


1Department of Dermatology, Venereology and Allergology, 2Division of Laboratory Medicine, University Hospital Würzburg, and 3Institute of Pathology and Comprehensive Cancer Center Mainfranken, University Würzburg, Würzburg, Germany
Primary cutaneous marginal zone lymphomas (PCMZL) frequently exhibit lymphoplasmacytoid/plasmacytic differentiation, implying the capacity to produce monoclonal immunoglobulins. As these paraproteins are secreted, and thus are measurable in blood and urine, they may correlate with disease burden and serve as tumour markers reflecting therapeutic response. This study retrospectively analysed the records of 23 patients with PCMZL. During treatment and follow-up, laboratory tests, including full blood count, lactate dehydrogenase, serum protein electrophoresis and turbidimetric analyses, were conducted. Thirty-nine percent of cases showed a suspicious serum protein electrophoresis in terms of paraproteinaemia. In 44% of cases the heavy and light chain restriction in tissue samples correlated with serological findings. Altogether, 89% of the PCMZL patients with paraproteinaemia eventually experienced a relapse, in contrast to 62% of the group without paraproteinaemia. This study analysed the incidence and clinical implications of paraproteinaemia in patients with PCMZL. A clear correlation was found between paraproteinaemia, tumour relapse and therapeutic intervention.
Key words: lymphoma; immunofixation; monoclonal immunoglobulins; monoclonal gammopathy.
Accepted Aug 7, 2018; Epub ahead of print Aug 7, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Verena G. Frings, Department of Dermatology, Venereology and Allergology, University Hospital Würzburg, Josef-Schneider-Straße 2, DE-97080 Würzburg, Germany. E-mail: frings_v@ukw.de
The expression and secretion of monoclonal immunoglobulins or paraproteins by lymphoma cells is a well-known phenomenon. This study analyses the presence and significance of paraprotein expression and secretion in primary cutaneous marginal zone lymphoma. During treat-ment and follow-up, blood and tissue of 23 patients were evaluated for immunoglobulin expression by immunohistochemistry, serum protein electrophoresis and turbidimetric analyses. Concordant paraproteins shown in tissue samples were in almost all cases also detected in the blood correlating to the clinical course and tumour relapse. Our data suggest paraproteinaemia as a tumour marker in primary cutaneous marginal zone lymphoma.
The expression and secretion of monoclonal immunoglobulins or paraproteins by lymphoma cells is a well-known phenomenon frequently observed in various types of B-cell non-Hodgkin’s lymphomas (1). Lymphoma-derived paraproteins are monoclonal proteins by nature and can be detected as a homogeneous spike-like peak in a focal region of the gamma-globulin zone in serum protein electrophoresis (monoclonal gammopathy). Provided no haematological neoplasm is diagnosed as the underlying cause of monoclonal gammopathy, this putatively prodromal state before any overt lymphoma is designated as “monoclonal gammopathy of undetermined significance” (MGUS). Monoclonal gammopathy has to be clearly separated from polyclonal or oligoclonal elevation of immunoglobulins in response to, for example, inflammatory stimuli or chronic illness (2).
Monoclonal immunoglobulins (Ig) can present as IgM-isotype or as so-called class-switched isotypes, namely IgG, IgA, or IgE. Class-switched isotypes occur only after a complex molecular process of recombination and juxtaposition of the Ig heavy chain gene segment to rearranged variable segments, mainly in response to antigen exposure (3). Immunoglobulins expressed on the cell membrane of lymphoma cells can be visualized by immunohistochemistry in tumour tissue by routine histopathological work-up. Since paraproteins are secreted, and can thus be detected in blood and urine, they may serve as tumour markers reflecting therapeutic response. Their levels are thought to correlate with disease burden (4). In this respect, elevated monoclonal IgM is a typical feature of Waldenström’s macroglobulinaemia, defined as an IgM-restricted lymphoplasmacytic lymphoma (LPL) with bone marrow involvement and any level of an IgM monoclonal gammopathy in the blood (5–8). The WHO classification (9) recommends establishing the diagnosis of Waldenström’s macroglobulinaemia after exclusion of plasmacytoid/plasmacytic variants of other lymphomas. Since IgM paraprotein can also occur in other B-cell neoplasms such as IgM-expressing nodal marginal zone lymphomas (5, 10) or any precursatory MGUS, as mentioned above.
