


Department of Dermatology and Venereology, Skåne University Hospital, SE-205 02 Malmö, Sweden. E-mail: gregtheodosiou@yahoo.com
Accepted Aug 29, 2018; Epub ahead of print Sep 3, 2018
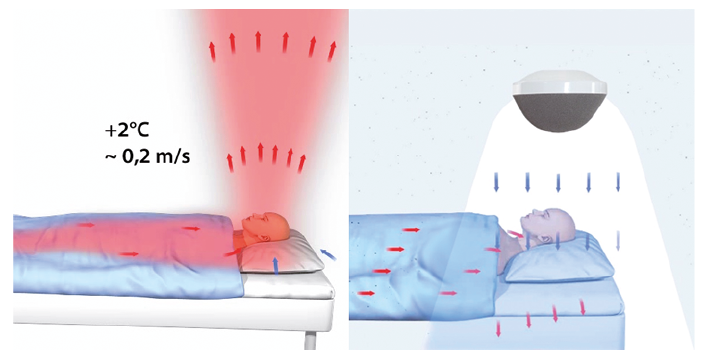
Children and teenagers with severe atopic dermatitis (AD) refractory to standard treatment often require systemic treatment with anti-inflammatory and immunosuppressive drugs. The temperature-controlled laminar airflow (TLA) (Airsonett™) device is a non-pharmaceutical add-on treatment option for patients with poorly controlled allergic asthma. The TLA delivers filtered, allergen-free, particle-free air to the patient’s breathing zone during the night (Fig. 1). It has been shown to improve quality of life (QoL) and reduce symptoms and exacerbations of asthma (1). Aeroallergens have been shown to elicit AD (2). However, specific allergen immunotherapy, reduction in house dust mites, and avoidance measures for treating AD have shown mixed outcomes (3). The effect of TLA use in patients with AD has not been sufficiently investigated. We report here a case of a teenager with severe AD refractory to intensive topical treatment and phototherapy, which responded to overnight use of a TLA during a 12-month period.
Fig. 1. Temperature-controlled laminar airflow (TLA) device function. Arrows indicate the direction in which particles flow (a) without and (b) with the TLA operating. The red arrows indicate the the upward airflow during sleep that concentrates the airborne particles and allergens to the breathing zone of the patient. The blue arrows indicate the cooled and filtered air that descends towards the breathing zone of the patient counteracting the allergen- and particle-rich airflow.
A 14-year old boy with persistent severe AD and allergic rhinoconjunctivitis, who had been a patient of our department since early childhood, was prick-tested and found to be sensitized to pollen and house dust mite. His disease was severely pruritic with frequent exacerbations and severe impairment of QoL for years despite therapy escalation. His parents had repeatedly reported that he would wake up frequently at night, stay awake due to attacks of itching, and experienced daytime sleepiness.
The patient had been treated previously with various topical regimens, including emollients, strong glucocorticosteroids and tacrolimus 0.1%, with partial improvement. He had also been treated with narrow-band ultraviolet B phototherapy 3 times a week for 12 weeks, with no effect and, subsequently, with a UVA/UVB phototherapy regime, 2 times weekly for 14 weeks, which resulted in minimal improvement in itch, QoL and sleep-quality.
We decided to try the overnight use of a TLA, initially for a 4-month period, as an add-on treatment, instead of proceeding direct to systemic treatment, given the fact that the patient and his family were reluctant to try systemic immunosuppression. The effect of the treatment was assessed using SCORing Atopic Dermatitis (SCORAD)-Index, Investigator Global Assessment (IGA), Dermatology Life Quality Index (DLQI), visual analogue scale (VAS)-itch, and VAS-sleep. During overnight use of the TLA the patient was treated with anti-inflammatory mometasone-furoate 0.1% cream once daily and an emollient containing 5% urea at least twice daily.
At the first follow-up visit, 4 months later, the patient’s QoL was significantly improved, he reported a marked improvement in sleep quality, and agreed to continue with overnight use of the TLA. No adverse events were reported. The improvement in SCORAD was parallel to the improvement in QoL and it was decided to extend the overnight use of the TLA for a 12-month period. The visible lesions cleared and the anti-inflammatory topical therapy was tapered down to twice weekly until the next follow-up visit.
