


1Department of Dermatology, Radboud University Medical Center, 2Department for Health Evidence, Radboud University, and 3Radboud University, Nijmegen, The Netherlands
Little is known about the relationship between nail psoriasis and psoriasis severity in children, and there has been no longitudinal assessment of psoriasis severity related to nail psoriasis. The aim of this study was to assess whether nail psoriasis could serve as a predictor for a more severe disease course. De-identified data were obtained from the ChildCAPTURE registry, a daily clinical practice cohort of children with psoriasis, from September 2008 to November 2015. Cross-sectional analyses were performed at baseline. Longitudinal data until 2-year follow-up were analysed by linear mixed models. Nail psoriasis was present in 19.0% of all 343 patients at baseline and cross-sectionally associated with higher Psoriasis Area and Severity Index (PASI) (p = 0.033). Longitudinal analysis demonstrated higher PASI (p < 0.001) during 2-year follow-up in patients with nail involvement at baseline. These findings suggest that nail psoriasis is a potential clinical predictor for more severe disease course over time in paediatric psoriasis.
Key words: paediatric psoriasis; pediatric psoriasis; nail psoriasis; psoriasis severity.
Accepted Sep 11, 2018; Epub ahead of print Sep 12, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Inge M. G. J. Bronckers, Department of Dermatology, Radboud University Medical Center, René Descartesdreef 1, PO Box 9101, NL-6500 HB, The Netherlands. E-mail: Inge.Bronckers@radboudumc.nl
Psoriasis is a common chronic inflammatory skin disorder that can also affect the nails. It develops during childhood in almost one-third of cases. Early identification of children with an increased risk for a severe course of their psoriasis is essential for adequate intervention and subsequent limitation of disease progression. This study shows that nail involvement in paediatric psoriasis is associated with a more severe psoriasis disease course during 2-year follow-up. These findings suggest that nail psoriasis is a potential clinical predictor for a more severe disease course over time in children with psoriasis.
Psoriasis develops during childhood in almost one-third of cases, with an almost linear increase in prevalence rates until 18 years of age (1–5). Nail psoriasis affects over 50% of the adult population with psoriasis, and is even more prevalent in patients with psoriatic arthritis (PsA) (6–11). Although a range of prevalence rates has been reported in children, a recent study of 4,853 children revealed an overall prevalence of 15.7% (12, 13).
Evidence regarding nail psoriasis in children and its association with psoriasis severity is scarce. A recent multicentre, cross-sectional study demonstrated more severe disease in 313 children with nail involvement compared with those without nail involvement. Nail psoriasis was also associated with male sex, palmoplantar psoriasis and PsA (14). Two other cross-sectional studies in children reported no relationship between nail psoriasis and psoriasis severity (13, 15). Remarkably, reported signs of nail psoriasis and psoriasis severity scores in these studies were based on historical information rather than physical examination of the nails and skin. In adults, studies have found nail psoriasis to be a potential clinical predictor of developing enthesitis and PsA (16, 17), and have demonstrated an association between nail psoriasis and higher psoriasis severity scores (9, 18–21). Augustin et al. (20) reported higher Psoriasis Area and Severity Index (PASI) and Body Surface Area (BSA) scores in adult patients with nail psoriasis in a cohort of 3,531 patients. Based on these findings, they proposed to examine whether current nail involvement is predictive of a more severe psoriasis course in future.
Approximately one-third of children with psoriasis experience more severe or recalcitrant disease (5, 22). Early identification of children with an increased risk for a severe disease course is essential for adequate intervention and subsequent limitation of disease progression. The presence of nail psoriasis as non-invasive, clinical predictor for a more severe disease course could contribute to this concept and become important for providing optimal treatment strategies.
The aim of this prospective, observational study in a daily practice cohort of paediatric patients with psoriasis was to describe epidemiological and disease characteristics of children diagnosed with nail psoriasis at baseline, to determine the presence of nail psoriasis over time, to assess the relationship between nail psoriasis and reported psoriasis severity scores, and, ultimately, to study the predictive value of nail psoriasis for a more severe disease course over time.
