


1Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, 12 Jiangwangmiao Road, Nanjing, 210042, Jiangsu, Departments of Dermatology: 2Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, Jiangsu, 3Affiliated Zhongshan Hospital of Fudan University, Shanghai, China and 4The University of Texas MD Anderson Cancer Center, Houston, USA, and 5Jiangsu Key Laboratory of Molecular Biology for Skin Diseases and STIs, Nanjing, Jiangsu, China. *E-mail:fangmin5758@aliyun.com
#These authors contributed equally to this work.
Accepted Jun 26, 2018; Epub ahead of print Jun 29, 2018
The co-existence of 2 different types of lymphoma in a single patient is rare. We report here a case of secondary cutaneous Epstein–Barr virus (EBV)-associated diffuse large B-cell lymphoma (DLBCL) with Hodgkin/Reed-Sternberg-like (HRS-L) cells that developed in a patient with lymph node angioimmunoblastic T-cell lymphoma (AITL).
A 49-year-old Chinese woman presented with enlarged left cervical lymph nodes for 2 months in September 2010. She had no visible lesions on her skin. Computed tomography (CT) revealed enlarged bilateral cervical lymph nodes and hepatosplenomegaly. Lymph node biopsy revealed that the normal lymph node architecture was destroyed by small- to medium-sized lymphoid cells with clear cytoplasm and mildly irregular nuclei (Fig. 1A). Plasma cells, eosinophils and scattered large immunoblast-like lymphoid cells were observed. Those small- to medium-sized lymphoid cells were positive for CD3, CD4, CD10, PD-1, and CXCL-13, but negative for CD20 and CD30. The scattered large immunoblast-like cells were positive for CD20 and weakly positive for CD30. The proliferation of follicular dendritic cells was highlighted by CD21 and CD23 staining. No EBER-positive cells were observed on an in situ hybridization assay. A diagnosis of AITL was made according to World Health Organization (WHO) classification criteria (1). The patient received 6 cycles of chemotherapy with CHOP regimen (cyclophosphamide, doxyrubin, vincristine, prednisone), which led to complete remission. She was followed-up for 21 months without treatment, with no further symptoms.
In June 2012, the patient developed multiple plaques and nodules, with ulcers on her trunk and extremities (Fig. 1B). The lesions had nodal and perivascular proliferation of small- to medium-sized lymphocytes in the dermal and upper subcutis, with scattered large-sized atypical lymphoid cells. The small- to medium-sized lymphocytes were positive for CD3 and CD4, but negative for CD10, CD20, PD-1 and CXCL-13. The large atypical cells were positive for CD20 and weakly positive for CD30, and negative for CD3, CD4 and CD10. The patient was diagnosed with cutaneous lymphoid atypical proliferation.
After diagnosis, the patient was treated with prednisone, 30 mg/day for 3 weeks, and most of the lesions disappeared. However, one nodule on the chest persisted and enlarged after 2 months. A second biopsy of the chest nodule revealed diffuse proliferation of medium-to-large-sized atypical lymphoid cells in the dermal and subcutis, mixed with numbers of HRS-L large cells (Fig. 1C, D). The medium-to-large-sized cells expressed CD20 (Fig. 1E), CD79a, Bcl-2, Bcl-6 and MUM-1. The HRS-L cells expressed CD20 in varying degrees (Fig. 1F). Both of the populations of cells were negative for CD3, CD5 and CD10. In addition, the HRS-L cells were positive for CD30 (Fig. 1G), but not for CD15 and ALK. EBER were positive in 2 populations of cells. Based on these findings, a diagnosis of EBV+DLBCL was made.
