


Departments of Dermatology: 1Hospital da Barbanza, University Hospital, 2University of Santiago de Compostela, Santiago de Compostela, 3University Hospital, Pontevedra, 4Hospital Virxe da Xunqueira, University Hospital, La Coruña, 5University Hospital, Lucus Augusti, 6University Hospital, Vigo, 7University Hospital, Santiago de Compostela, 8University Hospital, La Coruña, and 9University Hospital, Ourense, Spain
Actinic cheilitis is thought to be a premalignant lesion or a superficial squamous cell carcinoma. The prevalence of actinic cheilitis in Europe is unknown. The aim of this study was to determine the prevalence of actinic cheilitis in the Galicia region (north-west Spain). Secondary objectives were the description of risk factors of actinic cheilitis. A cross-sectional multicentre study in patients ≥ 45 years of age was performed in 8 dermatology departments in Galicia region during a 1-year period. The prevalence of actinic cheilitis was 31.3%. Significant and independent risk factors of actinic cheilitis after multivariate analysis were age ≥ 60 years, Fitzpatrick skin phototype II, outdoor working for more than 25 years, and previous history of non-melanoma skin cancer. This is the first cross-sectional multicentre study of the prevalence of actinic cheilitis in Europe. Actinic cheilitis was present in almost one-third of the screened patients. Lip examination should be performed in all patients with chronic actinic damage.
Key words: actinic cheilitis; prevalence; epidemiology.
Accepted Aug 7, 2018; Epub ahead of print Aug 7, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Isabel Rodríguez-Blanco, Dermatology Department, Hospital da Barbanza-Hospital Gil Casares, C/Choupana s/n, ES-15706, Santiago de
Actinic cheilitis is a condition involving mainly the lower lip that is generally considered a superficial form of squamous cell carcinoma. Chronic sun exposure is a recognized risk factor for actinic cheilitis development. The prevalence of this disease in Europe is not known. We report the first multicenter prevalence study of actinic cheilitis. The disease was present in almost one third of the screened population ≥45 years. Significant and independent risk factors were age ≥60 years, fair skin (Fitzpatrick skin phototype II), outdoor working for more than 25 years and history of non melanoma skin cancer.
Actinic cheilitis (AC) is the most common denomination for a condition with clinical and histological changes due to chronic solar exposure, mainly involving the lower lip (1). Similarly to actinic keratosis (AK) of the skin, AC is considered to be a potentially malignant oral lesion (2) or even a lip in situ squamous cell carcinoma (SCC) (1, 3, 4).
Diagnosis and treatment of AC can be challenging; it has been shown that the clinical appearance of AC correlates poorly with the degree of dysplasia (5–9), thus clinicians have little evidence about the severity of the disease. The accuracy of diagnosis can be increased with new imaging techniques, such as dermoscopy, with the presence in AC of ill-demarcated borders, vascular telangiectasia, white-coloured projections and island-like structures around the ulcerous areas (10), or confocal microscopy (11). Performing a biopsy is mandatory in cases of doubtful lesions. Furthermore, the response to therapy is commonly unsatisfactory, with frequent recurrences.
There have been few epidemiological studies of AC compared with those related to AK; prevalence data of AC proceed from heterogeneous epidemiological studies performed in specific populations, mainly in South America (12–25), thus the prevalence in Europe has not been established, since multicentre, well-designed prevalence studies have not been performed.
The rate of progression of AC to an invasive SCC is unknown. Since the lip has traditionally been considered a high-risk location for SCC, knowledge of risk factors is of great importance.
The main objective of the present study was to determine the prevalence of AC in the Galicia region of Spain. Secondary objectives were: (i) to describe risk factors for AC in our study population; and (ii) to establish the clinical and epidemiological profile of patients with AC.
A cross-sectional multicentre study was conducted in Galicia (total population in 2016: 2,718,525; data from Galician Statistics Institute, http:www.ige.eu), a region located in north-west Spain. Consecutive patients attending a general dermatology outpatient clinic were recruited once a week from 12 January 2016 to 31 January 2017, by 8 dermatology consultants, located in 8 different hospitals. Only patients ≥ 45 years of age attending as a “First Visit”, who signed the informed consent were included. A “First Visit” was defined as: (i) a patient who was seen for the first time at that particular dermatology department; or (ii) a patient who had visited that dermatology department previously, but had been discharged. Patients who were not able to understand or answer the questions regarding clinical history were excluded. Data from each patient were collected by the dermatologists in a general form (Screening Form) and after clinical examination (naked eye and/or magnifying glasses), data from patients with AC were completed in an extra and detailed questionnaire (AC Form).