This prospective, single-centre study was conducted in children (aged < 18 years) diagnosed with psoriasis who attended the outpatient clinic of the Department of Dermatology at the Radboud University Medical Center between September 2008 and November 2015. All available data were extracted from the ChildCAPTURE registry (Continuous Assessment of Psoriasis Treatment Use Registry), a prospective, long-term, observational daily practice cohort of children with psoriasis. The study was carried out in the Netherlands in accordance with the applicable rules concerning the review of research ethics committees and informed consent.
At baseline and during follow-up, patient, psoriasis and treatment characteristics, including presence of nail psoriasis and PsA, were collected using a standard case report form. Psoriasis severity scores (PASI, BSA and Physician Global Assessment (PGA)) and patient-reported outcome measures (Children’s Dermatology Life Quality Index (CDLQI); visual analogue scales (VAS) for psoriasis severity, itch, pain and fatigue) were also collected. Patients on topical treatment were seen at least every 6 months to 1 year; patients on systemic medication (e.g. methotrexate, dimethylfumarate, biologics) were seen every 3 months. Cross-sectional analyses were performed at baseline visit.
Nail psoriasis. The diagnosis of nail psoriasis was made by 2 clinicians, and exclusively based on physical examination. All 20 nails were examined. Furthermore, the target Nail Psoriasis Severity Index (NAPSI) was used as a quantitative nail assessment tool at baseline and during each follow-up visit. This tool divides the nail into imaginary quadrants and records the number of quadrants in which any manifestations of nail matrix psoriasis (pitting, leukonychia, red spots in lunula, nail plate crumbling) or nail bed psoriasis (oil drop discoloration, onycholysis, nail bed hyperkeratosis, splinter haemorrhage) are present. At each visit the most severely affected nail was assigned a nail matrix and nail bed score of 0–4, which yielded a composite score between 0 and 8.
Psoriasis severity scores. PASI, BSA and PGA scores from 0 (clear) to 5 (very severe) were reported at baseline and during each follow-up visit. All psoriasis severity scores over a period of up to 2 years were included to assess disease severity over time in patients with and without nail involvement. This timeframe was based on mean ± standard deviation (SD) follow-up duration of 22.9 ± 23.5 months in 343 children. Two-year follow-up data were available for 40.5% of children. The percentage of patients with at least 2-year follow-up was comparable between the groups (nail psoriasis 41.5%; no nail psoriasis 40.3%, p = 0.853).
The presence or absence of nail psoriasis during follow-up was captured to better understand its consistence over time in children. The following categories can be distinguished: (i) patients with persistent nail psoriasis over time, (ii) patients with nail psoriasis occasionally during follow-up, and (iii) patients without nail psoriasis at any point in time.
Cross-sectional. Demographic data were summarized as medians and interquartile ranges (IQR) for continuous variables, and numbers and percentages for categorical variables. Patient and disease characteristics were presented for: (i) total number of patients, (ii) patients with nail involvement at baseline, and (iii) patients without nail involvement at baseline. Medians reported in patients with and without nail psoriasis were compared by Mann–Whitney U test. Differences between groups with regard to frequencies were analysed by χ2 tests for independence.
Longitudinal. PASI and PGA scores over time were both studied using linear mixed models (LMM). Psoriasis severity score was defined as dependent variable, and time (in months) from baseline visit as one of the main independent variables to model psoriasis severity over time. The occurrence of nail psoriasis at baseline and the interaction term between time and nail psoriasis were other key independent variables. The latter was included to test whether psoriasis severity scores over time are different between patients with vs. without nail involvement at baseline. Sex, psoriasis severity at baseline, psoriasis duration, most intensive treatment received until first visit, concomitant anti-psoriatic treatment, presence of nail matrix involvement, presence of nail bed involvement, and presence of nail psoriasis over time, were incorporated as possible confounding factors. Confounders that altered the unadjusted exposure-outcome effect by ≥ 10% were kept in the model. Variance components were used as covariance type (default setting of SPSS). As a result of this model, psoriasis severity scores over time for patients with nail psoriasis vs. without nail psoriasis at baseline were shown in Fig. 1. Corresponding estimated marginal means (EMM) were also calculated. In case the difference in EMM reaches significance, psoriasis severity scores over time are different between the 2 groups.
Statistical package SPSS version 22.0 (IBM, Armonk, NY, USA) was used to perform all analyses. p < 0.05 was considered significant.
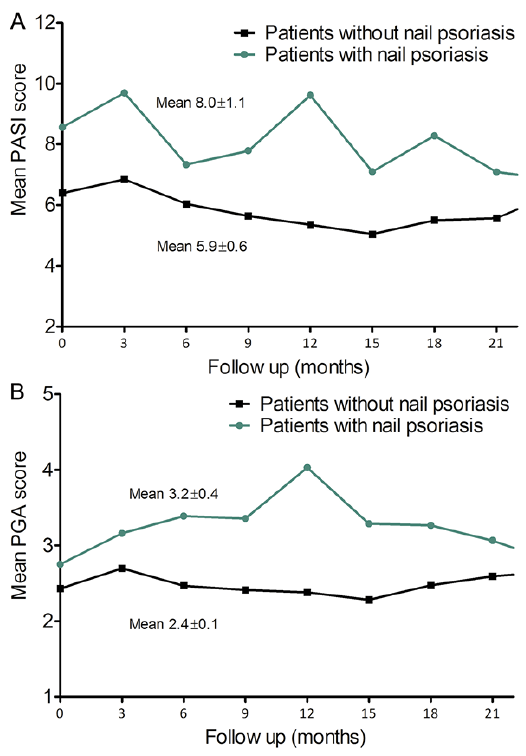
Fig. 1. Estimated psoriasis severity scores during 2-year follow-up in paediatric psoriasis patients with nail involvement (n = 65) and without nail involvement (n = 278) at baseline. (A) Mean Psoriasis Area and Severity Index (PASI) score during 2-year follow-up. (B) Mean Physician Global Assessment (PGA) score during 2-year follow-up. Linear mixed models were used to predict PASI and PGA scores over time. In both models sex, psoriasis duration and severity scores at baseline were incorporated as possible confounders.
(Graphs were presented for female subjects with a psoriasis duration of 24 months, a PASI score at baseline of 6.4 and 8.6 for subjects with and without nail psoriasis, respectively, and a PGA score at baseline of 2.43 and 2.75, respectively. Most intensive treatment received until first visit, concomitant anti-psoriatic treatment, presence of nail matrix involvement, presence of nail bed involvement and presence of nail psoriasis over time did not alter the unadjusted exposure-outcome effect by ≥10% and were therefore not kept in the model. Mean severity scores at 24 months were incorporated in our linear mixed model, but could not be presented graphically due to lower numbers at this point.).
Data from 343 de-identified patients were extracted from the ChildCAPTURE registry. Patient characteristics at baseline are shown in Table I. The majority of patients were females (58.0%) and median age and psoriasis duration were 11.0 and 1.4 years, respectively. Plaque psoriasis was the most common type of psoriasis (88.6%). Median PASI, BSA and PGA scores at first consultation were, respectively, 5.8, 5.4 and 2.0. Patients reported a median CDLQI score of 8.0. Koebnerization was observed in 78 (25.8%) patients. At baseline, 0.3% of patients were diagnosed with PsA and 3.2% had arthralgia without clinical arthritis.
Table I. Characteristics of paediatric psoriasis patients with and without nail involvement at baseline (n = 343)
A total of 65 subjects (19.0%) presented with nail psoriasis at their first visit (Table I). The median target NAPSI was 4.0. Nail psoriasis was associated with male sex (p = 0.015), concomitant higher VAS pain score (nail psoriasis 9.0 (53.0); no nail psoriasis 3.5 (20.0), p = 0.030) and more severe psoriasis. Median PASI scores in patients with and without nail involvement were, respectively, 6.5 (6.1) and 5.6 (4.7) (p = 0.033). BSA (nail psoriasis 7.0 (13.8); no nail psoriasis 5.0 (8.1), p = 0.034) and PGA (nail psoriasis 3.0 (2.0); no nail psoriasis 2.0 (1.0), p = 0.035) scores were also higher in patients with nail psoriasis. Psoriasis patients with nail involvement more often received systemic treatment at any time before their first visit (17.6 % in patients with nail psoriasis vs. 7.3% in patients without nail psoriasis, p = 0.026). All patients with palmoplantar psoriasis (n = 5) had nail psoriasis. Although total CDLQI score was slightly higher in patients with nail involvement, this effect did not reach statistical significance (p = 0.098). Number of patients with a positive Koebner phenomenon was similar between the 2 groups.
The presence of nail psoriasis during total available follow-up of all patients (n = 343; mean follow-up duration 22.9 months ± 23.6) was also captured. In total, 8.2% of patients had persistent nail psoriasis over time, and 22.1% occasionally had nail psoriasis. Most patients (69.7%) did not show signs of nail psoriasis at any time.
Longitudinal analysis of psoriasis severity scores in patients with and without nail psoriasis at baseline was performed to further investigate the role of nail psoriasis as predictor for a more severe disease course over time. LMM demonstrated an overall higher PASI score during 2-year follow-up in children with nail psoriasis compared with children without nail psoriasis at baseline (nail psoriasis at baseline, EMM 5.73 (95% confidence interval (CI) 5.00–6.46); no nail psoriasis at baseline, EMM 4.17 (95% CI 3.80–4.53), p < 0.001). This was also true for PGA scores during follow-up (nail psoriasis at baseline, EMM 2.55 (95% CI 2.35–2.76); no nail psoriasis at baseline, EMM 1.84 (95% CI 1.74–1.94), p < 0.001). Psoriasis severity scores over time are shown in Fig. 1. Results were corrected for possible confounders at baseline, including sex, psoriasis duration and psoriasis severity score at baseline. Most intensive treatment received until first visit, concomitant anti-psoriatic treatment, presence of nail matrix involvement, presence of nail bed involvement and presence of nail psoriasis over time did not alter the unadjusted exposure-outcome effect and were therefore not kept in the model. Tables II and III provide detailed information about the models used.
Table II. Linear mixed model used to estimate PASI scores during 2-year follow-up in paediatric psoriasis patients with (n = 65) and without (n = 278) nail involvement at baseline
Table III. Linear mixed model used to estimate PGA scores during 2-year follow-up in paediatric psoriasis patients with (n = 65) and without (n = 278) nail involvement at baseline
This single-centre, prospective study focused on the occurrence of nail involvement in paediatric psoriasis, epidemiological and clinical characteristics of this subpopulation, and its predicting value for a more severe disease course. Whereas conflicting results were previously reported in children, we found higher psoriasis severity scores in children with nail psoriasis within a large paediatric psoriasis population, both at baseline and during follow-up. Pourchot et al. (14) also reported more severe skin disease in children with nail psoriasis. However, psoriasis severity was defined as the use of systemic medication before or at the day of inclusion and not determined by physical examination. Mercy et al. (13) did not find an association between nail involvement and severity of skin psoriasis in 181 children aged 5–17 years, but reported that a greater proportion of children with severe psoriasis had a history of nail involvement (severe psoriasis 43.7% vs. mild psoriasis 33.3%, p = 0.300). Previous studies in children also demonstrated nail psoriasis to be present more often in boys than girls, suggesting a possible role for koebnerization in boys (13, 14). Nail psoriasis in our population was also present more frequently in boys than in girls. However, no association was found between the Koebner phenomenon and male sex by an additional χ2 test for independence (p = 0.580). Pourchot et al. (14) found a significant association between nail psoriasis and PsA (p = 0.03) in children with psoriasis. The current study did not demonstrate an association between nail psoriasis and joint involvement. However, it should be noted that only one patient (0.3%) was diagnosed with PsA in our population at baseline.
Cross-sectional analyses at baseline found nail psoriasis to be present in 19.0% of children. Piraccini et al. (12) reported an overall prevalence of 15.7% in 4,853 children and, respectively, 19.4% and 15.5% in 2 centres specialized in nail disorders in Greece and Italy. Prevalence rates in adult psoriasis are higher, which suggests an association with psoriasis duration, but this is still a matter of debate (18, 20, 21). In our population, no significant difference in psoriasis duration between patients with vs. without nail involvement was found. Moreover, almost 80% of children reported either persistent nail psoriasis (8.2%) or no signs of nail psoriasis (69.7%) during total follow-up. From a clinical perspective, the latter also suggests the presence of nail psoriasis to be a relatively stable process rather than a highly fluctuating on-off phenomenon in children. This, together with our finding that presence of nail psoriasis over time did not affect psoriasis severity scores over time, advocates nail psoriasis at baseline as a representative point in time to distinguish between having or not having nail psoriasis and assess its predictive value for a more severe disease course until 2-year follow-up.
This study is the first to show the role of nail psoriasis at baseline as a non-invasive predictor for a more severe disease course over time. Longitudinal analysis was corrected for possible confounders at baseline, including sex, psoriasis duration and psoriasis severity score at baseline. The results revealed substantially higher PASI and PGA scores during 2-year follow-up in children with clinical signs of nail psoriasis at baseline. As such, our longitudinal findings go beyond previously reported cross-sectional findings in both children and adults, and fit within the concept of early identification of patients at risk for a more severe disease course. Our study was limited by the use of the target NAPSI (0–8), in which only the most severely affected nail was scored. Further research using specific and validated nail psoriasis scoring systems of all fingernails and/or toenails is needed to further determine the role of different signs of nail psoriasis and the extent of nail involvement in predicting the severity of skin psoriasis.
Mean follow-up duration of all children in our registry was approximately 2 years at time of analysis, limiting longitudinal analysis and the subsequent role of nail psoriasis in predicting psoriasis severity to 2-year follow-up. Whether nail psoriasis is predictive for more severe disease on the long term could not be determined. In addition, onychomycosis was clinically not suspected in any of our subjects with nail psoriasis; however, nails were not cultured to confirm its absence. Finally, although nail psoriasis proved to be relative stable over time in our population, a small percentage of children without nail psoriasis at baseline still developed nail abnormalities during follow up. This may lead to underestimation of percentage of children with nail psoriasis used for longitudinal analysis.
In conclusion, nail psoriasis in children is associated with more severe psoriasis cross-sectionally, as well as a more severe disease course over time. Our findings suggest nail psoriasis to be a potential clinical predictor for a more severe disease course in the paediatric population. Therefore, nail psoriasis as a clinical predictor could assist in the prompt identification of patients at risk for a more severe disease course and subsequently result in early intervention to restrict further disease progression.
Conflict of interest statements: IMGJB has carried out clinical trials for Abbvie, Leo Pharma and Pfizer. FMB has carried out clinical trials for Janssen, Leo Pharma and Pfizer. MJvG has carried out clinical trials for AbbVie, Astellas, Leo Pharma, and Pfizer and has received speaking fees from MSD and reimbursement for attending a symposium from Pfizer and Janssen. JMMG and WK have no conflict of interests to declare. PCMvdK has carried out clinical trials for Centocor, Pfizer, Schering Plough, AbbVie, Philips Lighting, Novartis, GSK, Eli Lilly, Amgen and Almirall, and has consultancy services for Schering Plough, Celgene, Centocor, Almirall, Pfizer, AbbVie, Actelion, Galderma, Novartis, Janssen, Sandoz, Eli Lilly, Amgen and Leo pharma. All funding is not personal, but goes to the independent research fund of the Department of Dermatology of Radboud University Medical Centre Nijmegen, the Netherlands. He is past president and board member of the International Psoriasis Council and medical advisor of the International Federation of Psoriasis Patients. MCP has been a consultant for Amgen and Celgene and received unrestricted research grants from Janssen Pharmaceuticals and Pfizer. All funding is not personal, but goes to the independent research fund of the Department of Dermatology of Radboud University Medical Centre Nijmegen, the Netherlands. EMGdJ has received research grants for the independent research fund of the Department of Dermatology of Radboud University Medical Centre Nijmegen, the Netherlands from