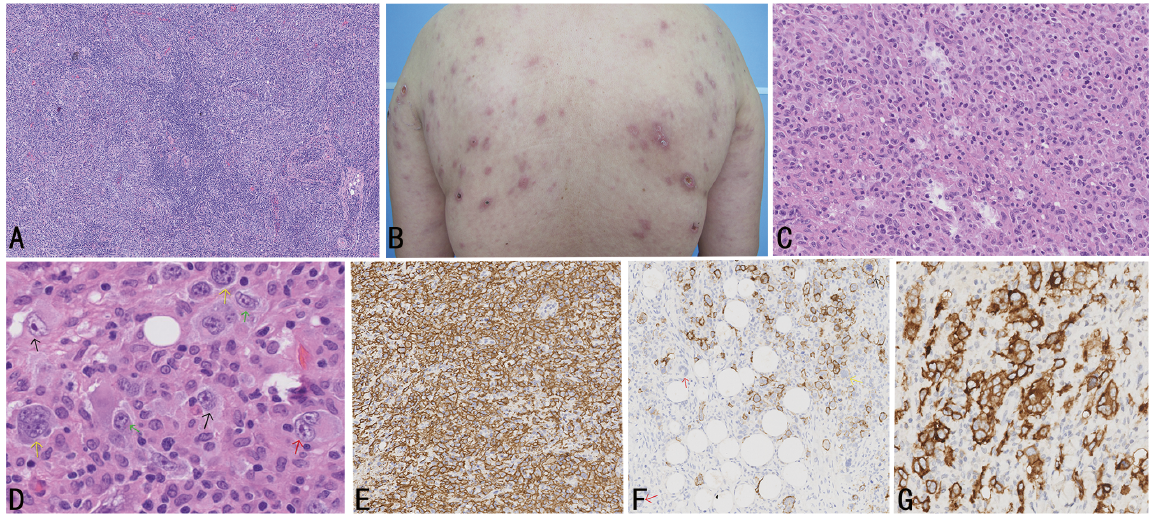
Fig. 1. (A) Lymph node biopsy revealed that the normal architecture of the lymph node was destroyed by small- to medium-sized lymphoid cells with clear cytoplasm and mildly irregular nuclei. There was marked proliferation of high endothelial venules (haematoxylin and eosin (H&E), ×20). (B) Multiple plaques and nodules with ulcers and crusts on the back. (C) Tumour cells diffusely infiltrated in the dermis (H&E ×5). (D) Large polygonal cells, resembling Hodgkin/Reed-Sternberg-like (HRS-L) large binuclear cells (red arrows) and mononuclear cells (black arrows) or hallmark cells of anaplastic cell lymphoma (green arrows). Some cells have bizarre pleomorphic nuclei (yellow arrows) (H&E ×80). (E) Immunohistochemical staining showed that the medium- to large-sized cells expressed CD20 (×40). (F) Immunohistochemical staining showed that the HRS-L cells were positive for CD20 to varying degrees (black arrow: strong; red arrows: negative; yellow: mild) (×40). (G) Immunohistochemical staining showed that the HRS-L cells were positive for CD30 (×40).
After reviewing all 3 biopsies, scattered atypical large-sized cells were found in the first skin biopsy. These cells weakly expressed CD20 and CD30, and were positive for EBER. The patient was finally diagnosed with AITL with secondary cutaneous EBV-associated DLBCL with a HRS-L cell component. The patient underwent 4 cycles of chemotherapy with RCHOP regimen (rituximab CHOP) and the skin lesions disappeared completely. However, 5 months later the patient died of pancytopaenia and invasive fungal pneumonia.
The co-existence of 2 types of lymphoma in a single patient is very rare. The co-occurrence of T- and B-cell lymphoma in the same organ or tissues has been termed “composite lymphoma” (2). Other cases of an inimical lymphoma with subsequent development of a second lymphoma have been described previously (Table SI). Among these rare cases, AITL and DLBCL are the most common types of T- and B-cell lymphoma, respectively.
Most AITL showed scattered EBV-infected B lymphocytes (3), which suggests that AITL may be associated with a profound immune deficiency. Although the pathogenesis of EBV-associated DLBCL in the setting of AITL remains unclear, it is thought that the immune dysregulation presenting and pronounced by chemotherapy in AITL may result in the reactivation of EBV, which could play a role in the proliferation and transformation of B cells into immortalized EBV-infected B-cell clones. However, similar to previous reports (3–5), EBV-infected B lymphocytes were not found in the AITL component in our case. These findings suggest that the EBV infection may be transient in the pathogenesis of DLBCL. Further research is required to elucidate the mechanism involved in DLBCL derived from non-EBV-infected B cells of ALTL.
The histological features of cutaneous AITL were categorized by Martel et al. (6) into 4 patterns. However, to the best of our knowledge, the histological features found in our first skin biopsy, which was similar to the lymph node affected by AITL with EBV-associated HRS-L B-cells proliferation (5), have not been recorded previously in cutaneous AITL (6). Hoffmann et al. (3) found a significantly higher frequency of HRS-L cells in patients with composite AITL and DLBCL compared with cases of AITL with or without proliferation of associated B-cells, but not DLBCL. The EBV-positive rate was also higher in the former patients. The second skin biopsy of our patient also revealed a significantly increased number of HRS-L cells. These findings of EBV-associated HRS-L cells in DLBCL developed in AITL not only showed the gradual progression of the disease, but also support the specific role of EBV infection in B-cell transformation and proliferation.
Ten cases of DLBCL developed in extranodal organs have been reported, including skin (7), soft tissue (8), bone marrow (9), ileum (10), adrenal gland (11), duodenal bulbous and lung (12). From the available published data (Table SI), compared with the patients with secondary DLBCL in lymph nodes, patients with extranodal involvement have a lower survival rate (57% (4/7) vs. 20% (2/10)), which suggests that patients with DLBCL with involvement of extranodal organs may have a poor prognosis.
However, evidence from more cases is needed to elucidate this involvement.
This work was funded by CAMS Innovation Fund for Medical Sciences (CIFMS-2017-12M-1-017) and Peking Union Medical College Youth Fund (3332017168).


 Click to show fullsize
Click to show fullsize