


1Department of Dermatology, Kyoto University Graduate School of Medicine, 54 Shogoin-Kawahara, Sakyo, Kyoto 606-8507, and 2Department of Diagnostic Pathology, Kyoto University Hospital, Kyoto, Japan. *E-mail: hontetsu@kuhp.kyoto-u.ac.jp
Accepted Jun 14, 2018; Epub ahead of print Ju 25, 2018
Pityriasis rubra pilaris (PRP) is an inflammatory skin condition characterized by well-circumscribed hyperkeratotic plaques and palmoplantar keratoderma (1). The aetiology of PRP is unclear and although various treatment options, such as topical steroids and oral retinoic acids, are available, treatment responses are inconsistent and management is often difficult (2). We report here a case of PRP that was treated successfully with apremilast, a phosphodiesterase-4 (PDE4) inhibitor. Furthermore, using immunohistochemistry we examined the expression of nuclear factor of kappa light chain enhancer in B cells (NF-κB) and caspase recruitment domain family, member 14 (CARD14), a molecule that induces activation of NF-κB and is reported to be involved in the pathogenesis of PRP in the skin.
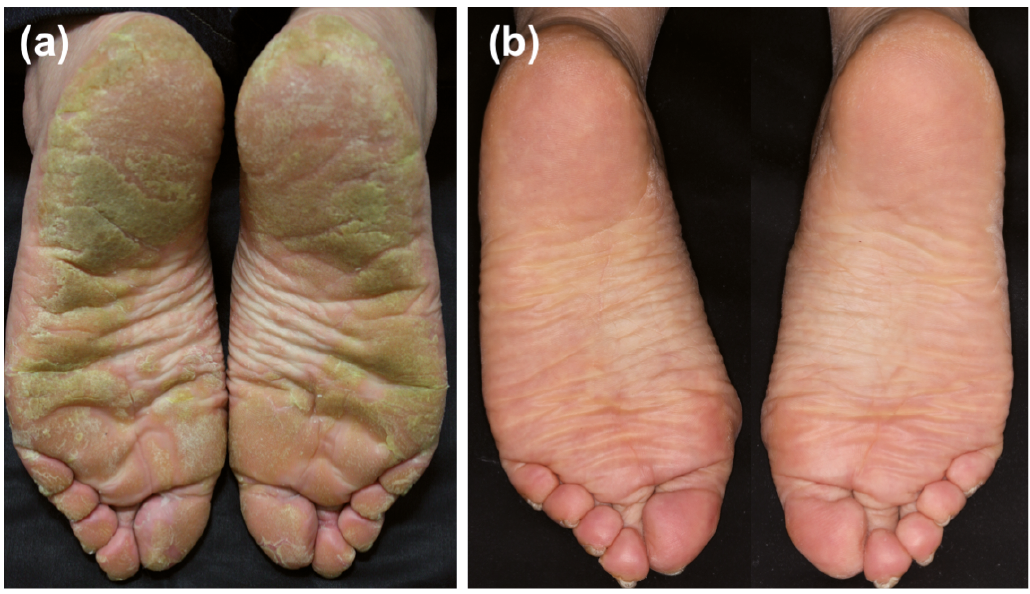
A 60-year-old woman with no significant medical or family history attended our clinic 4 years ago with a 1-month history of well-demarcated, pruritic erythema keratodes on the hands, soles of the feet, elbows, and knees (Fig. 1a). Keratinizing papules on the palms, and scales on the dorsa of the hands and nail beds, were also seen. No nail-fold capillary abnormalities or nail changes were evident, and she had no systemic symptoms. Skin biopsy at initial presentation showed a “chequerboard pattern” of alternating parakeratosis and orthokeratosis, irregularly elongated rete ridges, acantholysis, and dermal melanin incontinence (Fig. 2a). Based on the clinical and histological findings, she was diagnosed with type I PRP. She developed mild arthralgia 5 months later and was referred to the rheumatology department. Her autoantibody screening showed an elevated anti-centromere antibody and limited cutaneous systemic sclerosis was diagnosed, but no additional treatments were started by the rheumatologists. Over the following 4 years all strengths of topical steroid ointments, topical vitamin D3 analogues and salicylic acid, oral retinoic acid, and phototherapy were tried. Other treatments, such as methotrexate, were not considered due to possible side-effects. Although mild improvements were seen throughout the treatment period, the skin lesions always recurred and never completely resolved. As the symptoms were refractory, our treatment options were limited and we decided to start apremilast at 30 mg/day. Although no substantial changes in the hyperkeratosis of the feet were seen one month after the introduction of apremilast, significant improvements were seen after 2 months. Currently, the skin lesions have not shown any recurrence at 6 months of treatment with apremilast (Fig. 1b) and the patient has only experienced mild headaches, a common adverse event associated with apremilast, which was manageable with oral analgesia.
As apremilast is thought to suppress the activation of NF-κB, a transcriptional factor that induces various inflammatory mediators, and as recent studies have shown that the expression of CARD14, an important molecule for NF-κB activation, in keratinocytes is upregulated in PRP (3), we investigated the expressions of these factors in our patient. Immunohistochemistry was performed on the formaldehyde-fixed skin samples of the biopsy taken at the initial presentation, with antibodies against p65 (Cell Signaling Technology, #8242), a component of NF-κB, and CARD14 (SIGMA, HPA023388). Both p65 and CARD14 were only marginally expressed in the nucleus of keratinocytes in our patient (Fig. 2b, c). How-ever, their expressions were more concentrated around inflammatory cells surrounding the dermal vasculature (Fig. 2b, c).
Fig. 1. Clinical presentation of pityriasis rubra pilaris before and after treatment with apremilast. (a) Keratinization and erythema were seen on both feet and knees at initial presentation. (b) Significant improvements in the skin lesions were seen at 6 months after the start of treatment with apremilast.
Fig. 2. Histological presentation and immunohistochemical staining of pityriasis rubra pilaris for p65 and CARD14. (a) Haematoxylin and eosin staining of the skin biopsy shows the classic “chequerboard appearance” of alternating parakeratosis and orthokeratosis (original magnification ×5; scale bar=500 mm). (b) Skin biopsy stained for p65 shows nuclear staining in keratinocytes (white circle) and in inflammatory cells surrounding the vasculature (black square). (original magnification ×10; scale bar=250 mm). (c) Skin biopsy stained for CARD14. Weak expressions of CARD14 were seen in keratinocytes (white circle) and in dermal inflammatory cells around vessels (black square) (original magnification ×10; scale bar=250 mm).
Apremilast is an oral PDE4 inhibitor that is currently a treatment option for psoriasis and psoriatic arthritis (4). The mode of action of apremilast is considered to be the upregulation of intracellular cyclic adenosine mono-phosphate (cAMP) and thereby the suppression of NF-κB (4). Various types of cells, including keratinocytes, are regarded as targets of apremilast (5, 6).
Although the aetiology of PRP remains unclear, excess activation of CARD14 and NF-κB in keratinocytes is suggested as a possible pathological mechanism. Mutations in CARD14 are associated with hereditary forms of PRP (7), and such mutations result in the activation of NF-κB and therefore the upregulation of inflammatory cytokines in keratinocytes (8). Recent studies have also shown an increase in CARD14 and NF-κB (p65) expressions in keratinocytes in sporadic cases of PRP (3). Therefore, we initially hypothesized that CARD14 and p65 were also upregulated in the keratinocytes of our patient. However, immunohistochemistry staining showed that both CARD14 and p65 stained mainly in the nucleus of the dermal inflammatory cells rather than in keratinocytes. Therefore, in our patient, the activation of CARD14 and NF-κB in the dermal inflammatory cells may have been the main pathological mechanism for the skin inflammation. Indeed, a recent report indicates that CARD14 in the dermal inflammatory cells is essential in the development of psoriatic inflammation in mice (9). The activation of CARD14, not only in keratinocytes, but also in the dermal inflammatory cells, may play an important role in the pathogenesis of PRP. Apremilast may therefore exert its actions by inhibiting the activation of both keratinocytes and inflammatory cells in PRP.
Finding a successful treatment for PRP is often challenging in spite of the various treatment options currently available. While classical PRP is known to spontaneously regress, the timing of its resolution coinciding with the start of apremilast in our case suggests that apremilast may be effective in PRP. In keeping with our case, 2 previous cases of sporadic PRP were treated successfully with apremilast (10, 11). In both cases, significant improvements were evident shortly after the start of treatment with apremilast and no recurrence has been seen (10, 11). PDE4 inhibitors may therefore be considered as a new management option in cases of PRP that are resistant to mainstay treatments, such as steroids, vitamin D3 analogues, salicylic acid, and retinoids.
The authors thank Dr Mayuri Tanaka and Dr Ken J. Ishii (National Institutes of Biomedical Innovation, Health and Nutrition, Osaka, Japan) for technical support.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize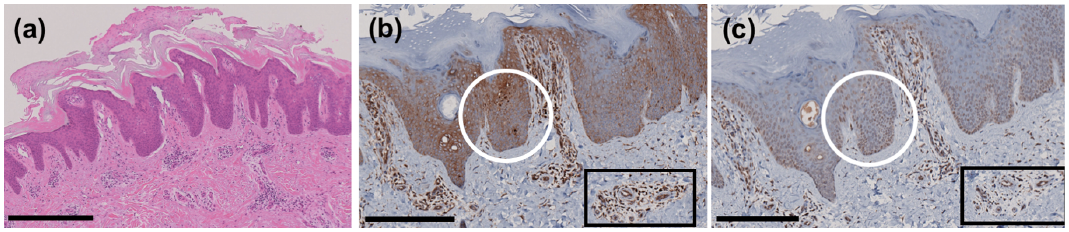 Click to show fullsize
Click to show fullsize