At the subsequent visit, 4 months later, the patient was almost free of symptoms, with only residual skin lichenification. He was able to reduce his treatment to moisturizers only. A significant improvement was observed in SCORAD, IGA and DLQI. The same parameters had plateaued at the 12-month assessment (Fig. 2).
Fig. 2. (a) SCORing Atopic Dermatitis (SCORAD). (b) Investigator Global Assessment (IGA). (c) Dermatology Life Quality Index (DLQI). (d) Visual analogue scale (VAS)-sleep and VAS-itch before, during and after 12-months’ add-on therapy with Airsonett™ (Airsonett AB, Ängelholm Sweden).
AD is the most common inflammatory disease during childhood, affecting up to 20% of children (4). AD accounts for the largest global burden of disability due to skin disease (4). Despite advances in treatment for AD the disease remains poorly controlled in a significant number of patients (5).
Exposure to aeroallergens, including gaseous-phase particles and pollutants derived from outdoor air and a variety of indoor sources including human-related activities, e.g. cooking and cleaning, and various biological sources, e.g. mould, fungal spores, pet and house dust-mite allergens, has been associated with the development and exacerbation of asthma (6).
Aeroallergens have been also shown to induce AD (2). A meta-analysis of studies of house dust mite avoidance strategies was inconclusive due to low-quality evidence available at that time (3). Similarly, a recent meta-analysis of 12 trials found no consistent evidence that specific allergen immunotherapy is effective for treating AD in patients sensitized to aeroallergens, but the low quality of evidence available was highlighted (7).
The device Airsonett™ (Airsonett AB, Ängelholm Sweden) uses a TLA of purified air directed to the patient’s breathing zone during the night (1). TLA distributes a filtered cooled laminar airflow, which displaces aeroallergens from the breathing zone (Fig. 1) (1, 8, 9). It has been shown that the TLA significantly reduces airway inflammation and improves the QoL of patients with allergic asthma (8, 9). A recent open-label, proof-of-concept trial demonstrated that TLA treatment may be an effective add-on to the management of children with severe AD (10). The purported mode of action is the elimination of aeroallergens during sleep.
At baseline our patient had persistent pruritus, which led to attacks of scratching, sleeplessness and daytime sleepiness, with a negative impact on his QoL, despite continuous medical treatment. The SCORAD index at baseline was 55.3. At follow-up visits at 4, 8 and 12 months, respectively, improvement in the rash with reduced skin inflammation was observed, as well as improvement in SCORAD, IGA and the patient-reported outcomes, VAS-itch and DLQI, compared with baseline. The improvement in severity of dermatitis was accompanied by a reduction in medication use. The frequency of application of topical glucocorticosteroids was gradually reduced to twice a week, while the patient continued with daily moisturizer. At the 12-month visit the topical treatment was limited to emollients alone.
A significant improvement in sleeping quality was reported. VAS-sleep was reduced from 9 to 0 over a period of 12 months. The TLA also provided long-lasting relief from intense pruritus. VAS-itch was reduced from 8 to 1 at the final visit. No adverse events were reported.
We report here a case of a teenager with AD refractory to standard treatment, which responded to overnight use of a TLA device. The patient reported a significant improvement in QoL over the entire 12 months. He was willing to continue with overnight use of the TLA device after the 12-month observation period. This preliminary report suggests that TLA treatment could be considered as an add-on therapy for patients with severe AD.
The main limitation of this report is that it is possible that the clinical improvement seen during the 12-month period was in fact spontaneous remission due to the unpredictable course of the disease, or even to the placebo effect. Another limitation is that it remains unclear why displacement of the aeroallergens and/or other inhaled exposures from the patient’s breathing zone during the night, which is the purported mode of action of TLA, might improve this skin condition.
Further studies are warranted to determine the efficacy of TLA in AD and to identify which patients will benefit most.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize