


1Harvard Medical School and Beth Israel Deaconess Hospital, Boston, Massachusetts, USA, 2Department of Dermatology, Faculty of Health Sciences, University Hospital of North Norway, 3Institute of Clinical Medicine, Arctic University, Tromsø, Norway, 4AbbVie Inc., North Chicago, Illinois, and 5Fort HealthCare, Fort Atkinson, Wisconsin, USA
Hidradenitis Suppurativa Clinical Response (HiSCR), is a validated tool that has been used to assess the efficacy of adalimumab among patients with hidradenitis suppurativa. We evaluated the clinical meaning of HiSCR by relating it to patient-reported outcomes to give further context to its achievement in a post hoc analysis of integrated data from two phase 3 clinical trials (PIONEER I and II). Pooling placebo and active treatment arms, 39% of patients (245/629) achieved HiSCR at week 12. Irrespective of treatment, significantly (p < 0.05) more HiSCR responders than non-responders experienced clinically meaningful improvement in Dermatology Life Quality Index (60.5% vs 30.4%), Pain Numeric Rating Scale (46.9% vs 19.9%), hidradenitis suppurativa quality of life (49.4% vs 26.9%), work-related performance (52.6% vs 37.7%), and non-work-related performance (59.5% vs 33.3%). Clinically meaningful outcomes in hidradenitis suppurativa are more likely to be attained in patients achieving HiSCR level improvement.
Key words: abscess; inflammatory nodule; DLQI; PIONEER I; PIONEER II; minimum clinically important difference.
Accepted Jul 27, 2018; Epub ahed of print Aug 7, 2018
Acta Derm Venereol
Corr: Brian M. Calimlim, DrPH, MS, Dept GMH1, AbbVie Inc., 1 N Waukegan
Road, North Chicago, IL 60064, USA. E-mail: brian.calimlim@abbvie.com
Hidradenitis suppurativa is a chronic skin disease characterized by inflammation and deep-seated lesions. The hidradenitis suppurativa clinical response (called HiSCR) is a straightforward and well-validated tool designed to assess treatment response. It is based on the counts of easily recognizable clinical signs of hidradenitis suppurativa, including inflammatory nodules, abscesses, and draining fistulas. This study verifies that the HiSCR is a reliable tool for assessing clinically meaningful improvements in inflammatory signs and symptoms of hidradenitis suppurativa and improving health outcomes from the patient’s perspective. Given these characteristics, the HiSCR is appropriate for use in clinical trials and clinical care.
Hidradenitis suppurativa (HS), or acne inversa, is a chronic skin disease characterized by recurrent inflammation and deep?seated lesions in apocrine gland?bearing, intertriginous areas of the body (1–3). The reported prevalence of HS varies widely from 0.03% to 8%, depending on the setting and methodology used (4), but may be underreported, as the average time from first symptoms to diagnosis is 7 years (5). HS can cause scarring and disability (6, 7) and substantially affects patient health-related quality of life (HRQL) outcomes (8–11). Available clinical measures for assessing HS disease severity include Hurley stage, modified Sartorius score, and the HS Physician’s Global Assessment (12–15); however, none of these measures have been validated in depth regarding clinical and patient relevance and impact.
HS clinical response (HiSCR) (16) is a validated tool that has been used to assess treatment efficacy in clinical trials. HiSCR is designed to be a practical measure and is based on counts of easily recognizable clinical signs, including inflammatory nodules, abscesses, and draining fistulas. The HiSCR was designed based on data from a phase 2 clinical trial in patients with HS and retrospectively tested in that data set (16, 17). Phase 3 clinical trials (PIONEER I and II) (18) assessing the effect of adalimumab (ADA) on HS subsequently used HiSCR as a measure of treatment response and ultimately led to approval by the US Food and Drug Administration (FDA) for the treatment of moderate to severe HS in adult patients, and by the European Medicines Agency (EMA) for the treatment of active moderate to severe HS in adult patients who have failed to respond to conventional systemic therapies.
