticular dermis, absence of histopathological correlation. Readers were not blinded for images corresponding to before and after treatment.
In conclusion, RCM is a valuable tool for monitoring treatment effects on signs of photodamaged skin. In addition, the use of DSHA for photodamaged skin leads to an improvement in clinical irregular pigmentation and coarseness and reduces irregular honeycomb pattern and mottled pigmentation in the epidermis.
Funding sources: This study was partially funded by Almirall S.A.
Conflict of interest: GSM and OMM-A have been remunerated by Almirall for attending national conferences. NJG has been paid as a consultant by Almirall on issues unrelated to the study product. IAS worked as a scientific advisor for Almirall.


 Click to show fullsize
Click to show fullsize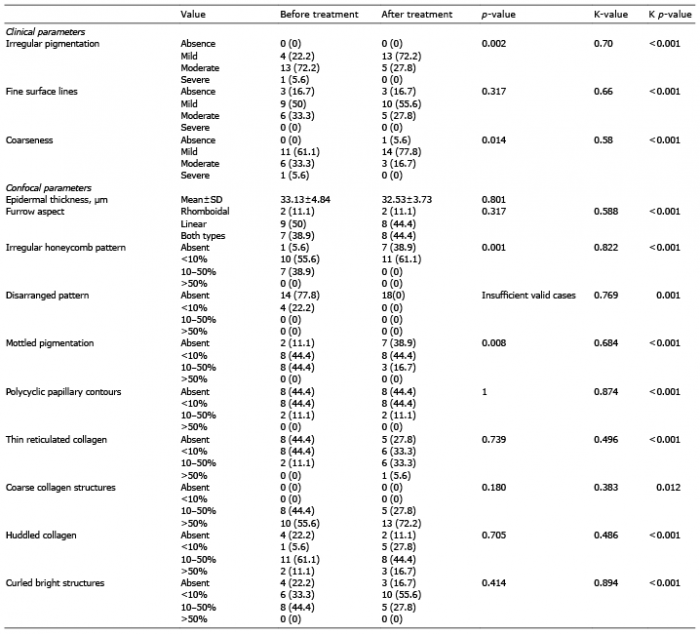 Click to show fullsize
Click to show fullsize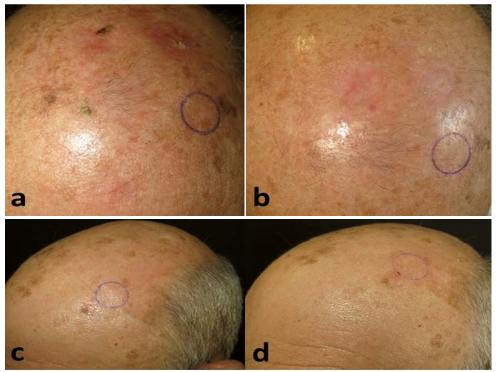 Click to show fullsize
Click to show fullsize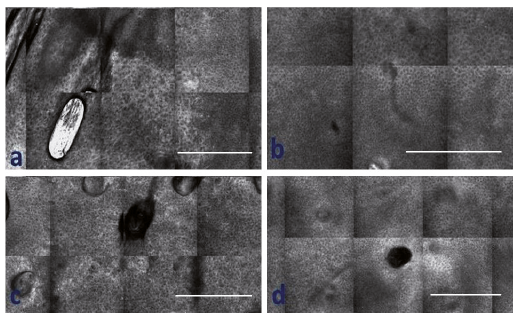 Click to show fullsize
Click to show fullsize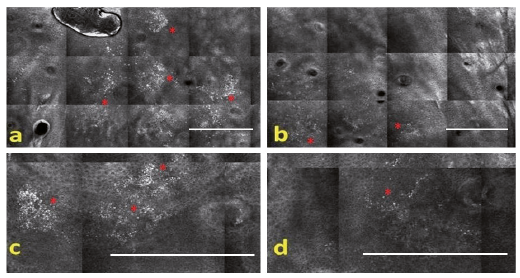 Click to show fullsize
Click to show fullsize