In a preliminary analysis, when 250 cases were reached, the prevalence of patients with AC was slightly higher than 30%, so a sample size calculation was performed using a formula to assess a proportion in a statistically infinite population, establish-ing a sample of approximately 1,200 cases that demonstrated a prevalence of approximately 30% with a standard error between 2.5% and 2.6%. Thus, more than 300 cases of patients with AC were recruited, increasing the statistical power of the comparisons between this subsample and the one without AC.
A descriptive analysis was performed for all the collected variables. Categorical variables were presented as a list of frequencies and proportions. In case of quantitative variables (continuous or ordinal) central tendency estimators, such as means, median and mode, and dispersion measures (standard deviation [SD] and maximum-minimum values) were calculated.
The study population was biased, with a greater presence of women and elderly subjects. In order to correct this bias, the screening sample was weighted according to the age and sex distribution for the Galician population over 45 years old in 2016 (source: Instituto Galego de Estatistica, https://www.ige.eu/web/index.jsp) using the raking ratio estimation method (26). This method is used to adjust the sampling weights of the sample data based on known population characteristics when they are more than one.
Clinical characteristics of AC, classification of Fitzpatrick’s skin type (27) and standardization of each hair and eye colour were precisely specified in a previous meeting by all the investigators, in order to minimize inter-observer bias. All the investigators were dermatologists with expertise in actinic damage and skin cancer. AC was defined by the presence of one or several of the following items (modified from Ribeiro et al. (22)): persistent desquamation, persistent erythema, mottled appearance (erythema and white patches), plaque (solid, raised, flat lesion > 1 cm) and/or erosion/ulceration that could not be attributed to other dermatological disorders. All patients were treated according to European Guidelines for the evaluation and treatment of AK (28), and those with uncertain lesions were biopsied according to clinicians’ criteria; therefore, those with uncertain eroded/ulcerated lesions (n = 7) were biopsied excluding SCC. Those patients with infiltrated erosions/ulcerations or tumour lesions, in which a firm suspicion of SCC was raised, were biopsied or completely excised and not included in the study.
The study protocol was approved by the Research Ethics Committee of Pontevedra-Vigo-Ourense, Spain (protocol number 2015/582).
All statistical analyses were performed using SPSS 22.0 statistical software for Windows.
A total of 1,250 patients were selected for the study, 11 of whom declined to participate in the study or to sign the consent form; therefore a total of 1,239 patients completed the Screening Form.
Data for the total and AC population of the study regarding age, sex distribution, tobacco consumption, Fitzpatrick skin type, outdoor working for more than 25 years and history of non-melanoma skin cancer (NMSC) are showed in Table SI. Additional demographic and clinical data for the AC population are shown in Table I.
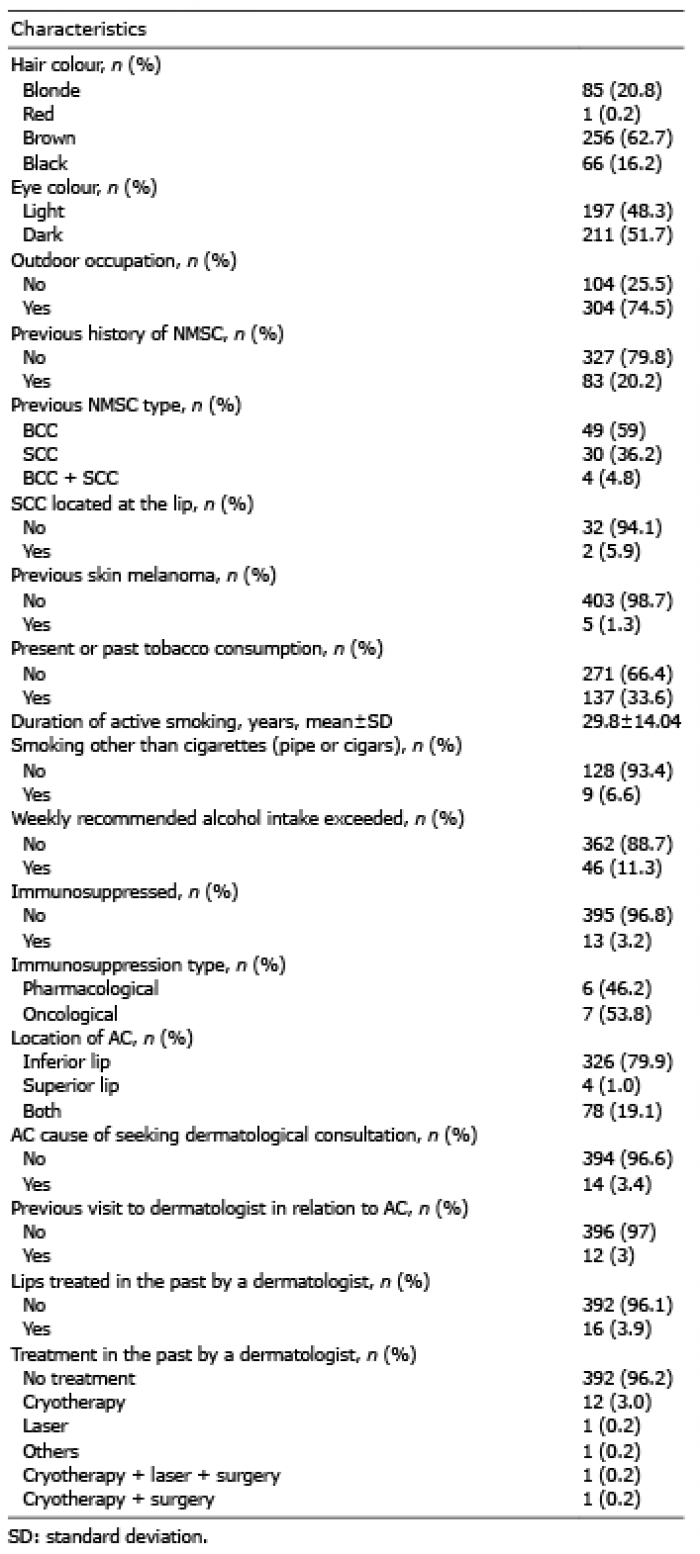
Table I. Summary table for patients with actinic cheilitis (AC)
The mean ± SD age of the total sample was 65.8 ± 11.9 years (range 45–96 years). Women accounted for 59.1% and 40.9% were men. Previous or current smoking history was reported by 38.4% of patients. All patients were Caucasians and Fitzpatrick type III was the most prevalent (52%), followed by type II (30.8%) and type IV (16.2%); types I and V were barely represented (0.6% and 0.5%, respectively) and no patients with phototype VI were present. Outdoor working for more than 25 years was reported by 39.7% of the patients and previous NMSC was present in 11.6% of the population.
In relation to the AC population, mean age was 71.9 years (SD 10.47, range 45–96 years) and regarding sex distribution, 55.4% were female and 44.6% were male. Most of AC population had skin phototype III (46.8%) or II (45.6%), followed by IV (7.1%) and I (0.5%). Both hair and eye colour were also analysed; brown hair was present in 62.7% of the population, followed by blonde hair (20.8%), black hair (16.2%) and red hair (0.2%), and 48.3% had light eye colour. Outdoor occupation was reported by 74.5% of the AC patients and 96.4% of them had worked outdoors for more than 25 years. Previous history of NMSC (confirmed by reviewing medical records or by a medical report from another centre supplied by the patient) was present in 20.2%, being basal cell carcinoma the most frequent (59%), followed by SCC (36.2%) and a combination of both (4.8%); in 5.9% of the patients with previous SCC, this carcinoma was located at the lip. Only 1.3% of the AC population had a previous skin melanoma. Present or past tobacco consumption was present in 33.6% of the patients with AC and the mean duration of active smoking was 29.8 years; only 6.6% had the habit of smoking other than cigarettes (pipe or cigars). Weekly recommended alcohol consumption (no more than 14 units during a week) was exceeded by 11.3%. Just 3.2% of AC patients were immunosuppressed, either related to oncological (53.8%) or pharmacological causes (46.2%). Location of AC was mainly at the inferior lip (79.9%), followed by both lips (19.1%) and only 1% at the superior lip. The reason for seeking dermatological consultation was the lip symptoms in only 3.4% of the AC patients; 3% had visited a dermatologist in the past in relation to a lip problem and 3.9% had their lips previously treated by a dermatologist (using cryotherapy, laser, surgery or others).
A total of 410 out of 1,239 patients were diagnosed as having AC and complete data were available in 408 patients. The prevalence of AC in the study population was found to be 33.1% (95% confidence interval (95% CI) 30.5–35.7). This result was corrected after weighting the total population of the study with data using Rake’s Ponderation method corresponding to age and sex distribution of Galician population from 45 years old onwards (year 2016, data from Galician Statistics Institute, www.ige.eu), being 31.3% (95% CI 28.7–33.8).
Univariate and multivariate analysis of the different variables are showed in Fig. S1. In univariate analysis, odds ratio (OR) related to female sex and tobacco consumption were 0.795 (95% CI 0.626–1.01, p = 0.06) and 0.77 (95% CI 0.6–0.99, p = 0.041), respectively, but after multivariate analysis these OR changed to 1.21 (95% CI 0.86–1.69, p = 0.27) and 1.36 (95% CI 0.96–1.93, p = 0.088), remaining the rest variables with minor changes (Fig. 1). Significant and independent risk factors of AC after multivariate analysis were age ≥ 60 years (from 60–69 years OR 4.07, p < 0.001; from 70–79 years OR 6.4, p < 0.001; from 80–89 years OR 9.46, p < 0.001; for older than 90 years OR 8.64, p = 0.004), Fitzpatrick skin phototype II (OR 2.94, p < 0.001), outdoor working for more than 25 years (OR 7.1, p < 0.001) and history of NMSC (OR 1.75, p = 0.012).
Fig. 1. Actinic cheilitis risk factors: univariate and adjusted.
The oncogenic potential of chronic sun-exposed skin is a major concern (4). AC is considered to be the lip counterpart of AK, with some peculiarities: the anatomical position and prominent shape of the lips make them more susceptible to UV radiation, mainly the lower lip, and to irritants, trauma or virus infections. The skin type of the vermillion is described as a transition between buccal mucosa and normal skin (3) and has a thinner epithelium that lacks keratin covering, with less melanin and fewer secretions from the sebaceous and sweat glands (6), all these features contributing to the increased susceptibility to solar radiation. Moreover, not only is AC a very well-known risk factor for the development of invasive SCC, but the lip has traditionally been considered a high-risk location for SCC.
The prevalence of AC in our study was 31.3%. The AC prevalence data described in the literature comprise a wide range, between 0.9% and 43.24% (12–25), and these differences could be related to the non-homogeneous clinical definition of AC and to the different inclusion criteria. Moreover, the majority of these studies were performed in selected populations, such as fishermen, sugar-cane collectors and rural workers from very specific geographical locations, lacking the advantages of a multicentre cross-sectional study. In addition, relevant data, such as Fitzpatrick skin type, previous solar exposure, photoprotective measures, history of NMSC and previous lip interventions were not properly collected. Therefore, transferring their results in terms of prevalence to the general population should be done with caution, as significant bias cannot be excluded. We consider that our study provides reliable data for AC prevalence, since it has been performed in 8 different hospitals, including patients selected only for the fact that they had arranged an appointment with a general dermatologist.
The high prevalence of AC in our study could be due to several reasons; one of them is the increasing median age of Galician population. Ageing is a major concern in terms of public health in industrialized countries. In 2016, population 65 years or older accounted for 24.31% in Galicia (data from Galician Statistics Institute, http:www.ige.eu), being one of the regions with the highest projected old-age dependency ratio in 2050 (29). Finally, another factor that may have influenced the results is the inclusion of early stages of the disease, such as persistent desquamation and persistent colour changes that could not be explained by other dermatological disorders; this allowed us to include even most incipient forms of AC.
A significant and independent correlation was found between age ≥ 60 years and AC, and the risk highly increased as age progressed. Significant association with ageing has been present in other studies (19, 21, 22) confirming that accumulation of sun exposure is the main risk factor for AC. This statement is further corroborated by the significant correlation between AC and outdoor working for more than 25 years (OR 7.14), being the relation with accumulated time of UV exposure also reported by other authors (18, 19, 22, 23, 25). Fitzpatrick phototype II was significantly related to AC presence (OR 2.94); this is coherent with previous AC prevalence studies that found a significant correlation with light/fair skin or white/Caucasian race (18–23, 25). No reliable data could be obtained regarding Fitzpatrick skin phototype I, since only 7 patients were screened and only 2 patients belonged to the AC positive subcohort. This is the first prevalence study of AC to specify Fitzpatrick’s classification of patients and data related to eye and hair colour. A significant correlation between history of NMSC and AC was described herein and no previous AC prevalence studies had analysed this before. This finding is consistent, as solar exposure is an important risk factor for AC and NMSC, mainly SCC, so AC should be ruled out in all patients with NMSC as part of routine dermatological exploration, in order to diagnose early stages.
The rest of the analysed variables were not significant. Sex distribution showed a high proportion of females in both the screening and the AC population (59.1% and 55.4%, respectively) and this could be related to the higher tendency of women to seek dermatological consultation compared with men (30); in contrast, other AC prevalence studies showed a clear superiority of men (15, 16, 18, 19, 23, 25) and the reasons the authors gave for that finding were that women often use lipsticks providing a physical block against UV radiation, have a bigger tendency to use a sunscreen and are less frequently engaged in outdoor activities. Furthermore, an important percentage of the AC prevalence studies were performed in specific populations with professional activities that clearly have a male predominance (fishermen, sugar-cane collectors, farmers, rural workers). Tobacco has a well-documented dose-response relationship with development of oral cancer (31) and lip cancer, especially in patients with the habit of leaving the cigarette on the lip while smoking (32). No relation between tobacco consumption and AC was found in our study and the same happened in all AC prevalence studies that specifically investigated this correlation (15, 18–22) or other AC retrospective studies (9) with the exception of Campisi & Margiotta (13) who described in 5 patients with AC a significant association with both tobacco smoking and alcohol drinking, but not separately. The influence of smoking in the development of AC has been controversial, but a causative relation has not been established (3), even when it is evident that constant exposure to heat generated by smoke combustion may aggravate the clinical aspect of the disease in individuals who are also exposed to solar radiation (3, 7, 19, 22). Alcohol drinking was correlated with AC in one study (19) in which the daily/weekly intake was not specified, as in the aforementioned study by Campisi & Margiotta (13).
Consistent with all prevalence studies, AC was located predominantly on the inferior lip and only 4 patients in our study (1%) had only superior lip affection, but all of them had had their inferior lip treated previously (2 with laser and 2 with surgical excision).
The present study has some limitations; one is related to its cross-sectional design in which the evolution is not analysed. In addition, the diagnosis was based on clinical features in more than 98% of cases and only 7 patients with uncertain lesions (1.71% of the AC population) were biopsied, being the clinical suspicion of AC confirming the clinical suspicion of AC in all of them. Although this is the first study of AC prevalence to assess the time period of tobacco consumption, a more accurate quantification could be made using the determination of pack-years instead of years of active smoking.
Only patients aged 45 years and over were selected for the study, as there is agreement that most cases occur in people over 50 years of age (6, 7, 19, 33); however, this could exclude younger patients with AC. The fact that the study was performed in an outpatient dermatology clinic setting may add some bias, as the higher proportion of female patients probably related to the aforementioned higher presence of females in dermatology clinics. Only patients attending as a “First Visit” were allowed to participate, excluding those who were followed up for other reasons, including AC, NMSC or others. Finally, even though a precise definition of AC was established before starting the study and all investigators were dermatologists with broad experience, inter-observer bias cannot be completely ruled out.
The first cross-sectional multicentre AC prevalence study is presented herein. As all previous prevalence studies, except for one in Sicily (13), were performed in South America, a close correlation with a European prevalence of AC in the Caucasian population aged 45 years and over should be expected. The high prevalence rates of AC documented in this study should alert public health authorities and clinicians to promote both primary and secondary prevention strategies. Photoprotective measures, long-term follow up and histopathological studies of suspicious lesions are recommended in order to decrease the potential progression of AC to invasive SCC.
Help with writing this paper was provided by CLEVER Instruments S.L, funded by LEO Pharma.
The authors thank Patricia Martin (LEO Pharma, Spain) for her deep involvement with this project.


 Click to show fullsize
Click to show fullsize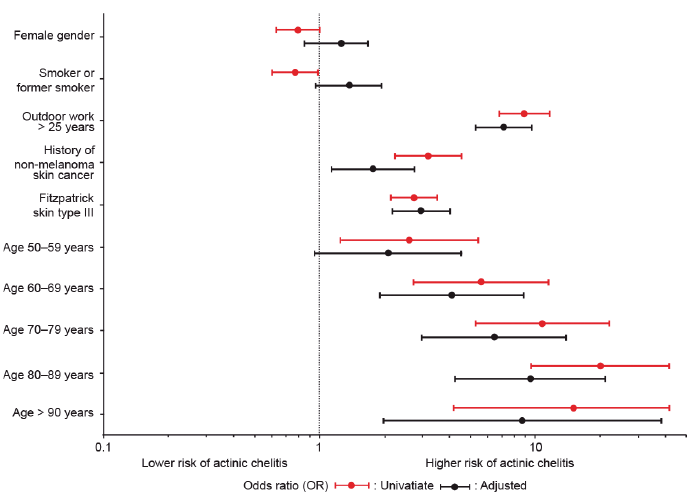 Click to show fullsize
Click to show fullsize