A recent systematic review (19) of HS outcome measures concluded that good-quality validation evidence is available for the HiSCR instrument, making HiSCR an appropriate tool to use to assess anti-inflammatory treatment effect in HS. The Ingram review (19) noted that evidence of association between HiSCR and minimum clinically important difference (MCID) in various outcomes was lacking. Therefore, the objective of this post hoc analysis was to further validate and assess the association of HiSCR with manifestations of HS commonly seen in the clinical setting and measures of HRQL, irrespective of treatment in combined data from two phase 3 randomized, controlled, double-blind trials (PIONEER I and II) and to provide new evidence on the association of MCID with patient-reported outcomes (PROs) and the attainment of HiSCR.
Data were combined from two phase 3 trials (PIONEER I [NCT01468207] and PIONEER II [NCT01468233]) that evaluated the efficacy and safety of ADA versus placebo in patients with moderate to severe HS. The two studies were conducted in accordance with the International Conference on Harmonisation guidelines, applicable regulations, and the principles of the Declaration of Helsinki. The study protocols were approved by the independent ethics committee or institutional review board at each study site. All patients provided written informed consent before enrollment. This post hoc analysis included data from the first 12 weeks of both studies in which patients were randomly assigned (1:1) to either ADA or placebo. The ADA dosing schedule was 160 mg at week 0, 80 mg at week 2, and 40 mg weekly at weeks 4 to 12.
Complete details of the eligibility requirements for the PIONEER I and II trials have been published (18). Briefly, adults with ≥ 1-year history of stable, moderate to severe HS were eligible to participate in these two trials if they had a total abscess and inflammatory nodule count (AN count) ≥ 3 at baseline, HS lesions in ≥ 2 distinct body areas, and Hurley Stage II or III in ≥ 1 area.
Patients were seen in clinic at baseline and at weeks 2, 4, 8, and 12 and the following assessments were performed: lesion counts and Hurley staging, physical examination, vital sign measurements, and laboratory tests. The primary endpoint in both studies was the proportion of patients achieving HiSCR (responders) at 12 weeks. HiSCR was defined as ≥ 50% reduction in AN count and no increase in number of abscesses or draining fistulas compared with baseline. Secondary endpoints included changes from baseline to week 12 in AN counts; the number of HS lesions, including abscesses, inflammatory nodules, and draining fistulas; modified Sartorius score; and high-sensitivity C-reactive protein (hs-CRP).
The Dermatology Life Quality Index (DLQI) is a validated questionnaire (20) used to assess skin symptoms and the impact of skin problems on quality of life. The DLQI is scaled from 0 to 30 points, with higher scores indicative of a greater impact of HS on the patient’s life. The MCID for DLQI was defined as at least a 5-unit decrease (21); MCID analyses were conducted among patients with baseline DLQI ≥ 5.
The Patient’s Global Assessment of Skin Pain Numeric Rating Scale (Pain NRS) is an 11-point numerical rating scale ranging from 0 (no skin pain) to 10 (skin pain as bad as you can imagine). Higher scores are indicative of a greater impact of HS on the patient’s life. This study analyzed the worst skin pain reported in the 7 days just before the time point of interest. MCID for pain was defined as a ≥ 30% (22) reduction relative to a patient’s baseline score and at least a 1-unit reduction from baseline. MCID analyses were conducted among patients with a baseline score ≥ 3.
HS quality of life (HSQL) was rated on an 11-point numerical rating scale from 0 (worst possible) to 10 (best possible). Lower scores are indicative of greater impact of HS on the patient’s life; MCID was defined as one half standard deviation (SD) of the total population’s baseline score (23). MCID analyses were conducted among those with a baseline HSQL of at most 10 minus one half SD.
The Work Productivity and Activity Impairment (WPAI) questionnaire is a validated instrument (24) that evaluates 4 areas: work time missed because of HS (absenteeism), impairment while working because of HS (presenteeism), overall work impairment because of HS, and impairment of daily activities because of HS (activity impairment). WPAI is scaled from 0% to 100%, with higher scores indicative of a greater impact of HS on the patient’s life. MCID was defined as one half SD of the total population’s baseline score (23). MCID analyses were conducted among those with a baseline score of at least one half SD.
