


1Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, 12 Jiangwangmiao St., Nanjing 210042, Jiangsu, and 2Jiangsu Key Laboratory of Molecular Biology for Skin Diseases and STIs, St. Nanjing, Jiangsu, China. *E-mail: whs33@vip.sina.com
#These authors contributed equally.
Accepted Jul 27, 2018; Epub ahead of print Aug 7, 2018
Detection of pathogens in skin infections caused by mycobacteria is difficult. Interferon-gamma release assay (IGRA), a preferred method for the diagnosis of latent tuberculosis infection (LTBI), has shown the capacity to detect mycobacterial infections (1–4). IGRAs have higher specificity over the tuberculin skin test, as they are based on Mycobacterium tuberculosis antigens encoded on RD1 (secretory antigen target 6 and culture filtrate protein 10). RD1 is absent in Bacillus Calmette–Guérin (BCG) and most environmental mycobacteria. However, a high degree of similarity was found in both the amino-acid sequences and the gene sequences encoding the RD1 antigens of M. tuberculosis and various other mycobacteria, i.e. M. marinum, M. szulgai, M. kansasii, and M. gordonae (1, 5–7).
The aim of this study was to prospectively explore the diagnostic value of the T-SPOT.TB test (Oxford Immunotec Ltd., Abingdon, UK), a representative IGRA, in cutaneous infections with RD1-possessing mycobacteria, including M. tuberculosis and RD1-possessing nontuberculous mycobacteria (NTM). Furthermore, we evaluated the changes in T-SPOT.TB test results after antibiotic treatment.
Between July 1, 2015 and December 30, 2017, we conducted the study at the Institute of Dermatology, Chinese Academy of Medical Sciences. All clinically suspected cases of cutaneous tuberculosis or NTM infections were screened prospectively. Ethics approval (2012-KY/LC-021) was obtained from our ethics committees. Informed consent was obtained from the participants.
There is currently no diagnostic method regarded as the gold standard for diagnosis of cutaneous tuberculosis, cutaneous infection of NTM and cutaneous fungal infection, so all eligible subjects were diagnosed with these diseases based on the following criteria: 1) chronic skin lesions, 2) pathology showing infectious granulomas, 3) molecular biological methods for the culture organism or biopsy samples confirming the corresponding disease.
Patients who met the following conditions were excluded: 1) having active tuberculosis of any organ except the skin; 2) having a history of anti-mycobacterium antibiotic treatment; 3) being ruled out by pathology; 4) refusing to participate.
Peripheral venous blood was collected for T-SPOT.TB test before treatment. Subjects in the group of cutaneous infection of RD1-possessing mycobacteria were followed up on every two months, and after 6 months of antibiotic therapy, they were further reevaluated using T-SPOT.TB test. Treatment of cutaneous tuberculosis followed the recommended guidelines by the WHO, which consist of an intensive phase for 2 months (isoniazid, rifampicin, ethambutol, and pyrazinamide) followed by a maintenance phase for 4 months (isoniazid and rifampicin) (8). Treatment for cutaneous NTM infection was designed based on drug susceptibility tests. For those who did not participate in such tests, we utilized empiric antibiotic therapies.
The procedure of T-SPOT.TB followed the manufacturer’s guidelines. The high spot numbers of Panel A minus Nil Control (PA) and Panel B minus Nil Control (PB) were recorded as spot forming cells (SFCs). Molecular biological methods were based on PCR and sequencing of the 16S rRNA and hsp65 genes (9). Homology analyses were conducted to define the strain.
Continuous variables were summarized using mean (standard deviation) for normally distributed data and using median (interquartile range (IQR)) for non-normally distributed data. The difference in age between groups was assessed by Mann–Whitney test. The differences in sex, underlying conditions, trauma history and HIV status were assessed by Chi-squared test. Positivity rates across groups were compared using Chi-squared tests. The median SFCs among groups were compared by Kruskal–Wallis test. Changes in positivity rates and SFCs before and after therapy were determined by McNemar’ test and Wilicoxon rank sum test, respectively. Statistical significance was considered as p < 0.05. Statistical analyses were performed using IBM SPSS 19.0.