AbbVie, Pfizer, and Janssen; has acted as consultant and/or paid speaker for and/or participated in research sponsored by companies that manufacture drugs used for the treatment of psoriasis including AbbVie, Janssen, MSD, Pfizer, Novartis, Lily, and Celgene; all funding is not personal but goes to the independent research fund of the Department of Dermatology of Radboud University Medical Centre Nijmegen, the Netherlands. MMBS received grants from/was involved in clinical trials from AbbVie, Almirall, Astellas, Leo Pharma, and Pfizer and has served as a consultant for AbbVie, Almirall, Boehringer Ingelheim, Lilly, Leo Pharma and Pfizer; all funding is not personal but goes to the independent research fund of the Department of Dermatology of Radboud University Medical Centre Nijmegen, the Netherlands.
Author’s institutional review board or its equivalent (CMO): The study has been reviewed by the ethics committee on the basis of the Dutch Code of conduct for health research, the Dutch Code of conduct for responsible use, the Dutch Personal Data Protection Act and the Medical Treatment Agreement Act and does not fall within the remit of the Medical Research Involving Human Subjects Act (WMO). File number CMO: 2012/383.


 Click to show fullsize
Click to show fullsize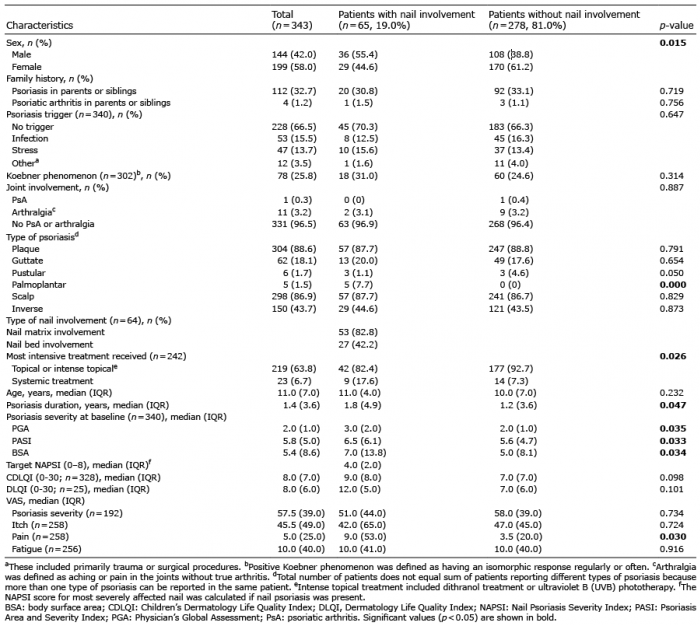 Click to show fullsize
Click to show fullsize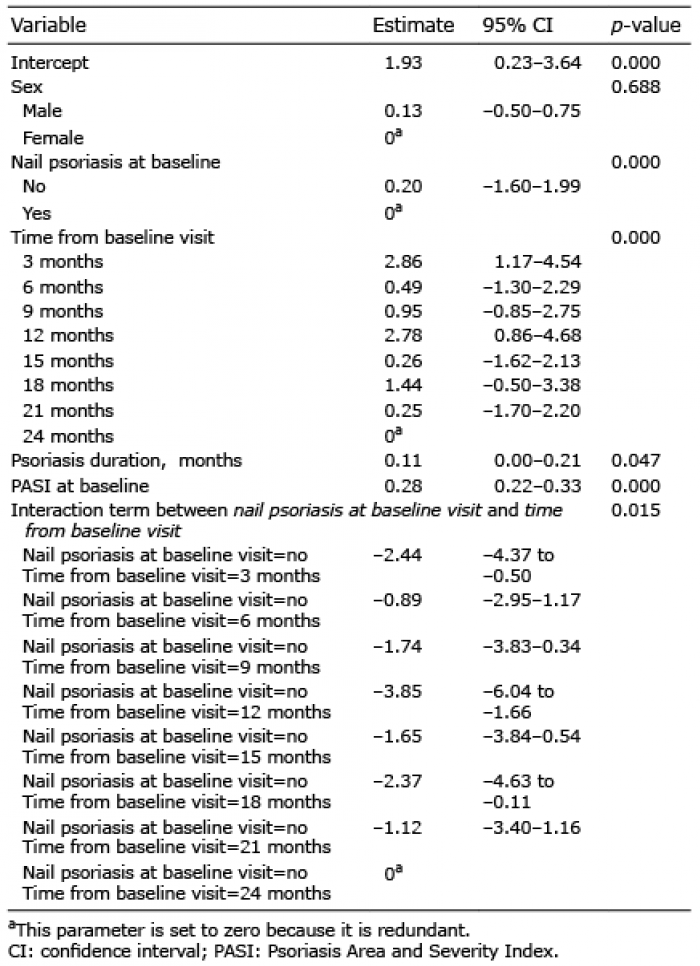 Click to show fullsize
Click to show fullsize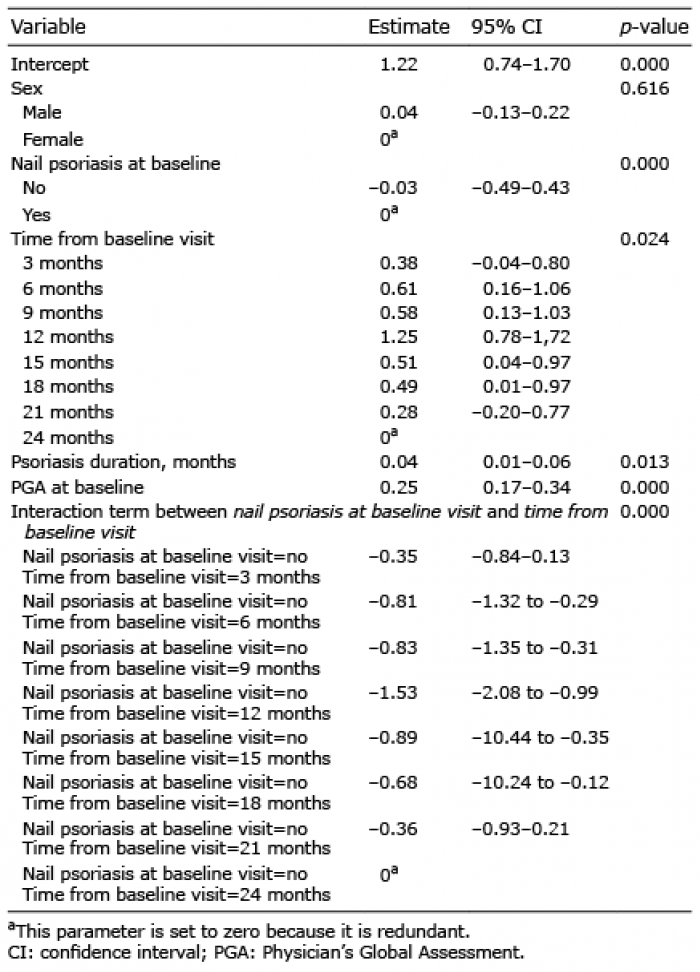 Click to show fullsize
Click to show fullsize