The Treatment Satisfaction Questionnaire for Medication (TSQM) is a validated tool (25) that includes assessments of the patient’s satisfaction with a medication’s effectiveness, lack of side effects, convenience, and global satisfaction with the medication. The TSQM is scaled from 0 to 100 points, with lower scores indicative of a greater dissatisfaction. MCID was defined as one half SD of the total population’s baseline score (23). MCID analyses were conducted among those with a baseline score of at most 100 minus one half SD.
All randomized patients were included in the integrated analyses. Differences in clinical assessment measures (AN count, lesion count, modified Sartorius score, and hs-CRP level) and PROs (DLQI, Pain NRS, WPAI, TSQM, and HSQL) between HiSCR responders and non-responders were calculated using least squares (LS) means and analysis of covariance. Missing data were imputed using last observation carried forward (LOCF).
The percentage of patients who attained the MCID was determined for each of the PROs (DLQI, Pain NRS, WPAI, TSQM, and HSQL). Differences between groups were evaluated using Fisher’s exact test for the proportion of patients attaining the MCID. Missing data were imputed using non-responder imputation (NRI). A nominal two-sided p-value is presented where applicable and is noted if less than 0.05.
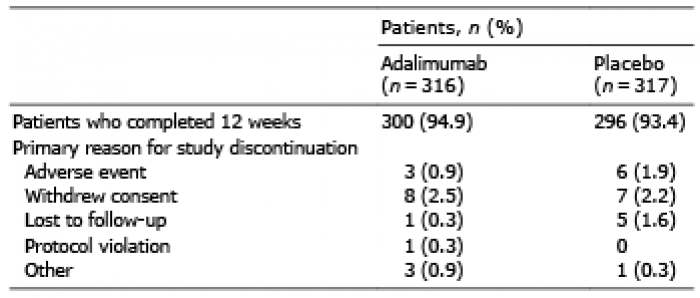
A total of 633 patients were randomly assigned treatment with either ADA (316 patients) or placebo (317 patients); of these, 629 patients were included in the integrated analysis; 4 patients were excluded because of missing data. Most (94.2% [596]) of the patients completed the study (Table I). At baseline, patients had a mean duration of HS of 11.5 years, with 46.9% of patients classified as Hurley Stage III (Table II). At baseline, mean ± SD lesion counts were 12.8 ± 11.7 for AN count, 2.5 ± 3.3 for abscesses, 10.3 ± 10.6 for inflammatory nodules, and 3.8 ± 4.8 for draining fistulas. Irrespective of treatment, 38.7% (245) of patients achieved HiSCR at week 12 and 60.7% (384) of patients did not.
Table I. Randomized patient disposition
Table II. Patient demographics and baseline characteristics
Irrespective of treatment, patients who achieved HiSCR experienced lower AN counts at week 12 (as expected because AN count reduction is a criterion of the HiSCR). The LS mean difference (95% confidence interval [CI]) was 8.6 (7.6, 9.7, p < 0.001) for AN counts (Fig. 1). Patients who achieved HiSCR also had lower lesion counts in multiple categories, including significantly fewer abscesses, draining fistulas, and inflammatory nodules at week 12 (Fig. 1). The LS mean difference (95% CI) was 6.7 (5.8, 7.7, p < 0.001) for inflammatory nodules, 2.6 (1.9, 3.3, p < 0.001) for draining fistulas, and 1.9 (1.6, 2.3, p < 0.001) for abscesses. Reductions in modified Sartorius scores and hs-CRP levels were observed at week 12; the LS mean difference (95% CI) was 46.1 (39.5, 52.7, p < 0.001) for modified Sartorius score and 6.2 mg/l (3.9, 8.6, p < 0.001) for hs-CRP.
Fig. 1. Least squares mean change from baseline to week 12 in clinical assessments: (A) lesion counts, (B) modified Sartorius score, and (C) high-sensitivity C-reactive protein (hs-CRP) levels. Missing data were imputed using last observation carried forward (LOCF). Asterisk (*) indicates statistical significance (p < 0.001) between Hidradenitis Suppurativa Clinical Response (HiSCR) responders and non-responders using analysis of covariance. AN count: sum of abscess and inflammatory nodules; CI: confidence interval; LS: least squares; SE: standard error.
Irrespective of treatment, patients who achieved HiSCR experienced significantly greater improvement in skin-specific quality of life as demonstrated by a greater reduction in mean DLQI score (Fig. 2); LS mean difference (95% CI) was 4.2 (3.3, 5.1, p < 0.001) for DLQI. Those who achieved HiSCR also had significantly greater reduction in skin pain as demonstrated by a decrease in Pain NRS, with LS mean difference (95% CI) 1.3 (0.9, 1.6, p < 0.001), and greater improvements in quality of life as demonstrated by an increase in HSQL, with LS mean difference (95% CI) –0.9 (–1.3, –0.6, p < 0.001) (Fig. 2).
Fig. 2. Least squares mean change from baseline to week 12 in patient-reported outcomes (PROs): (A) Dermatology Life Quality Index (DLQI) score, (B) Skin Pain Numeric Rating Scale (Pain NRS), (C) hidradenitis suppurativa quality of life (HSQL) score, (D) Work Productivity and Activity Impairment questionnaire (WPAI) scores, and (E) Treatment Satisfaction Questionnaire for Medicine (TSQM) scores. Missing data were imputed using last observation carried forward (LOCF). Asterisk (*) indicates statistically significant difference (p < 0.001) between Hidradenitis Suppurativa Response Score (HiSCR) responders and non-responders using analysis of covariance. Absenteeism, presenteeism, and overall work impairment were assessed only for employed patients. CI: confidence interval: LS: least squares; SE: standard error.
HiSCR responders experienced significantly greater improvement in presenteeism, overall work impairment, and activity impairment as demonstrated by greater reductions in mean scores (Fig. 2). The LS mean difference (95% CI) was 10.5 (5.6, 15.5, p < 0.001) for presenteeism, 10.2 (4.5, 15.9, p < 0.001) for overall work impairment, and 14.2 (10.2, 18.1, p < 0.001) for activity impairment; a statistically significant difference in absenteeism was not observed. HiSCR responders also experienced significantly greater satisfaction with the effectiveness of their medication and were more satisfied with their treatment overall (Fig. 2). The LS mean difference (95% CI) was –19.5 (–23.6, –15.3, p < 0.001) for satisfaction with effectiveness and –21.0 (–25.1, –16.8, p < 0.001) for global satisfaction; a statistically significant difference in patient satisfaction with side effects or convenience was not observed.
Fig. 3 specifies the MCID criterion for each PRO and summarizes the percentage of HiSCR responders and HiSCR non-responders who achieved clinically meaningful improvements in PROs during the study. Irrespective of treatment, significantly more HiSCR responders achieved a clinically meaningful improvement in DLQI than did HiSCR non-responders (60.5% vs 30.4%, p < 0.001), and a greater percentage of HiSCR responders achieved a meaningful improvement in Pain NRS compared with HiSCR non-responders (46.9% vs 19.9%; p < 0.001). More patients who achieved a HiSCR response also experienced a meaningful improvement in HSQL compared with patients who did not achieve a HiSCR response (49.4% vs 26.9%; p < 0.001). Significantly more HiSCR responders than HiSCR non-responders experienced meaningful improvements in presenteeism (52.6% vs 37.7%, p = 0.020) and activity impairment (59.5% vs 33.3%, p < 0.001). More HiSCR responders than HiSCR non-responders achieved a meaningful improvement in satisfaction with the effectiveness of their medication (65.2% vs 40.4%, p < 0.001) and global satisfaction with their medication (67.0% vs 39.3%, p < 0.001).
Fig. 3. Hidradenitis Suppurativa Response Score (HiSCR) at week 12 versus achievement of minimum clinically important difference (MCID) for patient-reported outcomes (PROs): (A) Dermatology Life Quality Index (DLQI) score, (B) Skin Pain Numeric Rating Scale (Pain NRS), (C) hidradenitis suppurativa quality of life (HSQL) score, (D) Work Productivity and Activity Impairment questionnaire (WPAI) scores, and (E) Treatment Satisfaction Questionnaire for Medicine (TSQM) scores. Missing data were reported using non-responder imputation (NRI). For DLQI, MCID was defined as at least a 5-unit decrease. For Pain NRS, MCID was defined as a ≥30% reduction relative to a patient’s baseline score and at least a 1-unit reduction from baseline. For HSQL, MCID was defined as one half standard deviation of the total population’s baseline score. For WPAI, MCID was defined as one half standard deviation of the total population’s baseline score. Absenteeism, presenteeism, and overall work impairment were assessed only for employed patients. For TSQM, MCID was defined as one half standard deviation of the total population’s baseline score.
Results presented in this study support HiSCR as a clinically meaningful indicator of improvement associated with a variety of positive health outcomes that are perceived as important and relevant to patients with HS. In this integrated analysis of two phase 3 studies, patients with HS who achieved HiSCR after 12 weeks of treatment experienced significantly fewer lesions of all types compared with those who did not achieve HiSCR. Achievement of HiSCR was accompanied by significant reductions in mean modified Sartorius scores and hs-CRP levels.
Attainment of HiSCR responder status was aligned with a clinically meaningful benefit from the patients’ perspectives as shown by significant improvements in skin-specific quality of life, pain at its worst, greater improvements in work and non-work-related activities, greater satisfaction with treatment, and the impact of HS on their lives. The findings of this analysis confirm the clinical meaningfulness of HiSCR as previously reported in its original validation (16). In both the original validation study and the present study, HiSCR achievers reported significantly greater improvements on DLQI, pain, overall work impairment, and daily activity impairment compared with nonachievers; the extent of the improvement in DLQI, pain, and WPAI scores was greater than MCID reported in the literature for the individual PROs (21, 22, 26). The present study took the analysis a step further and determined the percentage of patients who attained the MCID for each of the PROs. Achievement of HiSCR was associated with improvement in all clinical and patient-reported outcomes in this study. Specifically, at least half of HiSCR achievers reported improvement in quality of life outcome scores (DLQI, HSQL, overall work impairment, and activity impairment) that were greater than MCID. Results of the MCID analysis provide evidence that meaningful improvements are attained through achievement of HiSCR.
It should be noted that physicians and patients may evaluate the impact of disease on HRQL outcomes from different perspectives. For example, patient assessments may be influenced by their own experience and based on subjective symptoms, such as pain and how much the disease affects their ability to function, whereas physician assessments may be more influenced by observations of many patients or results obtained from more objective laboratory tests (27, 28). As a result, discordance between physician and patient assessments of disease activity have been reported for dermatologic diseases (27–30). Although we reported that HiSCR significantly correlated with physician-rated and patient-reported assessments (16), we do expect to see some degree of discordance between physician and patient assessments of HS disease activity because HiSCR is based on inflammatory count and not every nodule is the same in terms of pain and swelling, which are not captured in the clinician assessment. In addition, it can be difficult to distinguish between coalescing nodules in HS and as a result, accurately determining the counts can be challenging.
HiSCR is designed to assess treatment response by focusing on the inflammatory signs and symptoms of HS. A newly validated HS severity scoring system (IHS4) (31) also uses the inflammatory manifestations of HS as the basis of determining baseline disease severity. Because IHS4 uses the same clinical manifestations (abscesses, nodules, and draining fistulae) as HiSCR, these two tools may be easily incorporated into a clinical practice or clinical trial setting.
This study replicates and expands previously reported findings (16) examining how achieving HiSCR affects patients. However, there are limitations that need to be considered when interpreting the findings of this study. First, this was a post hoc analysis, and the randomized clinical trials that provided the data analyzed in this study were not powered or specifically designed for this investigation. Second, the results obtained in the clinical trial population may not be the same as those seen in the general population. Third, MCIDs were derived from baseline distributions. Detecting a meaningful change in PROs required baseline values to be within a specified level. As a result, the sample size for the MCID analyses was limited, particularly for WPAI absenteeism, for which only a few patients could exhibit a meaningful improvement based on the MCID threshold. Fourth, at the time the PIONEER studies were conducted, the MCID of the DLQI was 5 and this value was used as the pre-specified endpoint in these studies. Since then, the MCID of DLQI has shifted to 4 (21). To be consistent with the pre-specified endpoint in the PIONEER studies, our analysis used the more conservative cut-off point of 5 for DLQI, and the results demonstrate a positive association between clinically meaningful improvement in patient-reported HRQL outcomes and HiSCR achievement.
In conclusion, HiSCR offers an easy-to-use, valid, and reliable tool for assessing clinically meaningful HS treatment effectiveness in controlling inflammatory manifestations and improving health outcomes from the patient’s perspective. These data support the rationale for performing routine lesion counts and using HiSCR in noninvestigative daily practice both in the primary care and dermatology clinical settings.
Medical writing assistance was provided by Joann Hettasch, PhD, Fishawack Facilitate Ltd, Conshohocken, Pennsylvania, and was funded by AbbVie.
This study is a post hoc analysis of anonymized data from two previously published phase 3 clinical trials. Institutional review board approval was not required for this post-hoc analysis.
Funding: This work was supported by AbbVie. The study sponsor participated in the interpretation of data, review, and approval of the article.
Conflicts of interest: AK is a consultant and investigator for AbbVie and UCB and a consultant for Novartis. She has also received fellowship funding from AbbVie. TT is a consultant and investigator for AbbVie and UCB. BC, HT, and ZG are employees and stockholders of AbbVie. MO is a member of the speaker’s bureau for AbbVie, and is a consultant for AbbVie, Gilead Sciences, UCB, Crescendo Bioscience, GlaxoSmithKline, Innovaderm, and InflaRx.


 Click to show fullsize
Click to show fullsize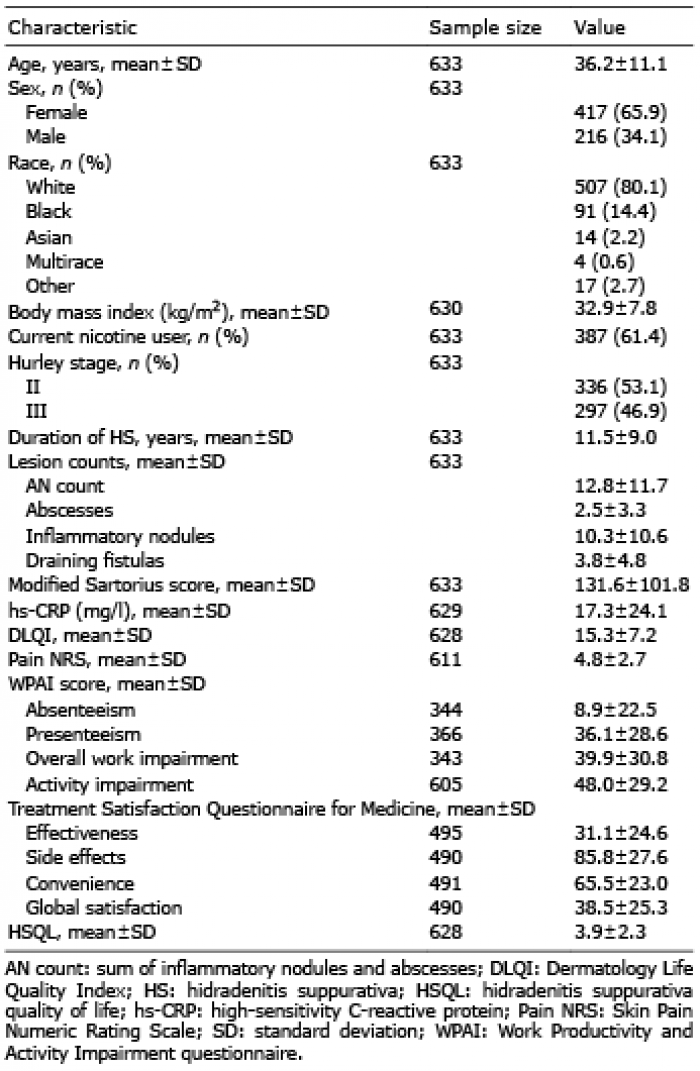 Click to show fullsize
Click to show fullsize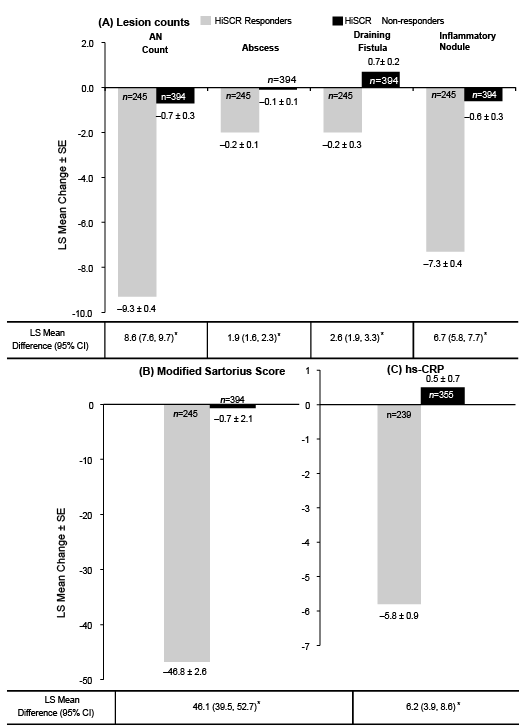 Click to show fullsize
Click to show fullsize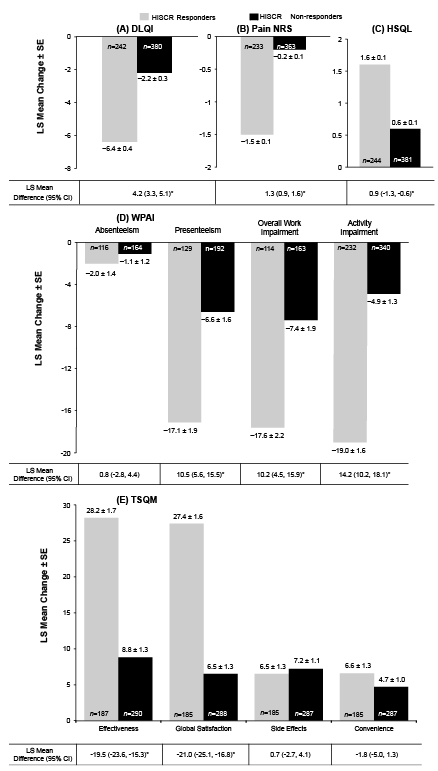 Click to show fullsize
Click to show fullsize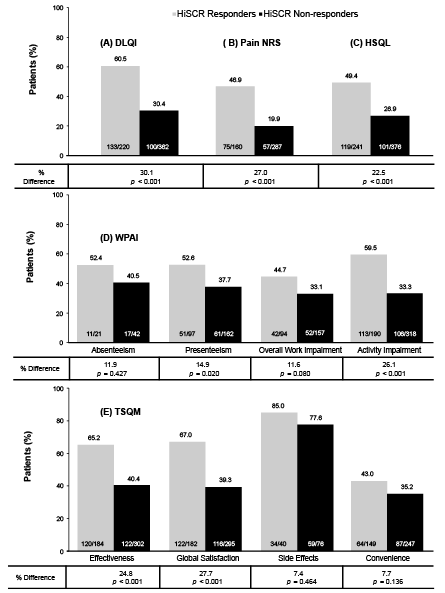 Click to show fullsize
Click to show fullsize