Primary cutaneous B-cell lymphomas (PCBCLs) encompass distinct entities, including the primary cutaneous marginal zone lymphoma (PCMZL) (11). PCMZL, an indolent lymphoma, is the second most common subtype of PCBCLs and belongs to the heterogeneous group of extranodal marginal zone lymphomas of the mucosa-associated lymphoid tissue (MALT) (7, 11–13). PCMZL usually shows an indolent clinical course with a 5-year survival rate of > 95%. Frequently, PCMZL exhibits lymphoplasmacytoid and plasmacytic differentiation (14), implying a potential for Ig production and secretion. Hence, national and international guidelines recommend serum protein electrophoresis to assess the presence of monoclonal gammopathy at time of first diagnosis of PCMZL (12, 15). However, as far as we know, no comprehensive data have been published to date on the systematic evaluation thereof, either at time of initial diagnosis or during follow-up of patients with PCMZL. Immunoglobulin light (kappa and lambda) and heavy chain expression (IgA, IgE, IgG and IgM) can be specifically visualized by immunohistochemistry in tissue. This feature is used as a diagnostic approach in addition to cytological and architectural features, further immunohistochemical workup (positivity of common B-cell markers CD20 and CD79a, negativity of germinal centre cell markers bcl-6 and CD10) and clonality analysis of the B-cell receptor (16). Contrary to non-cutaneous marginal zone lymphomas, that predominantly express the heavy chain IgM, PCMZL usually express class-switched immunoglobulins, such as IgG (mainly of the IgG4 subtype), IgA or IgE (17–20). We recently demonstrated that a rare subset of PCMZL expressing IgM heavy chains may also differ genetically from non-IgM-expressing PCMZL, as activating MYD88-mutations have been frequently, but hitherto exclusively, detected in this subgroup (21, 22). Extracutaneous manifestations of PCMZL are only rarely encountered (< 10%) (17). Hence, national and international guidelines usually recommend thorough clinical examination of the skin and lymph nodes as the most important follow-up examination of PCMZL, rather than routine imaging or blood tests (such as serum protein electrophoresis) (7, 9, 11).
No systematic investigation of the frequency of monoclonal immunoglobulin production in patients with PCMZL has been published so far. Therefore, the aim of the current study was to analyse the incidence, type and clinical relevance of paraproteinaemia in patients with PCMZL.
Within a retrospective setting we reviewed the records of 23 patients (at least 18 years of age) who were diagnosed with, treated and followed-up, for PCMZL at the cutaneous lymphoma outpatient clinic of the Department of Dermatology, Venereology and Allergology, University Hospital Würzburg, Germany. All patients had received skin biopsies or excision of the tumour with clear-cut diagnosis of PCMZL. At least 3 (dermato-) pathologists (EG, MW, AR) reviewed all histopathological cases with sections stained with haematoxylin and eosin and an appropriate panel of immunohistochemical stains to establish a diagnosis according to the WHO classification (7). In addition to routine histological assessment, we also analysed the presence and respective expression of immunoglobulin light (kappa and lambda) and heavy chains (IgA, IgG, IgG4 and IgM) in all cases as far as sufficient tissue material was available. Only cases with a clear-cut diagnosis of PCMZL were included; any ambiguous cases were excluded. Appropriate staging examinations included full blood count (Xn, Sysmex, Norderstedt, Germany), lactate dehydrogenase, turbidimetric analysis for direct detection and quantification of monoclonal immunoglobulins (Cobas Systems, Roche Diagnostics, Mannheim, Germany), serum protein electrophoresis (Hydrasys, Sebia, Evry, France), imaging examinations (ultrasound of lymph nodes and abdomen or computed tomography) and, in selected cases, bone marrow biopsy to exclude any systemic lymphoma manifestations. Tumour stage and the appropriate therapy were established according to international recommendations (23) and the German guidelines for cutaneous lymphomas (24, 25). Follow-up investigations included regular laboratory tests (blood and urine) with a varying panel of parameters. Relapse was defined as any novel cutaneous or extracutaneous manifestation of PCMZL and cure as absence of any disease manifestations.
We analysed the records of 23 patients (mean age 61 ± 18 (range 30–99) years; 12 females, 11 males) with a diagnosis of PCMZL. Eighteen patients were examined regularly from initial diagnosis onwards; mean follow-up time was 78 ± 57 (range 4–192) months until the time of submission of manuscript. Five patients were lost to follow-up after a mean of 67 ± 38 (range 13–115) months, mainly due to consecutive aftercare by local dermatologists. None of the patients showed B symptoms at any time. At first consultation lactate dehydrogenase was within standard values (< 250 U/l) in all patients.
At initial diagnosis, 12 (52%), 8 (35%), and 3 (13%) patients were staged pT1, pT2 and pT3, respectively. None of the patients showed any manifestation of systemic lymphoma in the applied staging examinations including imaging and, in selected cases, bone marrow biopsy. One patient presented with micro-focal bone marrow infiltration not contradicting the final diagnosis of PCMZL according to standard diagnostic consensus guidelines (23, 26, 27). During further follow-up, no progress was seen in 7 patients with tumour stage pT1. Two patients showed progress to tumour stage pT2 and another 3 patients developed tumour stage pT3. Regional lymph node involvement based on clinical and radiological investigation was seen in one patient, showing complete stable remission after rituximab and radiotherapy. Histopathological examination was not performed in this case. Two further patients presented with a histologically proven non-related secondary nodal lymphoma (nodal marginal zone lymphoma, clonally divergent) with one of these cases being published previously (28). No more patients showed any distant organ involvement.
Different therapeutic modalities according to tumour stage and the patient`s general condition were applied according to treatment guidelines that included tumour excision, radiation therapy or, in selected cases, systemic treatment (rituximab, bendamustine or α-interferon). At time of manuscript submission, 13 (72%) patients were tumour-free, 5 (28%) were alive with disease and no information on the outcome was available in another 5 (28%) cases. No death attributed to the lymphoma occurred in the followed-up patient population.
In addition to routine histological assessment, additional (immuno-) histochemical information for expression of immunoglobulin light (kappa and lambda) and heavy chain (IgA, IgG, IgG4 and IgM) was available with varying frequencies. Light and heavy chain restriction was present and analysed in areas of plasmacytic differentiation within the lymphoma infiltrate. Immunoglobulin light chain expression was assessable in 21 out of the 23 cases; thereof, 12 (57%) cases showed restriction to kappa and 6 cases (29%) to lambda light chains. In 3 (14%) cases, we observed no light chain predominance. Furthermore, information about heavy chain expression in tissue was available in 19 out of 23 cases; thereof, 5 (26%) cases were solely positive for IgM, 9 (47%) cases for IgG and 2 cases (11%) for IgA. No heavy chain predominance was found in 2 (11%) cases. All patients met the criteria of PCMZL irrespective of the results of the light or heavy chain restriction.
PCMZL patients received routine laboratory tests including urinalysis (14/23), serum protein electrophoresis at first presentation and over time (21/23) and direct assessment of immunoglobulins by turbidometry (16/23) at time of first diagnosis and on further follow-up. Nine of 23 patients (39%) showed a suspicious serum protein electrophoresis. Of these, 89% (8/9) presented with a monoclonal peak within the gamma fraction suggestive of monoclonal gammopathy and 11% (1/9) expressed an oligo- or polyclonal pattern. One patient initially presented with a normal serum protein electrophoresis and subsequently developed a monoclonal peak. Cases with mono-/oligo-/polyclonal paraproteinaemia in serum protein electrophoresis were then further analysed for direct quantification of the respective paraproteins (IgG, IgM, IgA) by turbidimetric immunoassays. Eight out of 9 (89%) and one additional patient with an unsuspicious serum protein electrophoresis, who by chance received a turbidimetric immunoassay, showed paraproteinaemia, i.e. elevated levels of IgG, IgM, or IgA.
Furthermore, 54% (7/13) of our patients had an abnormal light chain expression in the serum and 36% (5/14) presented with kappa light-chain proteinuria at either time of diagnosis or during scheduled monitoring.
Of the 9 patients with paraproteinaemia, 44% (4/9) presented with monoclonal IgM and 11% (1/9) with monoclonal IgG. Two cases (22%) showed a combined IgG/IgA or IgG/IgM paraproteinaemia. More than half of the patients with proved paraproteinaemia (56%; 5/9) had a persistent course of increased IgG, IgM or IgA levels in serum without normalization while being under therapy. In addition, in 67% (6/9) of these cases an increased kappa/lambda quotient, indicating light chain restriction, could be seen in the serum as well.
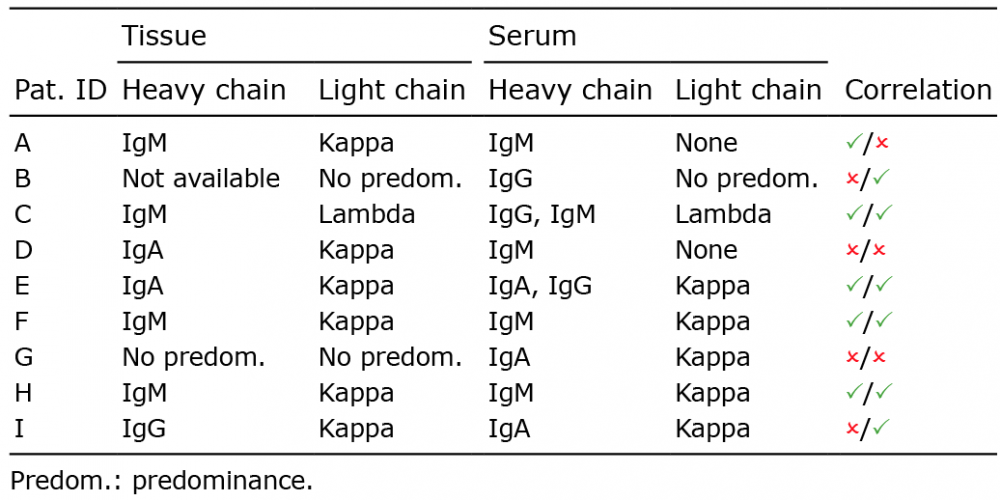
In 44% of the cases with paraproteinaemia, the elevated heavy and light chain correlated between the histological and serological findings. In another 33% of cases, at least either the heavy or light chain restriction correlated. Of all 9 cases with evident paraproteinaemia, 2 could not be assessed histologically due to missing availability of tissue samples (Table I).
Table I. Detailed overview of tissue light and heavy chain restriction in relation to serological paraproteinaemia
Coincidentally, patients with paraproteinaemia comprised all detected cases of proteinuria (5/14 in all patients, 5/9 in patients with paraproteinaemia).
Serological tests detected conspicuous serum protein electrophoresis in 89% (8/9) of the paraproteinaemia cases. In 1 patient serum IgM paraproteinaemia was detected; however, 7 years before he was diagnosed with PCMZL. Waldenström’s macroglobulinaemia had been ruled out on several occasions in that case. In 44% (4/9) paraproteinaemia normalized under therapy.
Six of 9 patients with paraproteinaemia underwent tumour excision as primary treatment. Radiation therapy was initially performed in the remaining 3 patients, since surgery was not the first therapeutic choice due to tumour size or multilocular manifestation.
Altogether, 8 PCMZL patients (89%) with paraproteinaemia eventually experienced a relapse. In contrast, only 9 of 14 patients (64%) without paraproteinaemia relapsed. Five patients (56%) with paraproteinaemia received at one or more occasions a systemic therapy with rituximab, and radiation therapy was administered as second- or third-line therapy in 3 patients (33%). Only one patient with deep extensive lymphoma manifestation of PCMZL received bendamustine as next-line treatment.
To assess whether paraproteinaemia might be a diagnostic parameter of disease severity and progression in patients with PCMZL, we correlated clinical data with serological findings. A detailed overview of paraproteinaemia over a distinct period and its change depending on disease course, i.e. tumour relapse or treatment response/therapeutic intervention, is given in Fig. 1 for the 9 patients with paraproteinaemia treated at our institution. Overall, a clear correlation was noted between paraproteinaemia, tumour relapse and therapeutic intervention. A detailed overview of the patients with paraproteinaemia and PCMZL is given in Table II. A decrease in paraproteinaemia corresponded to clinical response. However, the presence or extent of paraproteinaemia was, in general, not indicative of overall clinical stage according to TNM classification.
Fig. 1. Incidence of paraproteinaemia and its change depending on disease course, i.e. tumour relapse or treatment response/therapeutic intervention for 9 patients with primary cutaneous marginal zone lymphomas. A clear correlation can be seen between paraproteinaemia, tumour relapse and therapeutic intervention.
Table II. Relation between paraproteinaemia and disease burden: a detailed overview
Paraproteinaemia is a well-known phenomenon in patients with a variety of haematological neoplasias; how-ever, to the best of our knowledge no previous study has evaluated the incidence of paraproteinaemia in PCMZL and its significance as a marker for disease severity and treatment response.
Paraproteinaemia has repeatedly been reported in patients with various forms of NHL (1, 29–31), but has been considered to be a rare event in patients with MALT lymphoma (10). In our study, a distinct relationship between serum paraproteinaemia and the immunohistochemical results for heavy and light chain restriction was noted (67%, 6/9). In those patients with divergent tissue and blood findings with respect to paraprotein subtype, no evidence of further (systemic) lymphoma was present at time of diagnosis or during follow-up. This finding is consistent with previous studies (10), and suggests that the most likely explanation for paraproteinaemia in patients with PCMZL is the production of immunoglobulins by clonal lymphoplasmacytic/plasmacytic cells.
With respect to IgM paraproteinaemia, the detection of monoclonal IgM is a hallmark of LPL/Waldenström’s macroglobulinaemia; however, IgM paraproteinaemia may also be found in patients with a variety of other types of B-cell lymphoma. In a survey of 430 patients with serum IgM paraprotein, Kyle & Garton (6) identified, among other lymphoproliferative diseases, 242 (56.3%) as MGUS, 71 (16.5%) as Waldenström’s macroglobulinaemia, and 21 (4.9%) as CLL. In addition, Lin et al. (5) investigated lymphoid neoplasms associated with IgM paraproteinaemia and showed that, apart from typical associations, such as LPL/MW, approximately 20% of cases could be attributed to other types of B-cell lym-phoma and, rarely, T-cell lymphoma.
This is supported by our study that proved the capacity for immunoglobulin production and, thus, paraproteinaemia in 43% of cases (9/21) of PCMZL that could be attributed to increased IgM levels in nearly half of the patients (44%, 4/9). Among the analysed patients with PCMZL, 22% (2/9) presented with IgA, 11% (1/9) with IgG, and 2 (22%, 2/9) with combined IgG/IgA or IgG/IgM paraproteinaemia. This contrasts with data on the prevalence of respective heavy chain expression in tissue of PCMZL taken from literature or our own prior studies (21, 22, 32). Accordingly, PCMZL exhibit a preferential IgG (and less often IgA) heavy chain expression, while non-cutaneous marginal zone lymphomas predominantly display IgM expression (18, 19, 22). According to these data, a novel concept has evolved demonstrating that 2 major biological subsets reside within PCMZL. One of those expresses class-switched immunoglobulins (IgA, IgG and IgE) and is the prevailing subtype, whereas the other subtype expresses non-class-switched IgM immunoglobulins (18, 19). Recent studies (19, 20) report that both types differ in the composition of inflammatory bystander cells, in that fewer infiltrating T cells and regulatory T cells are presenting IgM-positive PCMZL. These results support the assumption that class-switched and non-class-switched PCMZL are likely to have distinct biological features, as evidenced even on molecular genetic grounds (21, 22). However, the patient sample in the current study is too small to determine whether the presence of IgM paraproteinaemia in PCMZL is non-proportionally more frequent than in class-switched subtypes, or if IgM-positive cases may run a less indolent course.
Wöhrer & Raderer (10) reported that 21% of their patient collective with extranodal marginal zone lymphoma showed evidence of paraproteinaemia using immunofixation, while conventional serum protein electrophoresis was not indicative of paraproteinaemia. With respect to correct assessment of the frequency of paraprotein production, this information would have been missed without performance of additional immunofixation. According to this finding, we likewise hypothesize that the true frequency of paraproteinaemia may so far be underestimated in patients with PCMZL.
In order to gather further data on the true frequency and clinical implication of paraproteinaemia in PCMZL, not only serum protein electrophoresis should be implemented into the diagnostic algorithm of current national and international guidelines (15, 23), but also adjunctive immunofixation during the clinical course as a putative indicator of relapse.
This study shows that PCMZL frequently presents with elevated immunoglobulins in the serum, analogous to the expression pattern of the respective immunoglobulin heavy chain in the tissue as determined by immunohistochemistry. A clear relation could be established between the level of paraproteinaemia and the clinical course. Even though the number of PCMZL cases with paraproteinaemia is limited in our case series, we propose that the serological assessment of monoclonal immunoglobulins (protein electrophoresis and immunofixation) in patients with PCMZL may be an adjunctive clinical marker for tumour recurrence or therapeutic response in addition to thorough whole-body examination.
This work was supported by the Interdisziplinäre Zentrum für Klinische Forschung (IZKF), University Hospital Würzburg (Z-2/75).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize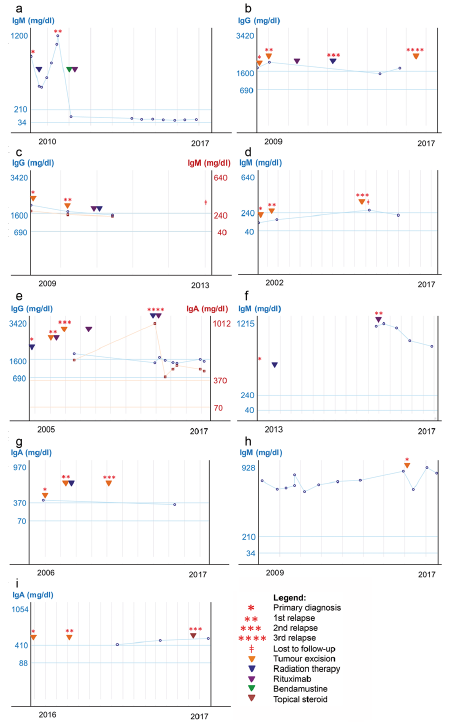 Click to show fullsize
Click to show fullsize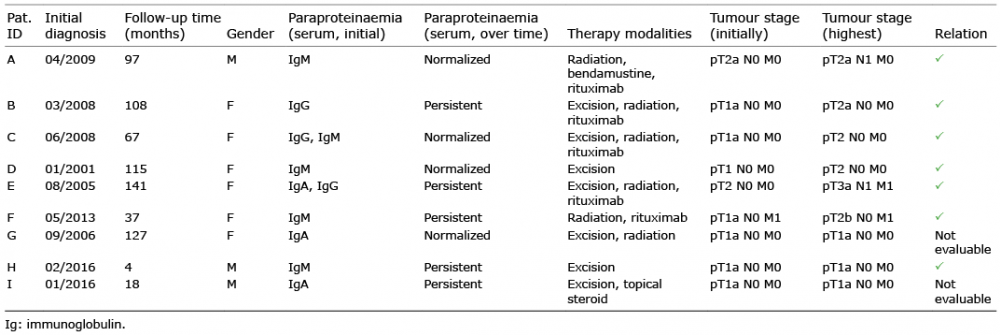 Click to show fullsize
Click to show fullsize