A total of 293 clinically suspected cases of cutaneous mycobacterial infection were screened for the study (Fig. S1). A total of 64 participants were eligible. Among them, 46 (71.9%) were classified as cutaneous infection of RD1-possessing mycobacterium, 8 (12.5%) as cutaneous infection of RD1-negative NTM, and 10 (15.6%) as cutaneous fungal diseases. The basic characteristics of the 64 participants are shown in Table SI. Forty (87.0%) of 46 cutaneous infections with RD1-possessing mycobacterium cases tested positive for T-SPOT.TB, which was much higher than those with RD1-negative NTM and fungal infections (Both 0%) (p = 0.000). The sensitivity in cutaneous tuberculosis and cutaneous infections of RD1-possessing NTM were 95.8% and 72.7%, respectively (p = 0.090) (Table SII).
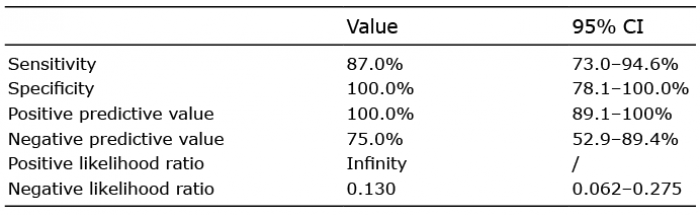
The diagnostic performance of the T-SPOT.TB test in cutaneous infections of RD1-possessing mycobacteria is shown in Table I. Median SFCs in cutaneous infection of M. tuberculosis, RD1-possessing NTM, and RD1-negative NTM before anti-mycobacterium therapy were 23.5 (IQR 10.5–54.0), 14.0 (IQR 6.5–33.8) and 0.0 (IQR 0.0–1.5), respectively (Fig. S2) (p = 0.000).
Table I. Diagnostic performance of T-SPOT.TB in cutaneous infections of RD1-possessing mycobacterium
All patients responded well. In the 42 patients (91.3%) who finished the study, the positive rate decreased from 95.5% to 59.1% (p = 0.008) in cutaneous tuberculosis and from 75.0% to 45.0% in RD1-posessing NTM (p = 0.031) after therapy (Table SIII). Quantitative results of T-SPOT.TB in the 42 patients showed that most cases had reduction of PA or PB after treatment (Fig. S3). The median number of SFCs also fell significantly after treatment (Table SIII).
Previous reports have suggested that IGRAs show positive results for infection by NTMs such as M. marinum, M. kansasii, and M. gordonae (1–4). In the present study, we found that cutaneous tuberculosis and RD1-posesssing NTM infections also lead to positive T-SPOT.TB test results. Further, 87% of cutaneous infections by RD1-possessing mycobacteria but 0% of those by RD1-negative mycobacteria tested positive using the T-SPOT.TB test, which could potentially be used to differentiate these infections. Cutaneous tuberculosis and M. marinum infection are the two most common cutaneous mycobacterial diseases in China. Notably, a positive T-SPOT.TB result is a reliable indicator of the above infections, but a negative result does not rule them out.
Previous studies on the role of T-SPOT.TB in monitoring therapy have yielded varying results. We believe that this was due to significant heterogeneity between populations, methods, and study designs. All eligible cases in our study were microbiologically confirmed, thus minimizing bias brought about by uncertain cases. Despite a lack of comparability between different individuals, we found that a majority of patient SFC levels decreased after treatment, thus potentially providing a way to monitor therapeutic efficacy.
LTBI is usually diagnosed using IGRAs when no clinical or microbiological evidence of active tuberculosis can be found (10). However, we suggest that not only cutaneous tuberculosis but also RD1-possessing NTM infections should be excluded before using T-SPOT.TB test for the diagnosis of LTBI, particularly in areas with high prevalence of cutaneous infections of RD1-possessing mycobacteria. For example, areas along the river or sea, such as those found in Eastern Asia, have high numbers of skin infections caused by M. marinum (11–13). A number of such infections can be latent or transient while still testing positive under the T-SPOT.TB test, thus causing false-positives.
The present study certainly has limitations. The first is the limited size of the sample. This is due to limitations in current diagnostic methods, which make the diagnosis of cutaneous mycobacterial infections difficult. The second limitation is that cases of M. kansasii, M. gordonae, and M. szulgai infection were low in number, so use of T-SPOT.TB tests for the detection of all RD1-possessing NTM infections requires further study.
We thank Lemuel Shui-Lun Tsang for editing the manuscript. We thank the colleagues at the Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College for their work in sample processing.
This work was supported by grants from CAMS Innovation Fund for Medical Sciences [grant number 2016-I2M-1-005, 2017-I2M-B&R-14], Natural Science Foundation of China [grant number 81371751)], and Jiangsu Provincial Natural Science Foundation [grant number BK20141065].
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize